La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Vitasanol.com.tr
Multiple micronutrient supplementation increases the growth of Mexican infants1–4
Juan A Rivera, Teresita González-Cossío, Mario Flores, Minerva Romero, Marta Rivera, Martha M Téllez-Rojo,Jorge L Rosado, and Kenneth H BrownABSTRACT
many studies about the effect of individual micronutrients on
Background: The role of single micronutrient deficiencies in the
etiology of growth retardation has recently gained attention. How-
Supplementation trials using single micronutrients show pos-
ever, because multiple micronutrient deficiencies are common in
itive but small effects of zinc supplementation on growth. The
children in developing countries, it is possible that more than one
effects are greater in stunted children and in children with low
micronutrient may limit growth and, hence, the correction of a sin-
serum zinc concentrations (3). The results of iron supplementa-
gle deficiency may not be enough to improve growth substantially.
tion studies indicate positive effects in anemic children but
Objective: The objective was to evaluate the effect of multiple
not in nonanemic children (4–7); there appear to be few or no
micronutrient supplementation on the growth of children aged
effects of vitamin A on growth (8–10), except in children with
8–14 mo whose diets were poor in several micronutrients. Design: Children were randomly assigned to 1 of 2 groups. One
Multiple micronutrient deficiencies are common among chil-
group received a multiple micronutrient supplement containing
dren living in poverty. It is possible that more than one micronu-
the recommended dietary allowance (RDA) or 1.5 times the RDA
trient deficiency is responsible for limiting growth; therefore, the
of vitamins A, D, E, K, C, B-1, B-6, B-12, riboflavin, niacin,
correction of a single deficiency may not be enough to improve
biotin, folic acid, and pantothenic acid, and iron, zinc, iodine,
growth substantially. In experimental animals, an imbalance of
copper, manganese, and selenium. The other group received a
essential nutrients in the diet (12) or micronutrient deficiencies
placebo. Supplements were administered 6 d/wk for an average of
(13) produce anorexia, which may affect growth. It has been sug-
12.2 mo. Body length was measured at baseline and monthly
gested that latent deficiencies of other micronutrients besides
thereafter until the end of supplementation.
zinc can suppress growth after zinc repletion (14, 15). Results: Supplemented infants initially aged < 12 mo had signi-
A multiple micronutrient supplementation trial conducted in
ficantly greater length gains than did the placebo group, with a
Chinese children aged 6–9 y found positive effects of supple-
difference of 8.2 mm (length-for-age z score: 0.3) at the end of
mentation on growth (16). Children received multiple micronu-
supplementation. In contrast, differences in length gains between
trients, including zinc; multiple micronutrients without zinc; or
the supplemented and placebo groups initially aged ≥ 12 mo were
zinc only. The greatest effects occurred after treatment with the
multiple micronutrient mixture that included zinc. Notably, the
Conclusions: Micronutrient deficiencies limited the growth of the
group that received multiple micronutrients without zinc had a
Mexican infants studied. Improving micronutrient intakes should
greater growth response than did the group that received zinc
be a component of interventions to promote growth in infants liv-ing in settings where micronutrient intakes are inadequate. Am J Clin Nutr 2001;74:657–63.
1 From the Centro de Investigación en Nutrición y Salud, Instituto
Nacional de Salud Pública, Cuernavaca, Morelos, Mexico; the Departamento
KEY WORDS
de Fisiología de la Nutrición, Instituto Nacional de Ciencias Médicas y Nutri-
growth, growth retardation, micronutrient deficiencies, Mexico,
ción “Salvador Zubirán”, Mexico DF; and the Program in International Nutri-
tion and Department of Nutrition, University of California, Davis, CA.
2 Preliminary results presented as an abstract at Experimental Biology 1996
(FASEB J 1996;10:A290) and in tabular form at Experimental Biology 1998. INTRODUCTION
3 Supported by the Applied Diarrheal Disease Research Program from
Harvard University (grant 184) and by the World Health Organization (pro-
Growth retardation is highly prevalent among children in
low-income countries (1). Infections and inadequate food
4 Address reprint requests to JA Rivera, Instituto Nacional de Salud Pub-
intake are well-established causes of growth retardation; how-
lica, Avenida Universidad no. 655, Colonia Santa Maria Ahuacatitlan, CP
ever, the possible specific role of micronutrient deficiencies in
62508, Cuernavaca, Morelos, Mexico. E-mail: jrivera@insp.mx.
the etiology of growth retardation and other developmental and
health outcomes has gained attention recently. As a result,
Accepted for publication January 3, 2001. Am J Clin Nutr 2001;74:657–63. Printed in USA. 2001 American Society for Clinical Nutrition
only. The results suggest that deficiencies in micronutrients other
sium iodide), copper (as copper gluconate), manganese (as man-
than just zinc were suppressing growth.
ganese sulfate), and selenium (as selenium sulfate). The supple-
The dietary intake of children in rural areas in Mexico is defi-
ment also contained 1.2 times the RDA for children aged 1–3 y
cient in several micronutrients. A national probabilistic survey
of vitamin A (as retinyl palmitate) and 1.5 times the RDA of
conducted in 1999 found that children aged < 5 y in rural Mex-
ascorbic acid (extra fine), riboflavin, vitamin B-12, iron (as fer-
ico had low dietary intakes of iron, vitamin A, vitamin C, and
ric orthophosphate), and zinc (as zinc sulfate).
