La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Vejigadolorosa.com.ar
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609 A c t a s U r o l ó g i c a s E s p a ñ o l a s Original – Prostate cancer Practical treatment approach in radiation- induced cystitis R. Martínez-Rodríguez, J. Areal-Calama, O. Buisan-Rueda, C. González-Satue, J. Sanchez-Macias, M. Arzoz-Fabregas, J. Gago-Ramos, S. Bayona-Arenas, L. Ibarz- Servio and J.M. Saladié-Roig Department of Urology, Germans Trias i Pujol Hospital, Badalona, Spain Practical treatment approach in radiation-induced cystitis
Received 30 November 2009; accepted 1 March 2010
Objective: Establish a pattern of behavior and treatment algorithm at the onset of
hematuria in patients with a previous history of pelvic radiation, checking for this
different treatment options reflected in the literature.
Material and methods: Through performing a PubMed literature review of articles
related to IC lies, searching items includes the different treatment options:
intravesical hyaluronic acid, conjugated estrogens, pentosan polysulfate, oral
Cáncer de próstata Guía de tratamiento
aminocaproic acid, recombinant factor VIIa, hyperbaric chamber, embolization,
aluminum intravesical, Helmstein ball and formalin. Limits the search to English or
Spanish publications and excluding those related to animal experimentation.
Results: Every option is exposed, referring to the physiopathology, dosage regimen
and administration, side effects and treatment efficacy.
Conclusions: Once patient hemodynamic stabilization is achieved, and after rule out
bladder tumors injuries and /or haemathuria originating from the upper urinary tract,
treatment should start rolling. To know different treatment options and patterns of
administration will allow the urologist to obtain a higher rate of success in the
2009 AEU. Published by Elsevier España, S.L. All rights reserved.
Keywords: Radiation-induced cystitis Haemathuria Radiotherapy Prostate cancer Treatment guide
E-mail: dr.rmartinez@yahoo.es (R. Martínez-Rodríguez).
0210-4806/$ - see front matter & 2009 AEU. Published by Elsevier Españ a, S.L. All rights reserved. doi:10.1016/j. acuro.2010.03.005
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609
The chronic phase in turn begins 6 months after radiotherapy. The
Introduction
effect of radiation upon the bladder wall leads to ischemia, which in turn
conditions changes at vascular and muscle level. Vascular endothelial
When the bladder is exposed to radiation in the context of radiotherapy
damage causes hyperplasia, occlusion and perivascular fibrosis. Muscle
for pelvic tumors, a series of histopathological changes are induced that
damage in turn causes smooth muscle fiber replacement by fibroblasts,
in turn have clinical consequences. In addition to irritative micturition
leading to fibrosis and a secondary reduction in bladder capacity and
syndrome characterized by micturition urgency, pollakiuria and dysuria,
compliance1. Both alterations increase bladder susceptibility to mucosal
the appearance of hematuria of highly variable intensity represents one
ulceration and bleeding, and even bladder perforation and the formation
of the most complex complications which the urologist must deal with.
The present article offers a succinct review of the available treatment
options for radiation-induced cystitis, with the purpose of facilitating its
practical management on the part of the urologist.
Specifically, the aim of the study is to establish an intervention protocol
Patient evaluation
and define a diagnostic algorithm capable of facilitating patient
Patients with radiation-induced cystitis can develop clinical
manifestations ranging from asymptomatic microhematuria to
macrohematuria with clots and secondary urinary retention. Despite the
Material and methods
establishment of a presumed diagnosis on the basis of the patient condition, it is always necessary to discard possible infections and/or
A PubMed literature search was made of articles related to actinic or
Urinary infection can exacerbate hematuria produced in the context of
radiation-induced cystitis. The search keywords included those referred
to the different treatment options: systemic, endovesical and/or physical
Radiotherapy for ovarian or cervical cancer increases the risk of
treatment procedures. These comprised the following: endovesical
bladder cancer 2- to 4-fold, and males subjected to radiotherapy for
hyaluronic acid, conjugated estrogens, pentosan polysulfate, oral
prostate cancer have a 50% increased risk of developing bladder cancer3.
aminocaproic acid, recombinant factor VIIa, hyperbaric chamber,
The exclusion of bladder neoformations based on urethrocystoscopy
and/or urinary cytology is mandatory in cases of macroscopic hematuria.
