La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Adjuvant doxorubicin and cyclophosphamide versus cyclophosphamide, methotrexate, and 5-fluorouracil chemotherapy in premenopausal women with axillary lymph node positive breast carcinoma
Adjuvant Doxorubicin and Cyclophosphamide versus Cyclophosphamide, Methotrexate, and 5-Fluorouracil Chemotherapy in Premenopausal Women with Axillary Lymph Node Positive Breast Carcinoma Results of a Randomized Controlled Trial Soo-Mee Bang, BACKGROUND. This randomized controlled trial was to determine whether a com- Dae Seog Heo,
bination chemotherapy regimen that contains anthracycline (doxorubicin and
Ki Hyeong Lee,
cyclophosphamide [AC]) is superior to the conventional cyclophosphamide, meth-
Jae Ho Byun,
otrexate, and 5-fluorouracil [CMF] combination in premenopausal women with
Heung Moon Chang,
axillary lymph node positive Stage II breast carcinoma. Dong-Yong Noh, METHODS. Premenopausal women with lymph node positive breast carcinoma Kuk Jin Choe,
were stratified according to age (younger than 35 or 35 years or older) and the
Yung-Jue Bang,
number of positive axillary lymph nodes (1–3, 4 –9, or Ն 10) and then randomly
Sung Rok Kim,
assigned to receive either doxorubicin 40 mg/m2 and cyclophosphamide 600
Noe Kyeong Kim,
mg/m2 intravenously (i.v.) every 3 weeks or cyclophosphamide 100 mg/m2 orally
on Days 1 through 14, methotrexate 40 mg/m2 and 5-fluorouracil 500 mg/m2 i.v. on
1 Department of Internal Medicine and Surgery,
Days 1 and 8 every 4 weeks. Both arms were scheduled for six cycles.
Clinical Research Institute, Seoul National Univer-
RESULTS. The median follow-up was 57 months. Eighteen of the 55 AC patients
sity College of Medicine, Seoul, Korea.
developed recurrence compared with 16 of the 69 CMF patients. The correspond-
2 Department of Internal Medicine, College of Med-
ing 5-year recurrence free survival rates were 64% and 78%, respectively (P ϭ 0.12).
icine, Chung-Buk University, Cheongjue, Korea.
The site of the first recurrence for AC patients was locoregional in 7%, distant in
3 Department of Internal Medicine, College of Med-
22%, and combined in 4%. The corresponding data for the CMF arm were 4%, 16%,
icine, In-Jae University, Seoul, Korea.
and 3%, respectively. Six AC patients died compared with 9 CMF patients. The
corresponding 5-year survival rates were 90% and 86%, respectively (P ϭ 0.96). More leukopenia (52%, mostly Grade 1–2) occurred in the CMF arm than in the AC
arm (33%, P ϭ 0.001), but no febrile episode was accompanied with leukopenia. CONCLUSIONS. This study showed no difference between AC and CMF with respect to both disease free and overall survival rates in premenopausal women with
axillary lymph node positive breast carcinoma. Cancer 2000;89:2521– 6. KEYWORDS: breast neoplasm, adjuvant chemotherapy, doxorubicin and cyclophos-
Supported in part by 1999-BK21 project for Med-
phamide (AC), cyclophosphamide, methotrexate, and 5-fluorouracil (CMF).
Address for reprints: Noe Kyeong Kim, M.D., De-
Adjuvant chemotherapy is known to decrease the recurrence and
partment of Internal Medicine, Seoul National Uni-
improve the survival rate of women with axillary lymph node
versity, Hospital, 28 Yongon-dong, Chongno-gu,
positive breast carcinoma.1 The combination chemotherapy regimen
Seoul, 110-744 Korea; fax: 82-2-742-6689;
of cyclophosphamide, methotrexate, and 5-fluorouracil (CMF), first
reported to be effective in lymph node positive breast carcinoma in1976, is still a commonly used adjuvant chemotherapy regimen.2
Received March 20, 2000; revisions received June28, 2000 and August 15, 2000; accepted August
However, the results of several clinical trials have failed to show the
role of anthracycline in the adjuvant setting in patients with axillary
CANCER December 15, 2000 / Volume 89 / Number 12
lymph node positive breast carcinoma. In the National
35 or 35 years or older) and number of positive axillary
Surgical Adjuvant Breast and Bowel Project (NSABP-
lymph nodes (1–3, 4 –9, or Ն 10). Sequential cards
B15) trial, women with axillary lymph node positive
were used for the randomization procedure.