zinc relative to requirements (17). The same survey reported a
The beverages were provided to the children 6 d/wk for an
national prevalence of anemia of 27.2% in children aged < 5 y
average of 12.2 mo under supervision of the study personnel,
and almost 50% in children aged 12–23 mo. Other dietary infor-
who recorded whether the supplement was consumed.
mation suggests low intakes of vitamin B-6 and riboflavin and
community based studies in rural areas have found biochemical
Data collection
evidence of iron, zinc, vitamin A, vitamin C, and vitamin B-12
At baseline, anthropometric measures were made, morbidity
and socioeconomic (eg, education level of the parents and housing
We conducted a study to evaluate the effect of multiple micronu-
quality) data were collected, intakes of breast milk and comple-
trient supplementation on the growth of children aged 8–14 mo liv-
mentary foods were obtained by direct weighing, and information
ing in a setting where the diet is poor in several micronutrients.
about the children’s appetites was ascertained. Biochemical dataon the micronutrient status of the children were unavailablebecause most of the families considered it unacceptable to draw
SUBJECTS AND METHODS
blood from infants. After the baseline data were collected, allparticipating children (n = 337) were followed for an average of
Study sample
12.2 ± 1.8 mo. During this time, anthropometric measures were
The present study was conducted in Xoxocotla, State of
made and dietary intakes were ascertained.
Morelos, a semirural setting located 90 km south of Mexico
City, at an altitude of 930 m above sea level, with an estimatedpopulation of 16 800 inhabitants. Agriculture is the principal
Anthropometric measures were made approximately every
occupation here and the general social and economic conditions
month until the end of supplementation. Weight was measured to
are poor. Most streets are unpaved and there is no sewage sys-
the nearest 10 g with an electronic scale (model 1583; Tanita,
tem, although a water supply system is available. A study con-
Tokyo) and length was measured to the nearest millimeter with a
ducted in a random sample of 366 families in this community
locally made wooden measuring board by 2 anthropometrists
showed that 62% of the houses had dirt floors, 31% had no
who were trained to take all measurements using standard tech-
latrines or toilets, and 21% had no water supply into the house.
niques (22, 23). Technical errors of measurement (TEMs) at the
Twenty-three percent of children aged < 5 y of age were stunted
end of the standardization period were within values reported for
[length-for-age or height-for-age z score < Ϫ2 of the reference
carefully conducted studies such as the Fels Longitudinal Study
data of the World Health Organization/National Center for Health
(22). For example, the intrameasurer TEMs for the 2 anthro-
Statistics/Centers for Disease Control and Prevention (WHO/
pometrists were 0.4 and 1.1 mm for length and 90 and 110 g for
NCHS/CDC; 19)]. Most of the men in this region are either
weight. The corresponding intermeasurer TEMs were 3.6 mm for
agricultural laborers or construction workers, whereas most of
length and 136 g for weight. An experienced anthropometrist
the women sell agricultural products in local markets or work as
visited the field every other week to supervise the measuring
domestic employees in nearby cities.
techniques. Length and weight data were transformed to z scores
The research team completed a census of Xoxocotla to iden-
by using the WHO/NCHS/CDC reference data (19).
tify children aged 8–14 mo. A total of 337 children in this age
group were enrolled after written consent was obtained fromtheir parents. The study protocol was explained in detail to each
Morbidity data were collected daily at the time the supple-
family and was approved by the Committee on the Use of Human
ment was distributed. A checklist was used to record symptoms
Subjects in Research of the National Institute of Public Health.
of diarrhea and acute respiratory infection observed by the moth-ers or caretakers during the previous 24 h. The morbidity data are
Study design
The Moses-Oakford method (20) was used to randomly assign
children to 1 of 2 groups in this double-blind, placebo-controlled,supplementation trial. One group received 30 mL of a beverage
In a subsample of 163 children (87 in the micronutrient group
containing multiple micronutrients (micronutrient group) and the
and 76 in the placebo group), dietary intakes were evaluated
other received 30 mL of a placebo (placebo group). The 2 bev-
at baseline and 2–3 mo after the initial measurement. Dietary
erages were indistinguishable, both of which contained sugar
evaluations included direct weighing of all foods and beverages
and artificial flavors but no protein or fat, and provided 126 kJ
consumed during Ϸ12 h and a 24-h dietary recall questionnaire
concerning dietary intakes during the 24 h before the direct
The supplement contained the recommended dietary allowance
weighing began. Data obtained from the use of both methods
(RDA; 21) for children aged 1–3 y of the vitamins D (as chole-
were combined to give complete 24-h dietary intakes of the chil-
calciferol), E (as tocopheryl acetate), K , niacin (as nicotin-
dren. A test-weighing technique was used to measure breast-milk
amide), thiamine (as thiamine mononitrate), B-6 (as pyridoxine
consumption during the same Ϸ12-h period of direct weighing.
hydrochloride), D-biotin, folic acid, and pantothenic acid (as
Breast-milk consumption during the day was extrapolated to 24 h,
D-calcium pantothenate) and of the minerals iodine (as potas-
assuming that children were breast-fed during the night, by using
a prediction equation derived from a study of Peruvian infants
z score, which was determined monthly during supplementation,
(24). The test-weighing data were not corrected for insensible
and the same independent variables used in the first set, except
water loss, which amounts to 0.03–0.05 g · kgϪ1 · minϪ1 (25, 26).
that the baseline length-for-age z score was used instead of base-
Therefore, our values for breast-milk intake were underestimated
line length. GEE models were also used to test for two-way
by 1–5% (27). Energy and nutrient intakes were derived by using
interactions between treatment and sex, treatment and age at
a food-composition database compiled by our group that used
baseline, and treatment and period of supplementation.