formalinization. The terms actinic and radioinduced were also
Endoscopy moreover offers an endoluminal view with characteristic
No limits were applied in terms of the date of publication or the
If hematuria persists despite continuous bladder irrigation and
endovesical coagulation of the bleeding lesions, hemodynamic
The search was limited to publications in Spanish and English, and
stabilization of the patient is the objective to be pursued. With the
animal experimentation studies were excluded. The level of scientific
patient under stable conditions, the management best suited to each
evidence was added corresponding to each of the options according to
individual case should be considered, among the range of options
the current classification, published in the clinical practice guides of the
Ia: The evidence comes from metaanalyses of well designed,
Treatment options
Ib: The evidence comes from at least one randomized, controlled trial.
IIa: The evidence comes from at least one well designed,
There is no definitive treatment for severe hemorrhagic cystitis. A
number of management options must be considered, and there is a range
IIb: The evidence comes from at least one well designed, quasi-
of possible combinations4. The most widespread management options
are indicated below, with a brief comment on their form of
I I I : The evidence comes from well designed, non-experimental
administration, efficacy and possible side effects.
descriptive studies such as comparative studies, correlation studies or
I V : The evidence comes from documents or opinions of expert
committees, or clinical experiences of authorities of prestige.
Histopathological considerations
The histopathological changes after radiation exposure occur in two
phases: acute and chronic. The acute and subacute phases are observed
between 3-6 months after treatment. Histopathologically, urothelial
desquamation, atypias and eosinophilic infiltrates have been described1.
Clinically, patients may experience micturition urgency, dysuria and/or
pollakiuria. Macrohematuria is observed in 7.7% of the cases, and
although it is more frequent between 6 months and 5 years after
treatment3-5, this interval can be expanded from 6 weeks to 14 years2.
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609
vagina is to be covered, in order to avoid abrasion secondary to
instillation fluid losses. Formalinization should start at low
concentrations (1-2%), with increments if needed. The duration of
instillation in turn should not exceed 15 min., with an intravesical pressure of less than 15 cmH2O.
Intravesical treatments
Because of the potential complications of the technique, it should only
be used when other more conservative options have failed.
1. Hyaluronic acid
Intravesical hyaluronic acid temporarily restores the deteriorated
glycosaminoglycan layer of the luminal surface of the bladder wall,
Systemic treatments
stimulating connective tissue replacement and subsequently facilitating
epithelial cell nesting and recomposition.
Its use is widely accepted in interstitial cystitis5,6 and has been proposed
4. Conjugated estrogens
as preventive cotreatment in recurrent urinary infections and in
The mechanism of action whereby conjugated estrogens act in
After bladder voiding, 40 mg of product are instilled in 50 ml of
hemorrhagic cystitis has not been fully established. Such treatment is
physiological saline solution – the patient being required to retain it for
accepted to modulate cellular immune responses and cytokines, and to
at least 30 minutes. The instillations are repeated once a week for the
stimulate endothelial cell activity14. The use of conjugated estrogens in
first month and then once monthly until symptoms control is achieved.
hemorrhagic cystitis has been reported to be both effective15,16 and
ineffective17. The relatively low cost of the treatment, its few side effects,
ease of administration, and the fact that it does not condition ulterior
2. Irrigation with aluminum salts
treatment modalities, make it necessary to consider conjugated estrogens
The administration of estrogens has been associated with
Aluminum (as aluminum ammonium sulfate, aluminum hydroxide or as
hypercoagulability18 and liver toxicity; as a result, liver enzyme and
aluminum potassium sulfate) exerts a protein precipitate astringent effect
serum bilirubin determinations are required before starting treatment.
on the cell surface and in the interstitial spaces8. Such irrigation results
The administration protocol described by Ordemann et al.19 consists of
in diminished capillary permeability, contraction of the intercellular
starting treatment with 6 mg/day fractionated into three doses, followed
space, vasoconstriction, hardening of the capillary endothelium and a
by gradual increments up to 12 mg/day and/or hematuria control. The
reduction of the edema, inflammation and exudate9.
resolution of hematuria has been reported to occur from as little as 8
After extracting the possible bladder clots, irrigation is started with 5
hours post-administration to as long as after 7 days. The treatment is
liters of distilled water in which 50 g of aluminum are dissolved (1%), at
prolonged for 5-16 weeks, with descending conjugated estrogen doses.