breast carcinoma were randomized to receive either
Patients in the AC group received doxorubicin 40
CMF or doxorubicin and cyclophosphamide (AC); no
mg/m2 and cyclophosphamide 600 mg/m2 i.v., every 3
difference was detected in disease free or overall sur-
weeks for 6 cycles. Patients in the CMF group received
vival.3 Other trials have compared CMF with CMF
cyclophophamide 100 mg/m2 p.o. on Days 1 through
followed by doxorubicin,4 CMF with 5-fluorouracil,
14, methotrexate 40 mg/m2 and 5-fluorouracil 500
epirubicin, and cyclophophamide (FEC),5 and CMF
mg/m2 i.v. on Days 1 and 8 every 4 weeks for 6 cycles.
with cyclophosphamide, doxorubicin, and 5-fluorou-
If on the day of the therapy the leukocyte count was
racil (CAF).6 No differences were detected during
less than 3.0 ϫ 109/L or the platelet count was less
these trials between regimens in disease free and over-
than 75 ϫ 109/L, it was recommended that treatment
all survival.4–6 However, a French trial showed long
be delayed for a maximum of 2 weeks and weekly
term survival benefits of anthracycline-based chemo-
blood counts were performed. Dose reduction by 25%
therapy. In this study, patients were randomized to
was recommended for a leukocyte count of 3.0 –3.9
receive 12 cycles of CMF or doxorubicin, vincristine,
ϫ 109/L or a platelet count of 75–100 ϫ 109/L.
cyclophosphamide, and 5-fluorouracil (AVCF).7 An-
After completion of chemotherapy, patients were
other trial that compared FEC with a CMF regimen
examined every 3 months until the end of the second
showed that patients on the FEC regimen had superior
year, then every 6 months for 5 years, and yearly
recurrence free and overall survival rates at 5 years.8
thereafter. At each follow-up visit, patients underwent
We therefore conducted a trial to investigate
a physical examination, and a history was taken, and a
whether the AC regimen is superior to the conven-
complete blood count, platelet count, and liver func-
tional CMF combination in premenopausal women
tion test were performed. Chest X-ray, abdominal ul-
with lymph node positive operable breast carcinoma.
trasonography, and bone scan were checked everyother visit. PATIENTS AND METHODS
The major outcome measures for the study were
Premenopausal women with histologically confirmed
recurrence free survival, overall survival, and toxicity.
axillary lymph node positive breast carcinoma who
Recurrence free survival, the primary protocol-defined
had undergone modified radical mastectomy or
outcome measure of the study, was timed from ran-
quadrantectomy plus axillary dissection were enrolled
domization until recurrence. Locoregional recurrence
in this study (T1 or T2N1M0 according to American
included recurrences in the breast, local chest wall,
Joint Committee on Cancer TNM classification). Post-
and regional recurrence. Regional recurrence was de-
operative radiotherapy was mandatory after the
fined as a recurrent tumor in the lymph nodes of
breast-conserving surgery. Elective radiotherapy after
ipsilateral axillary, supraclavicular, or internal mam-
mastectomy was adopted at the direction of the par-
mary chain. Distant recurrence was defined as a
ticipating physicians. Radiotherapy was performed af-
spread of the disease systemically beyond the limits
ter the completion of chemotherapy. Hormone recep-
previously described. A carcinoma that developed in
tor assays were not available for all patients.