3 different data sources. The main source was the food-composition
Probability values < 0.05 were considered statistically signifi-
database of the Instituto Nacional de Ciencias Médicas y Nutri-
cant for main effects and < 0.10 for interactions (32, 33). All statis-
ción “Salvador Zubirán” (the Mexican database).
tical analyses were performed by using STATA (release 6.0, Stata
This database was complemented with data from the US
Statistical Software, Stata Corporation, College Station, TX).
Department of Agriculture (28) and from the Institute of Nutri-tion of Central America and Panama (Guatemala City,Guatemala) for nutrients or foods not available in the Mexican
database. The composition of breast milk from healthy US
Compliance rates relative to the total projected days of sup-
women (29) was used to derive energy and nutrient intakes from
plementation were 80.5% in the placebo group and 91% in the
the breast milk consumed in the present study.
supplemented group (P < 0.05). Of the 337 children originallyrecruited (n = 169 in the micronutrient group and 168 in the
placebo group), 18 (n = 8 in the micronutrient group and 10 in
Information about the participants household characteristics
the placebo group) had missing anthropometric information;
(eg, type of floor, presence of toilet, and kitchen in a bedroom),
therefore, 319 children (n = 161 in the micronutrient group and
the possession of selected household goods (eg, radio, television,
158 in the placebo group) were included in the analysis. Baseline
blender, and refrigerator), and the education level of the parents
characteristics of the children, their parents, and their house-
was obtained by interviewing the mothers of the participating
holds by treatment group are presented in Table 1 according to
children. An indicator of housing conditions was derived by the
the age of the children at baseline: < 12 mo (infants) and ≥ 12 mo.
first component obtained by principal components analysis (30).
In the children aged ≥ 12 mo, there were no significant differ-
Only variables with factor loadings > 0.5 were maintained in the
ences in any of the variables between treatment groups. In the
model (ie, house and floor material and availability of piped
infants, the average weight of children in the placebo group was
water and a sewer system). The component explained 51.3% of
260 g less than that of children in the micronutrient group
the total variance. The resulting factor scores, which have a mean
(P < 0.05). However, all other variables, including baseline
of 0 and an SD of 1, were used as a continuous variable [the
length, age, and anthropometric indexes, were not significantly
socioeconomic status (SES) score]. In addition, the factor scores
were divided into tertiles, which were further used to construct a
In the children aged ≥ 12 mo, the proportion of households
with the kitchen in a bedroom was significantly greater in theplacebo than in the micronutrient group. No other variables were
Data analysis
significantly different between treatment groups.
Baseline characteristics of the study children, their mothers,
The mean dietary intake of iron ranged from 2.12 to 2.85 mg,
and their families were compared between treatment groups by
of zinc ranged from 2.63 to 3.13 mg, and of vitamin A from
using Student’s t tests for continuous variables and chi-square tests
506 to 660 g retinol equivalents in the total population. Protein
for categorical variables to identify potential confounding factors.
intakes were > 20 g in all groups and energy intakes were
Taking advantage of the repeated-measures design of the
between 2804 and 3210 kJ/d. Differences between treatment
study, we analyzed the data by using generalized estimating
equations (GEEs). This technique is used for the analysis of lon-
Changes in anthropometric measurements from baseline to
gitudinal data that are an extension of the generalized linear
the end of supplementation are presented in Table 2 by treatment
models, which were specially developed to account for the auto-
group according to the age of the children at baseline. In the chil-
correlation due to serial measurements (31), and allows the use
dren aged ≥ 12 mo, there were no significant differences in age
of time-dependent covariates, giving the regression coefficients
or in the anthropometric variables between treatment groups.
the usual interpretation. The assumption of Gaussian distribution
Infants in the micronutrient group were an average of 0.7 cm
of the outcome variables (length and length-for-age z score) were
taller (P < 0.05) and had a length-for-age z score 0.33 units
supported by an exploratory analysis of the empirical distribu-
higher (P < 0.05) than children in the placebo group. None of the
tion of the variables. An exchangeable correlation structure that
other variables differed significantly by treatment group between
baseline and the end of supplementation.
Two sets of GEE models were used to test the effect of treat-
A GEE model for the assessment of effects of multiple
ment on length. The first set used the dependent variable length,
micronutrient supplementation on linear growth was first tested
which was measured monthly from the first to the last month
for all ages combined (data not shown). An interaction term
of supplementation, and the independent variables treatment
between treatment and age was significant (P < 0.10), indicating
(micronutrients or placebo), baseline length, SES score, and sex,
that the effect of treatment was greater in the younger than in the
which were fixed; weight-for-length z score, age, and breast-
older age group. Therefore, results are presented separately for
feeding status, which were measured monthly from the first to
the children aged < 12 mo and for those aged ≥ 12 mo.
the last month of supplementation; and an indicator variable for
Results of the use of GEEs to determine the effects of micro-
the first to the fourth 3-mo periods of supplementation. The second
nutrient supplementation on length are shown in Table 3 and
set of GEE models used the dependent variable length-for-age
Figure 1 and on length-for-age z scores in Figure 2. The main TABLE 1 Baseline characteristics of the children, their parents, and their households by age1 1 n in brackets. 2 x– ± SD. 3 Significantly different from the micronutrient group, P < 0.05 (two-tailed t test). 4 Daily intake, including breast milk. 5 Subsample for dietary study.