This technique is safe, effective and generally well tolerated10. Side
effects have been reported such as suprapubic pain and spasms during the instillations9, as well as complications derived from the toxicity of
5. Pentosan polysulfate sodium
aluminum, and allergic reactions to its salts. Aluminum toxicity may be
seen in patients with renal failure and/or extensive damaged bladder
Up to 5% of the pentosan polysulfate sodium administered via the oral
surfaces that act as absorbing areas. The appearance of lethargy,
route is excreted in urine20. Although the precise mechanism of action is
confusion, metabolic acidosis or plasma aluminum elevations requires
not known, this drug repairs the urothelial glycosaminoglycan layer and
exerts an antiinflammatory effect21. Few studies have been published on
the use of pentosan polysulfate sodium, and the patient series have been
limited in size, though with long term follow-up that advocates the
3. Formalinization
efficacy of this treatment22,23. The few side effects, the absence of interactions with other treatments, and the relatively rapid results (1-8
weeks)24 make it necessary to consider this treatment as a first-line
Intravesical formalinization or formalin instillation was described by
Brown12 in 1969 as a method for controlling hematuria secondary to
advanced bladder carcinoma. Despite reported success rates of over
80%, the potential side effects and complications of this procedure have limited its use.
6. Aminocaproic acid
The toxicity of formalinization is directly dependent upon the
concentration of the formalin employed, and to a lesser extent on the
The use of epsilon aminocaproic acid for the management of hematuria
duration of exposure13. The data reported in this sense in the literature
of bladder origin has been described by a number of authors, with
different success rates. Its oral administration at a dose of 150
Toxicity is both local and systemic, secondary to absorption and
mg/kg/day during 21 days was described by Stefani et al.25 as an
metabolization to formic acid and formate. The effects include
effective way of treating hematuria in 9 patients, with hardly any side
effects. Its intravesical application was advocated by Singh et al.26 as a
obstruction, ureteral strictures, acute tubular necrosis, vesicoileal and
safe and effective option in 37 patients.
vesicovaginal fistulas, bladder disruption and toxic myocardiopathy,
It is necessary to discard possible blood dyscrasias before
administering the drug, regardless of the route employed. The short
After discarding the presence of vesicoureteral reflux with filling
series published to date and the lack of continuity in its use make it
cystography (or using Fogarty catheters to avoid reflux) and emptying
necessary to view this treatment option with caution.
the bladder of clots, the following recommendations can apply35: with
the patient under general or epidural anesthesia, the genital area (skin
and mucosal membranes) must be protected with vaseline, and/or the
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609
7. Recombinant factor VIIa
arteries, and finally small vessels that perfuse specific regions (i.e.,
supraselective embolization38). Such supraselective embolization has
Recombinant coagulation factor VIIa favors fibrin clot formation at the
made it possible to reduce the complications of the technique.
site of vascular damage, forming a complex with the exposed tissue
The most frequent problem is gluteal pain (gluteal claudication),
factor and acting upon the activated platelets27. Its use has been
resulting from embolization of the internal iliac artery and accidentally
authorized in refractory bleeding in patients with inhibitors targeted to
of the superior gluteal artery. Lower extremity necrosis has also been
factors VIII and IX, in factor VII deficiency, and in Glanzmann
described, secondary to migration of the occluding material, as well as
thrombasthenia. This treatment has been reported to be effective in
bladder wall necrosis, and rarely lower limb paraplegia due to
patients with thrombocytopenia and platelet disorders, bleeding
embolization of spinal arteries – with the consequent spinal cord
associated with oral anticoagulation, severe traumatisms and liver
diseases28, as well as in cases of severe bleeding in adult patients without
The advantages of the technique are that it can be carried out under
congenital coagulopathy or inhibitor development29.
local anesthesia, and posterior treatment modalities are not conditioned
Few randomized clinical trials have been published on the variety of
uses of such therapy, and most publications correspond to clinical notes
with small sample sizes. Scarpelini and Rizoli published a review on the
use of recombinant factor VIIa (rFVIIa) in the different surgical areas –
10. Helmstein balloon distension
reporting a decrease in preoperative bleeding in the context of retropubic
radical prostatectomy, after administering 20–40µg/kg of recombinant
In 1966, Helmstein successfully used hydrostatic pressure therapy in
factor VIIa30. However, in the mentioned study, the blood losses in the
bladder tumor treatment, inducing tissue necrosis through compression
control group were considerably higher than those considered acceptable
in 27 of the 35 patients described40. He later proposed the same method
The successful use of this treatment after radiotherapy has been
Most of the series published in relation to this technique date back to
reported in the gynecological setting31, when all other measures had
before 1980. It is globally described as useful, simple, with few side
effects, but offering only temporary action.