the opposite breast without any evidence of systemic
Patients were excluded from the study if they had
metastasis was considered as a new primary malig-
any evidence of metastasis, a documented history of
cardiac disease or previous cancer, inadequate renalfunction (as indicated by a serum creatinine levelϾ 1.5 times the normal upper limit), or elevated levels
Statistical Considerations
of liver enzymes (bilirubin Ͼ 3 mg/L, alkaline phos-
Survival time and time to recurrence were calculated
phatase Ͼ 1.5 times the normal upper limit, or aspar-
using the Kaplan–Meier method, and the log rank test
tate amintotransferase Ͼ 1.5 times the normal upper
was used to compare the curves of the survival times
limit), a serious underlying medical illness or locally
and the times to progression. The Cox proportional
advanced breast carcinoma before surgery, micro-
hazards model was used to adjust the observed treat-
scopic or macroscopic evidence of residual tumor, or
ment effect for the influence of various prognostic
if more than 7 weeks has elapsed from the initial
factors at study entry, and to detect the effect of un-
derlying prognostic factors on outcome. Other char-
Patient accrual began on October 1989 and was
acteristics of the two treatment arms were compared
completed on July 1996. After assignment to the study,
using the chi-square test. All calculations were per-
patients were stratified according to age (younger than
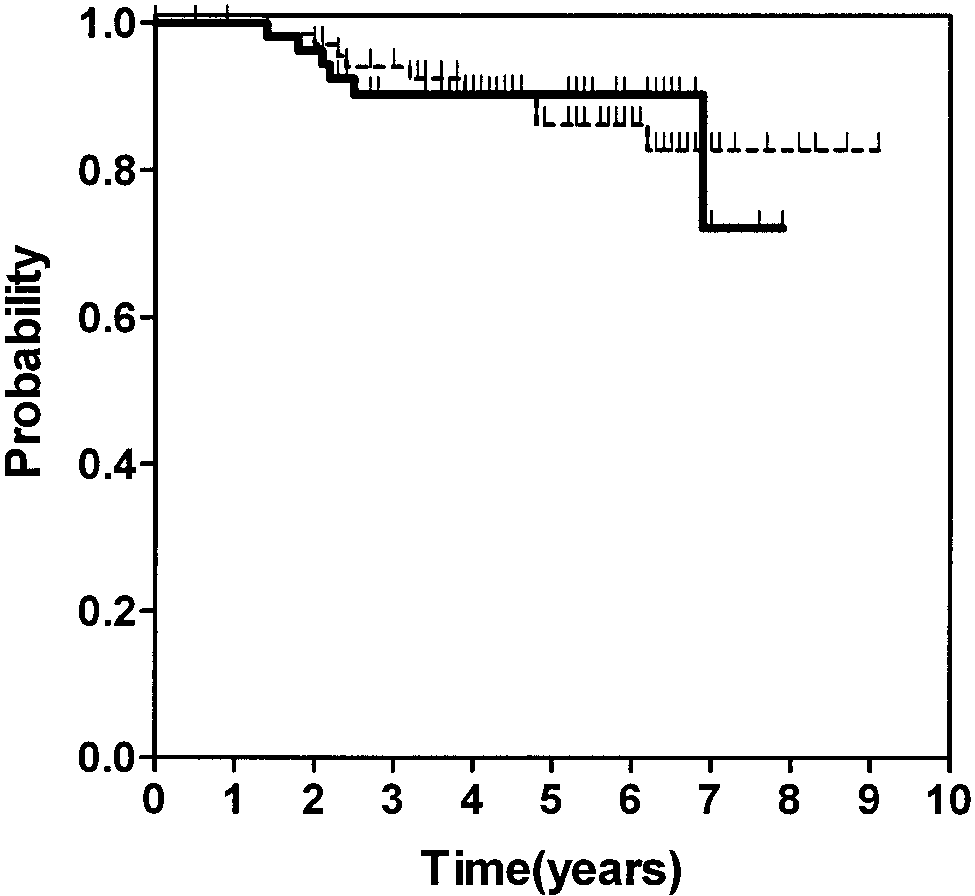
AC vs. CMF in Breast Carcinoma/Bang et al. TABLE 1 Baseline Characteristics of Study Patients FIGURE 1. Recurrence free survival of AC versus CMF (P ϭ 0.12). Solid black line, AC; dashed line, CMF.