effect of treatment and the interaction between treatment and
that had length-for-age z score as the dependent variable (data
period of supplementation were significant in the children aged
not shown). Results indicate that girls benefited more from sup-
< 12 y for both length and length-for-age z score, indicating
that the effect of supplementation on linear growth increased
The magnitude of the differences in attained length between
as the duration of supplementation increased in this group. In
the micronutrient and placebo groups by period of supplemen-
contrast, the main effect of treatment and the interaction
tation, after adjustment for potential confounders, are presented
between treatment and the indicator variables were not signi-
separately for the 2 age subgroups in Figure 1. In the infants,
ficant for length in any of the 3-mo periods of supplementa-
micronutrient supplementation had a positive effect on length
tion in the children aged ≥ 12 mo; however, the interaction
gain, which increased from 2.6 mm at the end of the first 3-mo
between treatment and period of supplementation was signifi-
period to 8.3 mm at the end of the fourth 3-mo period of sup-
cant for length-for-age z score only in the second and third
plementation. Most of the length gain (7.9 mm) occurred during
the first 3 periods of supplementation. In children aged ≥ 12 mo,
During data analysis, a differential response between sexes
differences between the micronutrient and placebo groups were
emerged; therefore, an interaction between sex and treatment
smaller and were not significant. At the end of supplementation,
was formally tested and it was significant (P < 0.10) in both the
children aged ≥ 12 mo in the micronutrient group were on aver-
model that had length as the dependant variable and in the model
age only 2.0 mm taller than the children in the placebo group. TABLE 2 Changes in anthropometric measurements and indexes from baseline to the end of supplementation in the micronutrient and placebo groups by age categories at baseline1 1 x– ± SD. 2 Significantly different from the micronutrient group, P < 0.05 (one-tailed t test).
overall length gain that was almost 5 mm (length-for-age z score:
Results of the use of generalized estimation equations to determine the
0.19) greater than the gain in the placebo group. The effect of
effect of multiple micronutrient supplementation on length by 3-mo
supplementation was greater in infants than in the children aged
periods of supplementation, adjusted for covariates
≥12 mo. In the younger age group, supplementation resulted in
an increase in length of 8.3 mm and in the length-for-age z score
of 0.3 units. In the infants, the length-for-age z score decreasedduring follow-up by
Ϸ0.1 units in the micronutrient group and
by Ϸ0.4 units in the placebo group. In contrast, in the children
aged ≥ 12 mo, the micronutrient group gained only 2.0 mm more
in length (a greater length-for-age z score of
placebo group after 12 mo of supplementation.
Compared with other supplementation trials, the observed
effect on the infants in the present study was not only significant
but was interpreted as biologically important given that the mean
baseline length-for-age z score of the study children was Ϫ1.3,
that macronutrients were not administered, and that the study
lasted only 1 y. For example, a well-controlled supplementary
feeding trial that provided a beverage with both macronutrients
and micronutrients to Guatemalan children for almost 3 y (from
3 to 36 mo of age) resulted in a cumulative effect of 2.5 cm in length
1 Micronutrient = 1, placebo = 0. 2
(34), Ϸ3 times the size of the effect observed in the present trial;
however, most of the effect of supplementary feeding occurred dur-
ing the first 2 y of life (35). In addition, the median length-for-age
Low tertile = 1, medium and high tertiles = 0. 5 Three-month periods of supplementation. z scores in the Guatemalan infants was less than Ϫ2 before supple-mentation (36), a value that is well below the median values in thepresent study. It is well known that the closer the z score is to 0, the
The magnitude of the differences in length-for-age z scores
less likely it is to detect any effect on linear growth.
between the micronutrient and placebo groups by period of sup-
The effects of micronutrient supplementation on length in the
plementation, after adjustment for potential confounders, are
infants in the present study were greater than those shown in a
presented separately for the 2 age subgroups in Figure 2. Length-
meta-analysis of zinc supplementation trials (3). In contrast, the
for-age z scores increased from 0.12 to 0.30 units from the first to
effects on older children, although statistically significant for
the fourth 3-mo periods of supplementation in the infants. As was
some 3-mo periods of supplementation, were small compared with
the case for length, most of the effect (0.29 units) was achieved
the effects of other interventions involving supplementary feeding
during the first 3 periods of supplementation. In children aged
or zinc supplementation. The finding of greater effects in infants
≥12 mo, adjusted differences between treatment groups were
than in older children is biologically plausible. Infants grow at
smaller than those for the children aged < 12 mo. At the end of the
faster rates than do older children, their micronutrient needs to
fourth 3-mo period of supplementation, the adjusted differences
sustain this accelerated growth are greater, and their diets are often
between treatment groups were 0.10 z score units (P < 0.10).
more restricted than those of older children. As mentioned previ-ously, most of the effect of supplementary feeding occurs duringthe first year of life (35); therefore, we had expected larger effects
DISCUSSION
on younger children at the time the study was designed.