Candidates for treatment with rFVIIa must meet the following
The technique involves fitting a specifically designed balloon (a normal
hematological criteria32: hematocrit > 24%; fibrinogen 50–100 mg/dl;
balloon or condom can be used) to the sectioned extremity of a no. 18
platelet count > 50,000 x 109; and pH >7.2. In addition, administration
Foley catheter. Under epidural anesthesia (in order to eliminate bladder
must adhere to a series of clinical intervention measures33.
The request for recombinant factor VIIa as treatment for radiation-
induced cystitis falls within the category of “compassionate drug use”. The recommended dose is 90 µg/kg, and a second dose may be administered after 20 minutes if the desired effect is not achieved. A further number of doses has not been shown to be effective.
Physical measures
8. Hyperbaric chamber
The administration of high-pressure oxygen stimulates angiogenesis in irradiation-damaged tissues34. The sessions last 90 minutes on average,
administering 100% oxygen in chambers at a pressure of 2-2.5
Figure 1 and 2. Supraselective embolization with fibrin plugs.
atmospheres35. Treatment consists of one daily session, 5 days a week.
tone), the balloon is inserted through the urethra into the bladder. The
The number of sessions varies according to the different literature
balloon is then inflated with saline to a pressure of 10-25 25 cmH2O
sources, though a minimum of 15 and a maximum of 60 are
above diastolic pressure18. This pressure must be maintained for 6 hours.
recommended before considering other treatment options30-32. The
Although in principle Helmstein recommended the posterior
patients in the reported series received an average of 30 sessions. The
administration of mannitol to deal with meatus edematization following
start of therapy in the three months following the onset of hematuria
compression, this practice has not been shown to offer advantages in
implies higher success rates, with a reduction in the number of required
other published series41. The hemostatic effect thus obtained persists for
sessions18,19. Previous endovesical treatments do not modify the success
rates of the hyperbaric chamber19. This treatment is well tolerated – the
The most frequently described complication is bladder rupture,
reported complications being auditory and visual barotraumas in isolated
detectable by a sudden intravesical pressure change during the
procedure. In practically all such situations conservative management is
carried out with urethral catheterization.
9. Arterial embolization
11. Cystectomy
Therapeutic embolization for the control of hematuria of bladder origin
was described as far back as 1974 by Hald et al., who occluded the
Surgery is to be considered only when the above described options have
Interruption of the blood supply yields success rates of about 90%
Anatomical dissection may be complicated according to the radiation
according to the literature37. The level of occlusion has been improved
received and the time elapsed. The type of urinary derivation must be
from initial embolization of the internal iliac artery to the anterior
adapted to the individual patient characteristics, the degree of patient
branch of the internal iliac artery, the superior and inferior vesical
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609
autonomy, the background disease, and the disease prognosis.
4. Denton AS, Clarke NW, Maher EJ. Intervenciones no quirúrgicas
Historically, hypogastric artery ligation has been an option when
para la cistitis tardía por radiación en pacientes que han recibido
radioterapia radical de pelvis (Revision Cochrane traducida). En:
La Biblioteca Cochrane Plus, 2008 Number 2. Oxford: Update Software Ltd. Available in: http://www. update-software.com.
Proposed algorithm
(Translated from The Cochrane Library, 2008 Issue 2.
Chichester,UK: John Wiley & Sons, Ltd.).
In the event of hematuria in a patient subjected to pelvic radiotherapy,
5. Kallestrup EB, et al. Treatment of intersticial cistitis with Cystistat:
the presence of bladder neoformations must be discarded, along with
a hialuronic acid product. Scan Journal of Urology. 2005;39:143–7.
hematuria of upper urinary tract origin.