MRM, modified radical mastectomy; Quad ϩ AND, quadrantectomy with dissection of axillary lymphnode; RT, radiation therapy; ER, estrogen receptor. a One patient who underwent Quad ϩ AND received radiotherapy after completion of chemotherapy. Recurrence Free Survival Eighteen AC patients developed recurrence of their breast carcinomas compared with 16 CMF patients.
The 5-year recurrence free survival rate of the AC
Patient Population
patients was 64% (95% confidence interval, 57–71%)
The trial was started in 1989 and was closed in 1996.
The median follow-up was 57 months. Fifty-eight
72– 84%) for the CMF patients (P ϭ 0.12; Fig. 1). The
women were allocated to AC therapy and 70 to CMF
site of the first recurrence for AC patients was locore-
therapy. This discrepancy in the number of patients
gional in 4 (7%) patients, distant in 12 (22%) patients,
was due to randomization procedure without bloc.
and combined in 2 (4%) patients. The corresponding
Three patients in the AC arm and one patient in the
data for the CMF arm were 3 (4%), 11 (16%), and 2
CMF arm were lost in follow-up after one to three
(3%) patients, respectively. There were three cases of
cycles of chemotherapy and were not included for the
contralateral breast carcinoma in the AC group com-
evaluation of recurrence, survival and toxicity. The
pared with two cases in the CMF group.
treatment groups were reasonably similar with respect
The 5-year recurrence free survival rates for sub-
to baseline characteristics, such as age, type of sur-
groups such as age (younger than 35 or 35 years or
gery, additional radiotherapy, tumor stage, number of
older), tumor stage (T1 or T2), number of the positive
positive axillary lymph nodes, and status of estrogen
axillary lymph nodes (1–3, 4 –9, or Ն 10), average rel-
ative dose intensity (Ͻ 0.8 or Ն 0.8) and average rel-ative dose intensity of doxorubicin (Ͻ 0.8 or Ն 0.8) arelisted in Table 2. In univariate and multivariate anal-
Drug Dosages
ysis, both tumor stage and the number of positive
Fifty-five patients treated with AC and 69 patients
lymph nodes were significant prognostic factors.
treated with CMF completed 6 cycles of chemother-apy. The average relative dose intensity for the drugs
Survival
in AC was 0.81 Ϯ 0.08, and the average relative dose
Six patients on the AC arm died compared with nine
intensity of doxorubicin was 0.83 Ϯ 0.08. The average
patients on the CMF arm. All these patients died of
relative dose intensity for the drugs in CMF was 0.86
disease progression. The 5-year survival rates were
Ϯ 0.10. The average relative dose intensity for the
90% (95% confidence interval, 86 –94%) and 86% (95%
drugs in AC was significantly lower than that of CMF
confidence interval, 82–90%), respectively (P ϭ 0.96;
Fig. 2). The 5-year survival rates for the subgroups are
CANCER December 15, 2000 / Volume 89 / Number 12 TABLE 2 Recurrence Free Survival and Overall Survival Subgroups P valuea P valueb P valuea P valueb
RFS: recurrence free survival; OS: overall survival; RDI: relative dose intensity. a Univariate analysis. b Multivariate analysis. c Of all drugs. d Of doxorubicin in the doxorubicin and cyclophosphamide arm. TABLE 3 Incidence of Hematologic Toxicity Significancea (P value)
AC: doxorubicin and cyclophosphamide; CMF: cyclophosphamide, methotrexate, and 5-fluorouracil. a Chi-square test.
episode of Grade 1 anemia and 5 episodes of Grade 2anemia in the CMF arm. FIGURE 2. Overall survival of AC versus CMF (P ϭ 0.96). Solid black line, AC; DISCUSSION
This report indicates that the recurrence free survival,overall survival, and patterns of treatment failure ofpatients treated with AC are nearly identical to those
listed in Table 2. Age and the number of positive
obtained after the administration of conventional
lymph nodes were significant predictors of survival by
CMF. Our results are similar to those of the NSABP-15
univariate and multivariate analysis.