Administration of a multiple micronutrient supplement 6 d/wk
Moreover, it is possible that the effects of supplementation
for Ϸ12 mo to children aged 8–14 mo at baseline resulted in an
would have been greater if the infants had been admitted to the
FIGURE 1. Differences in length between the micronutrient and placebo groups (micronutrient Ϫ placebo) adjusted for length at baseline, weight-
for-length z score at baseline, monthly breast-feeding status, sex, and socioeconomic status. *Significantly different from 0, P < 0.05. FIGURE 2. Differences in length-for-age z scores between the micronutrient and placebo groups (micronutrient Ϫ placebo) adjusted for length-
for-age z score at baseline, weight-for-length z score at baseline, monthly breast-feeding status, sex, and socioeconomic status. *Significantly differ-ent from 0, P < 0.05.
study at a younger age. The mean length of our study children at
the children in the present study. However, the mean total protein
baseline was already 1.3 SDs below the reference mean. The
intake was 30–40% greater than recommended amounts (21) and
mean length in the placebo group 1 y later was 0.25 SDs lower.
human and cow milk were the main protein sources, indicating
Therefore, potentially, a greater effect could have been achieved
that the protein consumed was generally of high quality. In con-
in younger children. We did not include children aged < 8 mo
trast, iron and zinc intakes were well below recommendations
because we were also interested in evaluating the effects of sup-
(21). Our results corroborate that micronutrients were a limiting
plementation on appetite and behavior, which were considered
dietary factor in the population studied.
easier to evaluate at older ages. Future studies should start sup-
The finding that girls benefited more from supplementation
than did boys, based on the effects of the interaction between sex
It is highly likely that the differences in linear growth between
and treatment on length, should be interpreted with caution
the micronutrient and the placebo groups was due to supplementa-
because sex was an unplanned comparison. Moreover, many vari-
tion because our study was randomized and double-blind, the
ables, including length-for-age z score, were significantly differ-
supplements were administered to all children 6 d/wk under super-
ent between treatment groups within sexes at baseline because
vision, and the supplements were well accepted as reflected by the
randomization was not stratified by sex. We recommend that
high compliance rate; on average, the supplements were consumed
future studies investigate this association.
on 86% of the scheduled days. Because the anthropometric indexes
Breast-feeding was negatively associated with linear growth
at baseline, most of the anthropometric measures made during the
in this analysis, however, this finding may have been due to neg-
study period, and other characteristics of the children and their
ative confounding. In poor rural and semirural settings in Mex-
families at baseline were similar between treatment groups, we
ico, such as the site in the present study, more educated women
considered randomization to have been effective (Table 1).
and those who work out of home tend to breast-feed less but live
Our results indicate that growth was stimulated in the infants in
in better conditions, which in turn is associated with better
the first 3 mo of supplementation and continuation of supplemen-
growth. In addition, anthropometric measures tend to be smaller
tation yielded ongoing positive effects on growth for at least
in breast-fed than in bottle-fed infants (40).
9 mo. Additional studies are needed to measure growth responses
The results of our study show that micronutrients are a limit-
when supplementation is begun at younger ages and continued for
ing factor for the growth of infants in Mexico and that public
health interventions aimed at improving the nutritional status
We had hypothesized that children who were more stunted at
and growth of infants and young children should consider
baseline would benefit more from supplementation than would
improvements in micronutrient intakes as an essential compo-
less-stunted children, as was observed in a zinc supplementation
nent. In addition, infants should be targeted in interventions
trial in Guatemalan children (37). However, the interaction
aimed at promoting growth through improvements in micronu-
between degree of initial stunting and treatment was not signifi-
cant. It is possible that the lack of an interaction between treat-ment and the degree of stunting was because the degree of stunting
REFERENCES
in the group studied was not as severe as in other studies. Forexample, the average baseline length-for-age z score in our zinc
1. Administrative Committee on Coordination/Sub-committee on
Nutrition. Fourth Report on the world nutrition situation. Geneva:
supplementation trial in Guatemala was Ϫ2.11 compared with
ACC/SCN in collaboration with IFPRI, 2000.
1.3 in the present study, despite the fact that the Guatemalan
2. Allen LH. Nutritional influences on linear growth: a general review.
children were younger (average age at baseline: 7.5 mo) than the
children in the present study (11.2 mo).
3. Brown KH, Peerson JM, Allen LH. Effect of zinc supplementation
The energy intakes of the micronutrient and placebo groups
on children’s growth: a meta-analysis of intervention trials. Bibl Nutr
were well within the requirements (38, 39) for the age groups of
4. Auckett MA, Parks YA, Scott PH, Wharton BA. Treatment with iron
20. Meinert CL, Tonascia S. Clinical trials. Design, conduct and analy-
increases weight gain and psychomotor development. Arch Dis
sis. New York: Oxford University Press, 1968:95–112.
21. National Research Council. Recommended dietary allowances.
5. Bhatia D, Seshadri S. Growth performance in anemia and following
10th ed. Washington, DC: National Academy Press, 1989.
iron supplementation. Indian Pediatr 1993;30:195–200.
22. Lohman T, Roche A, Martorell R. Anthropometric standardization
6. Chwang LC, Soemantri AG, Pollitt E. Iron supplementation and
reference manual. Chicago: Human Kinetics, 1988.
physical growth of rural Indonesian children. Am J Clin Nutr 1988;
23. Habicht JP. Estandarización de métodos epidemiológicos cuantita-
tivos sobre el terreno. (Standardization of quantitative epidemiologic
7. Lawless JW, Latham MC, Stephenson LS, Kinoti SN, Pertet AM. Iron
methods in the field.) Bol Oficina Sanit Panam 1974;76:375–84
supplementation improves appetite and growth in anemic Kenyan pri-
mary school children. J Nutr 1994;124:645–54.
24. de Kanashiro HC, Brown KH, López de Romaña G, Lopez T, Black RE.
8. Ramakrishnan U, Martorell R. The role of vitamin A in reducing
Consumption of food and nutrients by infants in Huascar (Lima),
child mortality and morbidity and improving growth. Salud Publica
Perú. Am J Clin Nutr 1990;52:995–1004.
25. Dewey KG, Heinig MJ, Nommsen LA, Lonnerdal B. Maternal ver-
9. West KP Jr, Djunaedi E, Pandji A, et al. Vitamin A supplementation
sus infant factors related to breast milk intake and residual milk vol-
and growth: a randomized community trial. Am J Clin Nutr 1988;
ume: the DARLING study. Pediatrics 1991;87:829–37.