6. Nordling J, Jorgensen S, Kallestrup E. Cystistat for the treatment of
When hematuria is attributed to radiation-induced cystitis, progressive
intersticial cistitis:a 3-year follow-up study. Urology. 2001;57(6
treatment should be provided after hemodynamic stabilization of the
7. Preventing radiation induced cistitis with hyaluronic acid. J Support
Formalinization should be considered only in life-threatening situations
where surgery is contraindicated. The following management algorithm
8. Ostroff EB, Chenault Jr OW. Alum irrigation for the control of
massive bladder hemorrhage. J Urol. 1982;128:929–30.
9. Arrizabalaga M, Extramiana J, Parra JL, et al. Treatment of
massive haematuria with aluminous salts. Br J Urol. 1987;60: 223–
10. Goswami AK, Mahajan RK, Nath R, et al. How safe is 1% alum
irrigation in controlling intractable vesical hemorrhage? J Urol
11. Choong M, Walkden R, Kirby. The management of intractable
Start outpatient hyaluronic instillations
12. Brown RB. A method of management of inoperable carcinoma of
13. Godec CJ, Gleich P. Intractable hematuria and formalin. J Urol.
Urethrocystoscopy in operating room: clot extraction and
14. Deshpande R, Khalili H, Pergolizzi RG, et al. Estradiol
electrocautery of suspect areas, with biopsy
downregulates LPS-induced cytokine production and NFkB
activation in murine macrophages. Am J Reprod Immunol.
15. Miller J, Burfield GD, Moretti KL. Oral conjugated estrogen
therapy for treatment of hemorrhagic cystitis. J Urol. 1994;151:
16. Rodriguez Luna JM, Teruel JL, Vallejo J, et al. Control of massive
hematuria in idiopathic hemorrhagic cystitis after administration of
conjugated estrogen. J Urol. 1992;148: 1524–5.
17. Vance BJ. Hemorrhagic cystitis: failure of estrogen treatment.
18. Daly E, Vessey MP, Hawkins MM, et al. Risk of venous
thromboembolism in users of hormone replacement therapy.
19. Ordemann R, Naumann R, Geissler G, et al. Encouraging results in
the treatment of haemorrhagic cystitis with estrogen-report of 10
Conclusions
casers and review of the literature. Bone Marrow Transplantation. 2000;25:981–5.
20. Parsons CL, Mulholland SG, Anwar H. Antibacterial activity
A brief account has been provided of the majority of available
therapeutic options. There is no single or ideal treatment. Knowing the
glycosaminoglycans. Infect Immun. 1979;24:552–7.
different options and their administration protocols will allow the
21. Chiang G, PATRA P, Letorneau R, et al. Pentosan polysulfate
urologist to secure a higher success rate in the difficult management of
inhibts mast cell histamine secretion and intracellular calcium ion
levels: an alternative explanation of its beneficial effect in
intersticial cystitis. J Urol. 2000;164:2119–25.
Conflicts of interest
22. Hampson SJ, Woodhouse CR. Sodium pentosan polysulphate in the
Management of haemorrhagic cistitis:Experience with 14 patients.
The authors declare no conflicts of interest.
23. Parson CL. Successful Management of radiation cistitis with
sodium pentosan polysulfate. J Urol. 1986;136:813–4.
24. Sandhu S, Goldstraw M, Woodhouse C. The management of
1. Pavlidakey P, MacLennan G. Radiation Cystitis. Journal of
haemorrhagic cystitis with sodium pentosan polysulphate. BJU.
2. Crew JP, Jephcott CR, Reynard JM. Radiation induced
25. Stefani M, English HA, Taylor AE. Safe and effective, prolonged
haemorrhagic cystitis. Eur Urol. 2001;40:111.
administration of epsilon aminocaproic acid in bleeding from the
3. Chan TY, Epstein JI. Radiation or chemotherapy cystitis with
urinary tract. J Urol. 1990;143:559–61.
„„pseudocarcinomatous‟‟ features. Am J Surg Pathol. 2004;28: 909.
26. Singh I, Laungani GB. Intravesical epsilon aminocaproic acid in
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609
management of intractable bladder hemorrhage. Urology. 1992;40:227–9.
27. Hedner U. Novoseven as a universal haemostatic agent. Blood
Coagul Fibrinolysis. 2000;11(Suppl 1):107–11.
28. Goodnough LT. Utilization of recombinant factor VIIa(rFVIIa) in
no-approved settings. Haematology (ASH Education program Book). 2004;1:466–70.