trial. However, the schedule of chemotherapy and thedose intensity of doxorubicin were different. Planned
Toxicity
dose intensity of doxorubicin was 13.3 mg/m2/week
More leukopenia occurred in the CMF arm and no
for 18 weeks in our trial; compared with 20 mg/m2/
patients suffered from febrile leukopenia in either
week for 12 weeks in NSABP-15.3 The recommenda-
arm. No difference was found in the incidence of
tion of AC in an adjuvant setting by NSABP-15 was
anemia. Two patients who had had iron deficiency
made because the toxicity resulting from 12 weeks of
anemia before adjuvant chemotherapy developed 1
AC therapy compared favorably with side effects as-
AC vs. CMF in Breast Carcinoma/Bang et al.
sociated with 24 weeks of conventional CMF. Doxoru-
prospective randomized trial, Peters et al.11 random-
bicin and cyclophosphamidechemotherapy was ex-
ized 783 patients with Stage II or IIIA breast carcinoma
amined for a longer period in our study and this
involving 10 or more axillary lymph nodes to receive
benefit with respect to duration and toxicity was
either high dose CPB (cyclophosphamide, cisplatin,
found to be reduced compared with the NSABP-15
and BCNU) with stem cell support or intermediate-
trial. In the French trial, the duration of adjuvant
dose CPB with granulocyte-colony stimulating factor
chemotherapy was 48 weeks, and the dose intensity of
support after 4 cycles of CAF. The intent-to-treat event
doxorubicin was 7.5 mg/m2/week. Although the dose
free survival and overall survival comparisons were
intensity of doxorubicin was lower than that of other
inconclusive after a median follow-up of 37 months.
trial, the total dose of doxorubicin was 2.5 times larger
Therapy-related deaths (7%) occurred only in the high
than that of NSABP-15 and our trials. In addition, the
dose CPB arm. This result needs cautious application
dose intensity of cyclophosphamide was also 1.5 times
of high dose chemotherapy. Another approach to im-
and vincristine was added. During the median follow-
prove the outcome of high risk group is adding tax-
up of 13 years, benefits of recurrence free and overall
anes to adjuvant doxorubicin-based chemotherapy.
survival increased evidently in the AVCF arm.7 In a
Henderson et al.12 reported that the addition of pac-
Canadian trial, epirubicin was substituted for doxoru-
litaxel reduced the recurrence rate by 22% and the
bicin, and the dose intensity of epirubicin was 30
death rate by 26% by multivariate analysis. This in-
mg/m2/week for 24 weeks. Patients with ECF chemo-
terim analysis will be reevaluated after longer follow-up.
therapy had better survival.8 The Cancer and Leuke-mia Group B have indicated that the total dose re-mains a critical determinant of outcome and dose
REFERENCES 1.
Early Breast Cancer Trialists Collaborative Group. Systemic
reduction, perhaps less than a threshold, leads to a
treatment of early breast cancer by hormonal, cytotoxic or
relatively worse outcome of the CAF regimen.9 These
immune therapy: 133 randomized trials involving 31,000
results suggest that anthracycline itself is not a prog-
recurrences and 24,000 deaths among 75,000 women. Lan-
nostic indicator, but that both the drug dose of an-
thracycline and other combined drugs may be the
Bonadonna G, Brusamolino E, Valagussa P, Rossi A, Brug-natelli L, Brambilla C, et al. Combination chemotherapy as
major prognostic factor. Our study was designed with
an adjuvant treatment in operable breast cancer. N Engl
lower dose of doxorubicin and the actual relative dose
intensity of AC arm was lower than that of the CMF
Fisher B, Brown AM, Dimitrov NV, Poisson R, Redmond C,
arm (P ϭ 0.006). The second factor is that a longer
Margolese RG, et al. Two months of doxorubicin-cyclo-
follow-up period is needed to ascertain the role of
phophamide with and without interval reinduction therapycompared with six months of cyclophophamide, methotrex-
anthracycline in adjuvant chemotherapy in lymph
ate and 5-fluorouracil in positive-node breast cancer pa-
node positive breast carcinoma. These factors may
tients with tamoxifen-nonresponsive tumors: results from
have contributed to our negative result.
the National Surgical Adjuvant Breast and Bowel Project
In subgroup analysis, the number of positive
B-15. J Clin Oncol 1990;8:1483–96.