26. Hendrikson EC, Seacat JM, Neville MC. Insensible weight loss in
10. Muhilal, Permeisih D, Idjradinata YR, Muherdiyantiningsih, Karyadi D.
children under one year of age. Acta Paediatr 1985;74:678–80.
27. Brown KH, Black RE, Robertson AD, Akhtar NA, Ahmed G,
Vitamin A–fortified monosodium glutamate on health, growth, and
Becker S. Clinical and field studies of human lactation: method-
survival of children: a controlled field trial. Am J Clin Nutr
ological considerations. Am J Clin Nutr 1982;35:745–56.
28. US Department of Agriculture, Agricultural Research Service.
11. Sommer A, West KP Jr. Consequences of vitamin A deficiency: child
USDA nutrient database for standard reference, release 13. Beltsville,
survival. In: Sommer A, West KP Jr, Olson JA, Ross CA, eds. Health,
MD: USDA Nutrient Data Laboratory, 1999.
survival, and vision. New York: Oxford University Press, 1996.
29. National Academy of Sciences. Nutrition during lactation. Washing-
12. Golden BE, Golden MHN. Relationship among dietary quality, chil-
ton, DC: Institute of Medicine, National Academy Press, 1991:116.
dren’s appetites, growth stunting, and efficiency of growth in poor
30. Kleinbaum DG, Kupper LL, Muller KE. Applied regression analy-
populations. Food Nutr Bull 1991;3:105–9.
sis and other multivariate methods. Boston: PWS-Kent PublishingCo, 1988:595–641.
13. Wallwork JC, Fosmire GJ, Sanstead HH. Effect of zinc deficiency
31. Diggle PJ, Liang KY, Zeger SL. Analysis of longitudinal data.
on appetite and plasma amino acid concentrations in the rat. Br J
Oxford, United Kingdom: Clarendon Press, 1996. (Oxford Statisti-
14. Carter JP, Grivetti LE, Davis JT, et al. Growth and sexual develop-
32. Cohen J. Statistical power analysis for the behavioral sciences. Rev
ment of adolescent Egyptian village boys. Effects of zinc, iron, and
ed. New York: Academic Press, 1977:1–292.
placebo supplementation. Am J Clin Nutr 1969;22:59–78.
33. Hosmer DW, Lemeshow S. Applied logistic regression. New York:
15. Ronaghy HA, Reinhold JG, Mahloudji M, Ghavami P, Fox MR,
John Wiley & Sons, 1989:82–133.
Halsted JA. Zinc supplementation of malnourished schoolboys in
34. Habicht JP, Martorell R, Rivera JA. Nutritional impact of supple-
Iran: increased growth and other effects Am J Clin Nutr 1974;27:
mentation in the INCAP longitudinal study: analytic strategies andinferences. J Nutr 1995;125:1042S–50S.
35. Schroeder DG, Martorell R, Rivera JA, Ruel MT, Habicht J-P. Age
16. Sandstead HH, Penland JG, Alcock NW, et al. Effects of repletion
differences in the impact of nutritional supplementation on growth.
with zinc and other micronutrients on neuropsychologic perfor-
mance and growth in Chinese children. Am J Clin Nutr 1998;
36. Rivera JA, Habicht J-P. The recovery of Guatemalan children with
mild to moderate wasting: factors enhancing the impact of supple-
17. Instituto Nacional de Salud Pública. Encuesta Nacional de Nutrición
mentary feeding. Am J Public Health 1996;86:1430–4.
1999. Tomo I. Niños menores de cinco años. (National nutrition sur-
37. Rivera JA, Ruel MT, Santizo MC, Lönnerdal B, Brown KH. Zinc
vey 1999. Vol 1. Children under five years of age.) Cuernavaca, Méx-
supplementation improves the growth of stunted rural Guatemalan
ico: Instituto Nacional de Salud Pública, 2000 (in Spanish).
38. Bute NF. Energy requirements of infants. Eur J Clin Nutr 1996;50:
18. Rivera J, Bourges H, Arroyo P, et al. Deficiencias de mirconutrimen-
tos. (Micronutrient deficiencies.) In: De la Fuente JR, Sepúlveda J,
39. Torún B, Davis PSW, Livingstone MBE, Paolisso M, Sackett R, Spurr GB.
eds. Diez problemas relevantes de salud pública en México. (Ten rel-
Energy requirements and dietary energy requirements for children and
evant public health problems in México.) México DF: Fondo de Cul-
adolescents 1 to 18 years old. Eur J Clin Nutr 1996;50:S37–81.