29. Lecumberri R, Paramo J, Hidalgo F, et al. Reducción de las
necesidades transfusionales en hemorragias adquiridas graves mediante factor VII activo recombinante. Med Clin. 2005;125:252–3.
30. Scarpelini S, Rizoli S. ecombinant factor VIIa and the surgical
patient. Current Opinion in Critical Care. 2006;12: 351–6.
31. Geisler JP, Linnemeier GC, Manahan KJ. Recombinant factor VIIa
to treta late radiation-induced hemorrhagic cistitis: a case report. J Reprod Med. 2008;53:360–2.
32. Vicent JL, Rossaint R, Riou B. Recommendations on the use of
recombinant activated factor VII as an adjunctive treatment for massive bleeding-a European perspectiva. Critical Care. 2006;10:R 120, doi:, doi:10.1186/cc5026.
33. Martinowitz U. Guidelines for the use of recombinant activated
factor VII(frFVIIa) in controlled bleeding: a report by the Israelı´ Multidisciplinary rFVIIa Task Force. Journal of Thrombosis and Haemostasis. 2005;3:640–8.
34. Mathews R, Rajan N, Josefson L, et al. Hiperbaric Oxygen Therapy
for irradiation induced hemorrhagic cystitis. Journal of Urology. 1999;161:435–7.
35. Chong KT, Kampson NB, Corman JM. Early hyperbaric oxygen
therapy improves outcome for radiation-induced hemorrhagic cystitis. Urology. 2005;65:649–53.
36. Hald T, Mygind T. Control of life-threating vesical hemorrhage by
unilateral hypogastric artery muscle embolization. J Urol. 1974;112:60–3.
37. McIvor J, Williams G, Southcott RD. Control of severe vesical
haemorrhage by therapeutic embolisation. Clin Radiol. 1982; 33:561–7.
38. De Bernardinis E, Vicini P, Salvatori F, et al. Superselective
embolization of bladder arteries in the treatment of intractable bladder haemorrhage. Int J Urol. 2005;12:503–5.
39. Palma Ceppi C, Reyes Osorio D, Palma Ceppi R, et al. Experience
in superselective embolization of bladder arteries in the treatment of intractable haematuria. Actas Urol Esp. 2008;32:542–5.
40. Helmstein K. Treatment of bladder carcinoma by a hydrostatic
pressure technique. Br J Urol. 1972;44:434–50.
41. Iveresen Hansen, Djurhuus J, Nestrom B. Hydrostatic pressure
treatment for carcinoma of the bladder. Scand J Urol Nephrol. 1976;10:209–13.
42. England HR, Rigby C, Shepheard BGF. Evaluation of Helmstein‟s
distension method for carcinoma of the bladder. Br J Urol. 1973;45:593–9.
(A) Biological Science (BS) 1. Dhaka University and Food Science composition databank on multi-(INFS), University ingradient cook foods and a Psychology, Dhaka Scales of infant Development Monopterus Cuchia, a non-Traditional Export Commodity of Bangladesh University, Probiotic Bacteria in Shrimp of Zoology, Dhaka diagnosis, treatment, prevention University, Dhaka- and control of ve
animal studies should be acknowledged, since some PBM has received payment for lectures or advisory board membership from reports11 have suggested that rimonabant might have AstraZeneca, Eli Lilly, GlaxoSmithKline, Janssen-Cilag, and Lundbeck in the past 3 years. MJM declares that she has no confl ict of interest. antidepressant or anxiolytic actions. Another obser-Di Marzo V, Matias I. Endo

 Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609 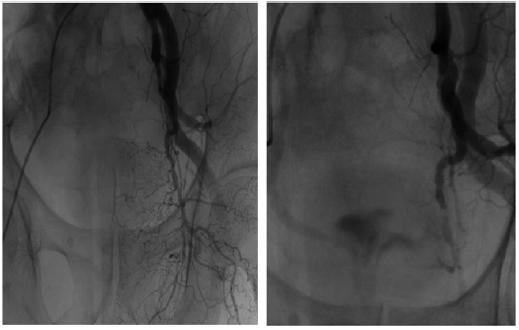 Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609
Document downloaded from http://www.elsevier.es on 18/06/2010. Copy for personal use. Transmission of this document by any means or in any format is forbidden.
ACTAS UROL ESP. 2010;34(7):603–609