lymph nodes was significant prognostic factor of re-
Moliterni A, Bonadonna G, Valagussa P, Ferrari L, ZambettiM. Cyclophophamide, methotrexate and 5-fluorouracil with
currence and survival. But recurrence of patients who
and without doxorubicin in the adjuvant treatment of re-
had 10 or more positive lymph nodes was paradoxi-
sectable breast cancer with one to three positive axillary
cally lower than that of those with 4 –9 positive lymph
nodes. J Clin Oncol 1991;9:1124 –30.
nodes. The number of patients with 10 or more posi-
Coombes RC, Bliss JM, Wils J, Morvan F, Espie´ M, Amadori
tive lymph nodes was only 14 in this trial. Thus, our
P, et al. Adjuvant cyclophophamide, methotrexate and 5-flu-orouracil versus 5-fluorouracil, epirubicin, and cyclo-
confounding result may be due to the small size of this
phophamide chemotherapy in premenopausal women with
subgroup. The 5-year recurrence free and overall sur-
axillary node-positive operable breast cancer: results of a
vival of this lymph node group was 69% and 76%,
randomized trial. J Clin Oncol 1996;14:35– 45.
respectively, in our data. Even in the best published
Carpenter JT, Velez-Garcia E, Aron BS, Salter M, Stahl DL,
results of standard adjuvant chemotherapy in this
Estes N, et al. Five-year results of a randomized comparisonof cyclophophamide, doxorubicin, and 5-fluorouracil versus
group, 50% of patients experience a recurrence and
cyclophophamide, methotrexate and 5-fluorouracil for
30% die within 5 years of diagnosis.10 New approaches
node-positive breast cancer [abstract]. Proc Am Soc Clin
to the management of this high risk group are being
actively investigated. One method involves the admin-
Misset JL, di Palma M, Delgado M, Plagne R, Chollet P,
istration of higher-than-standard doses of chemother-
Fumoleau P, et al. Adjuvant treatment of node-positivebreast cancer with cyclophosphamide, doxorubicin, flu-
apy. Hematopoietic growth factors and the supporting
orouracil, and vincristine versus cyclophosphamide, meth-
of stem cells have allowed the safe administration of
otrexate, and fluorouracil: final report after a 16-year me-
much larger doses of chemotherapy. In the largest
dian follow-up duration. J Clin Oncol 1996;14:1136 – 45. CANCER December 15, 2000 / Volume 89 / Number 12
Levine MN, Bramwell VH, Prichard KI, Norris BD, Shepherd
resectable breast cancer with more than three positive axil-
LE, Abu-Zahra H, et al. Randomized trial of intensive cyclo-
lary modes. J Clin Oncol 1991;9:2134 – 40.
phophamide, epirubicin, and 5-fluorouracil chemotherapy
11. Peters W, Rosner G, Vrenenburgh J, Shpall E, Crump M,
compared with cyclophophamide, methotrexate and 5-flu-
Richardson P, et al. A prospective randomized comparison
orouracil in premenopausal women with node-positive
of two doses of combination alkylating agents as consolida-
breast cancer. J Clin Oncol 1998;16:2651– 8.
tion after CAF in high-risk primary breast cancer involvingten or more axillary lymph nodes: preliminary results of
Budman DR, Berry DA, Cirricione CT, Henderson IC, Wood
CALGB 9082/SWOG 9114/NCIC MA-13 [abstract]. Proc Am
WC, Weiss RB, et al. Dose and dose intensity as determi-
nants of outcome in the adjuvant treatment of breast can-
12. Henderson IC, Berry D, Demetri G, Cirrincione C, Goldstein L,
cer. The Cancer and Leukemia Group B. J Natl Cancer Inst
Martino S, et al. Improved disease-free (DFS) and overall sur-
vival (OS) from the addition of sequential paclitaxel(T) but not
10. Buzzoni R, Bonadonna G, Valagussa P, Zambetti M. Adju-
from the escalation of doxorubicin(A) dose level in the adju-
vant chemotherapy with doxorubicin plus cyclophospha-
vant chemotherapy of patients with node-positive primary
mide, methotrexate, and 5-fluorouracil in the treatment of
breast cancer [abstract]. Proc Am Soc Clin Oncol 1998;17:101a.