40. World Health Organization. Physical status: the use and interpreta-
19. World Health Organization. Measurement of nutritional impact.
tion of anthropometry. World Health Organ Tech Rep Ser 1995;845:
Herzl Family Practice Centre, Goldfarb Breastfeeding Clinic Domperidone Patient Handout What is domperidone? Domperidone is a pill that can increase breastmilk by increasing your levels of prolactin(the hormone responsible for milk production). This pill was originally developed for stomach problems such as reflux and nausea. However, it is now bein
COMISIÓN INTERAMERICANA PARA EL CONTROL DEL ABUSO DE DROGAS REGLAMENTO MODELO SOBRE DELITOS DE LAVADO DE ACTIVOS RELACIONADOS CON EL TRÁFICO ILÍCITO DE DROGAS, Y Incluye las modificaciones introducidas por el Grupo de Expertos para el Control de Lavado de Activos en Chile, en octubre de 1997, en Estados Unidos de América, en mayo de 1998, en Argentina, en octubre de 1988, en Méx
 Multiple micronutrient supplementation increases the growth of Mexican infants1–4
Juan A Rivera, Teresita González-Cossío, Mario Flores, Minerva Romero, Marta Rivera, Martha M Téllez-Rojo,Jorge L Rosado, and Kenneth H Brown
ABSTRACT
Multiple micronutrient supplementation increases the growth of Mexican infants1–4
Juan A Rivera, Teresita González-Cossío, Mario Flores, Minerva Romero, Marta Rivera, Martha M Téllez-Rojo,Jorge L Rosado, and Kenneth H Brown
ABSTRACT only. The results suggest that deficiencies in micronutrients other
sium iodide), copper (as copper gluconate), manganese (as man-
than just zinc were suppressing growth.
only. The results suggest that deficiencies in micronutrients other
sium iodide), copper (as copper gluconate), manganese (as man-
than just zinc were suppressing growth. a prediction equation derived from a study of Peruvian infants
z score, which was determined monthly during supplementation,
(24). The test-weighing data were not corrected for insensible
and the same independent variables used in the first set, except
water loss, which amounts to 0.03–0.05 g · kgϪ1 · minϪ1 (25, 26).
a prediction equation derived from a study of Peruvian infants
z score, which was determined monthly during supplementation,
(24). The test-weighing data were not corrected for insensible
and the same independent variables used in the first set, except
water loss, which amounts to 0.03–0.05 g · kgϪ1 · minϪ1 (25, 26). TABLE 1
TABLE 1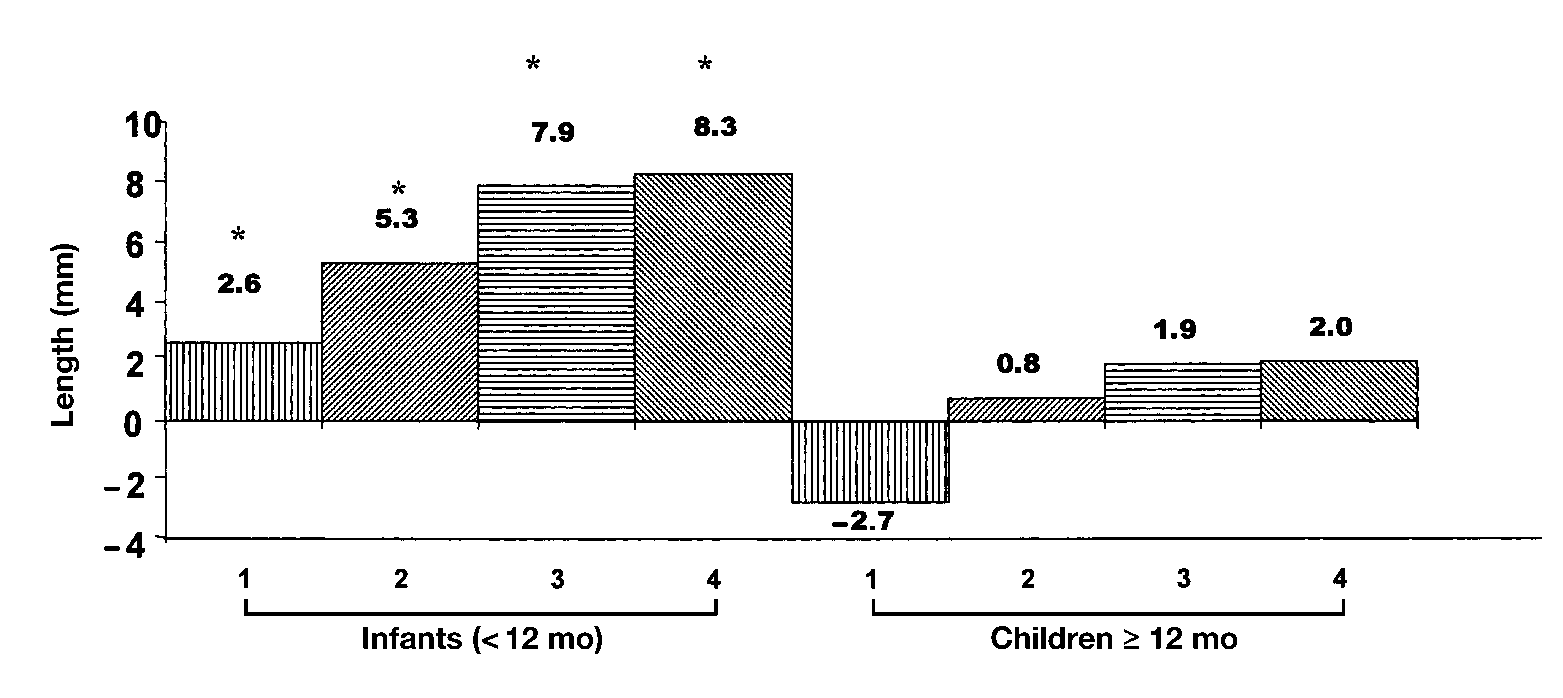
 overall length gain that was almost 5 mm (length-for-age z score:
Results of the use of generalized estimation equations to determine the
0.19) greater than the gain in the placebo group. The effect of
effect of multiple micronutrient supplementation on length by 3-mo
supplementation was greater in infants than in the children aged
periods of supplementation, adjusted for covariates
≥12 mo. In the younger age group, supplementation resulted in
an increase in length of 8.3 mm and in the length-for-age z score
of 0.3 units. In the infants, the length-for-age z score decreasedduring follow-up by
Ϸ0.1 units in the micronutrient group and
by Ϸ0.4 units in the placebo group. In contrast, in the children
aged ≥ 12 mo, the micronutrient group gained only 2.0 mm more
in length (a greater length-for-age z score of
placebo group after 12 mo of supplementation.
overall length gain that was almost 5 mm (length-for-age z score:
Results of the use of generalized estimation equations to determine the
0.19) greater than the gain in the placebo group. The effect of
effect of multiple micronutrient supplementation on length by 3-mo
supplementation was greater in infants than in the children aged
periods of supplementation, adjusted for covariates
≥12 mo. In the younger age group, supplementation resulted in
an increase in length of 8.3 mm and in the length-for-age z score
of 0.3 units. In the infants, the length-for-age z score decreasedduring follow-up by
Ϸ0.1 units in the micronutrient group and
by Ϸ0.4 units in the placebo group. In contrast, in the children
aged ≥ 12 mo, the micronutrient group gained only 2.0 mm more
in length (a greater length-for-age z score of
placebo group after 12 mo of supplementation.
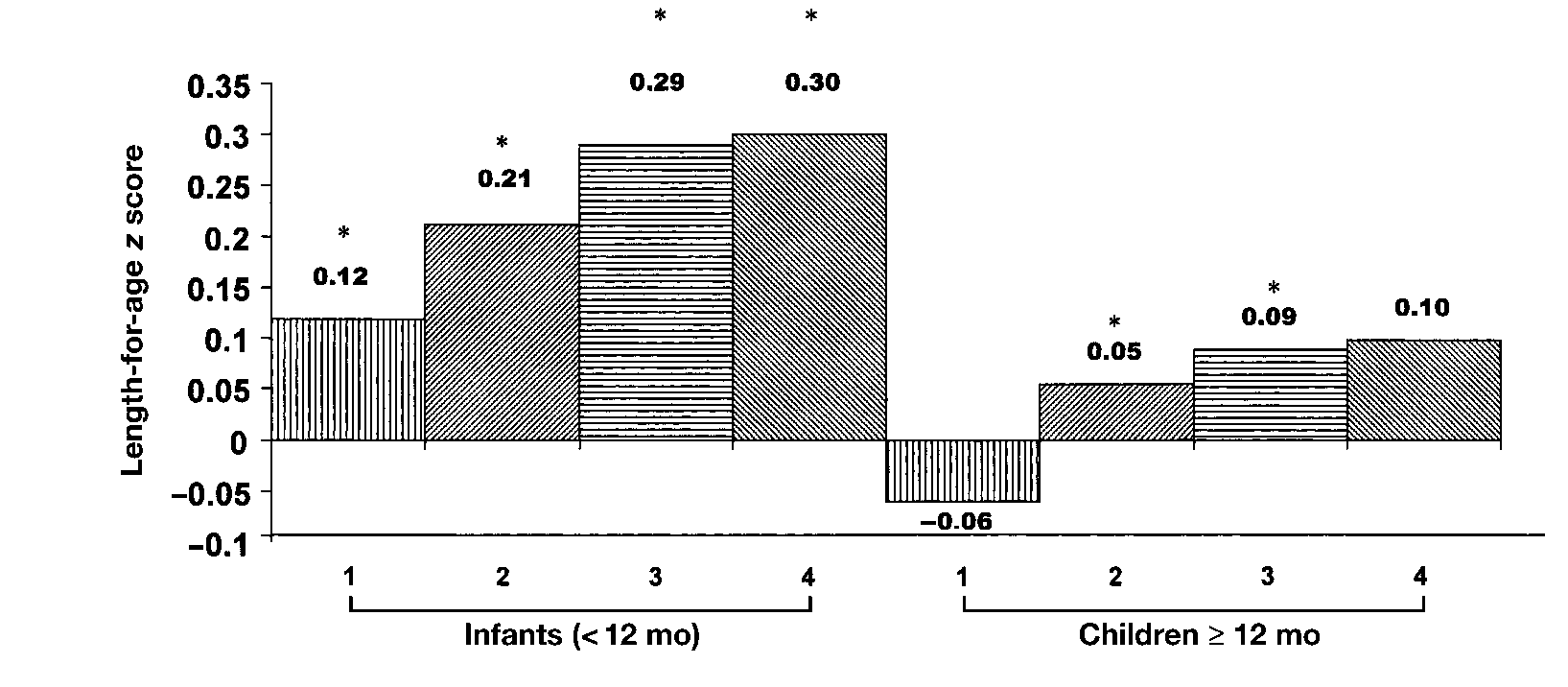
 FIGURE 2. Differences in length-for-age z scores between the micronutrient and placebo groups (micronutrient Ϫ placebo) adjusted for length-
FIGURE 2. Differences in length-for-age z scores between the micronutrient and placebo groups (micronutrient Ϫ placebo) adjusted for length- 4. Auckett MA, Parks YA, Scott PH, Wharton BA. Treatment with iron
20. Meinert CL, Tonascia S. Clinical trials. Design, conduct and analy-
increases weight gain and psychomotor development. Arch Dis
sis. New York: Oxford University Press, 1968:95–112.
4. Auckett MA, Parks YA, Scott PH, Wharton BA. Treatment with iron
20. Meinert CL, Tonascia S. Clinical trials. Design, conduct and analy-
increases weight gain and psychomotor development. Arch Dis
sis. New York: Oxford University Press, 1968:95–112.