411: Verplegen van kinderen en jeugdigen Extra praktijksituaties 411 11 Sanna heeft astma Het bestuderen van deze praktijksituatie en de bijbehorende vragen en opdrachten levert een bijdrage aan het behalen van de volgende eindtermen: 411-01.1-4, 411-02.1-2, 411-03.1-2, 411-03.5, 411-04.1, 411-05 en 411-06. Het is zaterdagmiddag, het regent buiten en Sanna ligt een beetje vervee
Rapid Communication Prevalence of clopidogrel non-responders among patientswith stable angina pectoris scheduled for elective coronarystent placementIris Müller, Felicitas Besta, Christian Schulz, Steffen Massberg, Albert Schönig, Meinrad GawazDeutsches Herzzentrum und 1. Medizinische Klinik, Klinikum rechts der Isar,Technische Universität München, Munich, Germany Summary Dual antiplatel
 AC vs. CMF in Breast Carcinoma/Bang et al.
AC vs. CMF in Breast Carcinoma/Bang et al.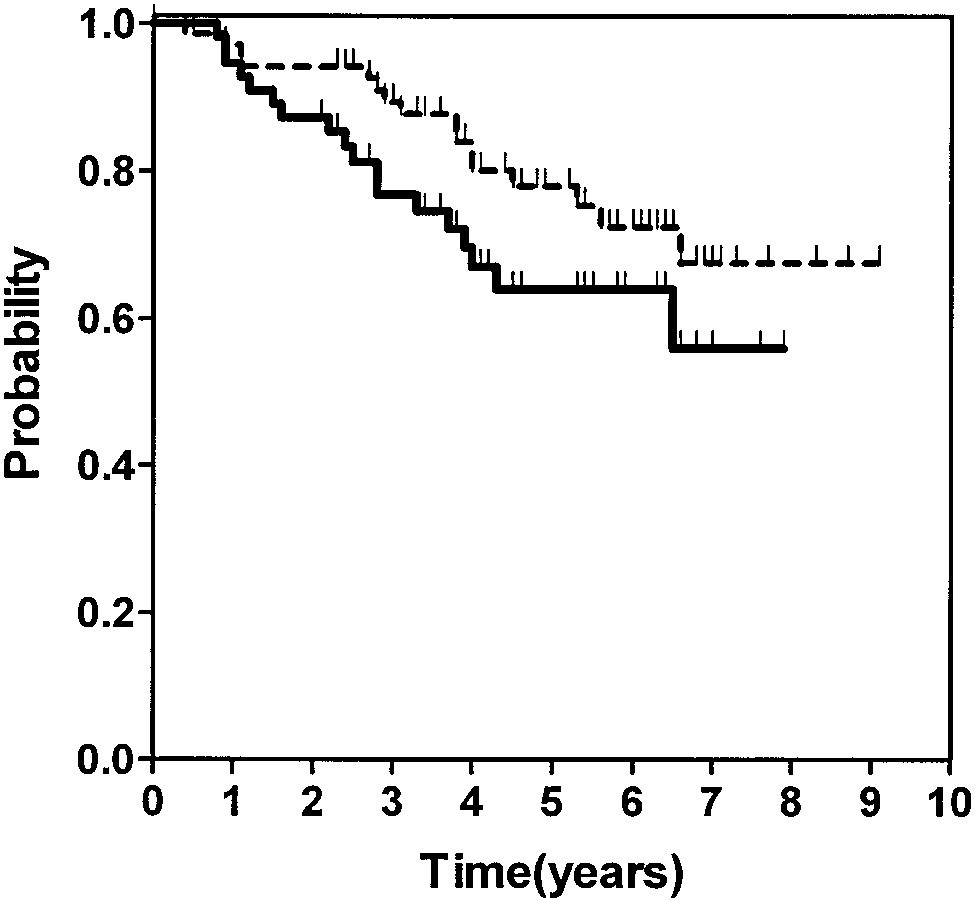 CANCER December 15, 2000 / Volume 89 / Number 12
CANCER December 15, 2000 / Volume 89 / Number 12