La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Müller: prevalence of clopidogrel non-responders among patients with stable angina pectoris …
Rapid Communication
Prevalence of clopidogrel non-responders among patientswith stable angina pectoris scheduled for elective coronarystent placement
Iris Müller, Felicitas Besta, Christian Schulz, Steffen Massberg, Albert Schönig, Meinrad GawazDeutsches Herzzentrum und 1. Medizinische Klinik, Klinikum rechts der Isar,Technische Universität München, Munich, Germany
Summary Dual antiplatelet therapy with aspirin and clopidogrel decreas-
tion that was less than 10% when compared to baseline values
es the rate of stent thrombosis in patients undergoing percu-
4 h after clopidogrel intake. Semi-responders were identified by
taneous coronary intervention (PCI). However, despite intensi-
an inhibition of 10 to 29%. Patients with an inhibition over 30%
fied antiplatelet treatment, up to 4.7% of the patients undergo-
were regarded as responders.We found that 5 (ADP 5 Mol/L)
ing coronary stenting develop thrombotic stent occlusion, sug-
to 11% (ADP 20 Mol/L) of the patients were non-responders
gesting incomplete platelet inhibition due to clopidogrel re-
and 9 to 26% were semi-responders. Among the group of non-
sistance. We evaluated the percentage of clopidogrel non-
responders there were two incidents of subacute stent throm-
responders among 105 patients with coronary artery disease
bosis after PCI. We conclude that a subgroup of patients
(CAD) undergoing elective PCI.All patients were treated regu-
undergoing PCI does not adequately respond to clopidogrel,
larly with aspirin 100 mg/d and received a loading dose of 600
which may correspond to the occurrence of thromboischemic
mg clopidogrel followed by a maintenance dose of 75 mg/d
complications. Point-of-care testing may help to identify these
before PCI. Clopidogrel non-responders were defined by an
patients who may then benefit from an alternative antiplatelet
inhibition of ADP (5 and 20 Mol/L) induced platelet aggrega-
Keywords Platelets, clopidogrel, non-responders, stenting, coronary artery disease Thromb Haemost 2003; 89: 783 –7 Introduction
Intracoronary stents are effective in the treatment of abrupt ves-
considerably lowered the rates of stent thrombosis (2-4). A
sel occlusion and improvement of suboptimal angioplasty
major clinical goal of antithrombotic therapy in patients under-
results. In contrast, subacute stent thrombosis is associated with
going coronary stent implantation is to be effective as soon as
a substantial increase in periprocedural morbidity and mortality
possible to prevent early stent thrombosis. Recently we found
(1). The introduction of dual antiplatelet therapy with a combi-
that increasing the loading dose of clopidogrel up to 600 mg
nation of aspirin and a thienopyridine (ticlopidine, clopidogrel)
results in rapid and pronounced inhibition of ADP-induced
Accepted after revision February 26, 2003
Deutsches Herzzentrum und 1. Medizinische KlinikKlinikum rechts der Isar, Technische Universität München
Financial support:This work was supported by a grant from the
Deutsche Forschungsgemeinschaft (Ga 381/4-1)
and by the Graduate Program 438 Vascular Biology in Medicine.
Tel.: +49-89-1218-4012, Fax: +49-89-1218-4003E-mail: gawaz@dhm.mhn.de
platelet aggregation with maximal inhibition four hours after
Platelet aggregation and definition of clopido-
first administration (5, 6). The purpose of the present study was
grel non-responders
to evaluate the consistency and inter-individual variability of
The effect of clopidogrel on platelet function was evaluated ex
platelet inhibition after clopidogrel administration in patients
vivo with platelet-rich plasma (PRP) by optical aggregometry as
with stable coronary artery disease scheduled for coronary
described (7). ADP (5 and 20 Mol/L) was used to induce plate-
let aggregation. Inhibition of aggregation was calculated in % asthe absolute reduction in maximum aggregation achieved by
ADP (5 and 20 Mol/L) 4 h after clopidogrel administrationcompared to baseline aggregation values before clopidogrelintake. Patients were considered responsive to clopidogrel if
Patients
inhibition of aggregation was higher than 30%. Non-responders
We studied 105 patients with stable coronary artery disease. All
were defined by a platelet inhibition of less than 10% and semi-
patients received regular aspirin therapy with a daily dose of
responders were characterized by an inhibition of platelet aggre-
100 mg. The study was performed according to the Declaration
of Helsinki and after approval by the Institutional EthicsCommittee of the Technische Universität München. All patients
Statistical analysis
were extensively informed and provided written consent before
Continuous variables are reported as mean ± standard deviation
the following treatment. Before coronary angiography they
(SD) and categorical variables are presented as frequencies and
were given an initial dose of 600 mg clopidogrel. Prior to, 4 and
percentages. Continuous variables were tested for intra-individ-
24 h after clopidogrel administration, whole blood was collect-
ual differences by using Wilcoxon signed rank test and inter-
ed using citrate as anticoagulant. At some patients, blood was
individual differences were identified using the Kruskal-Wallis
test. Categorical variables were compared using chi-square
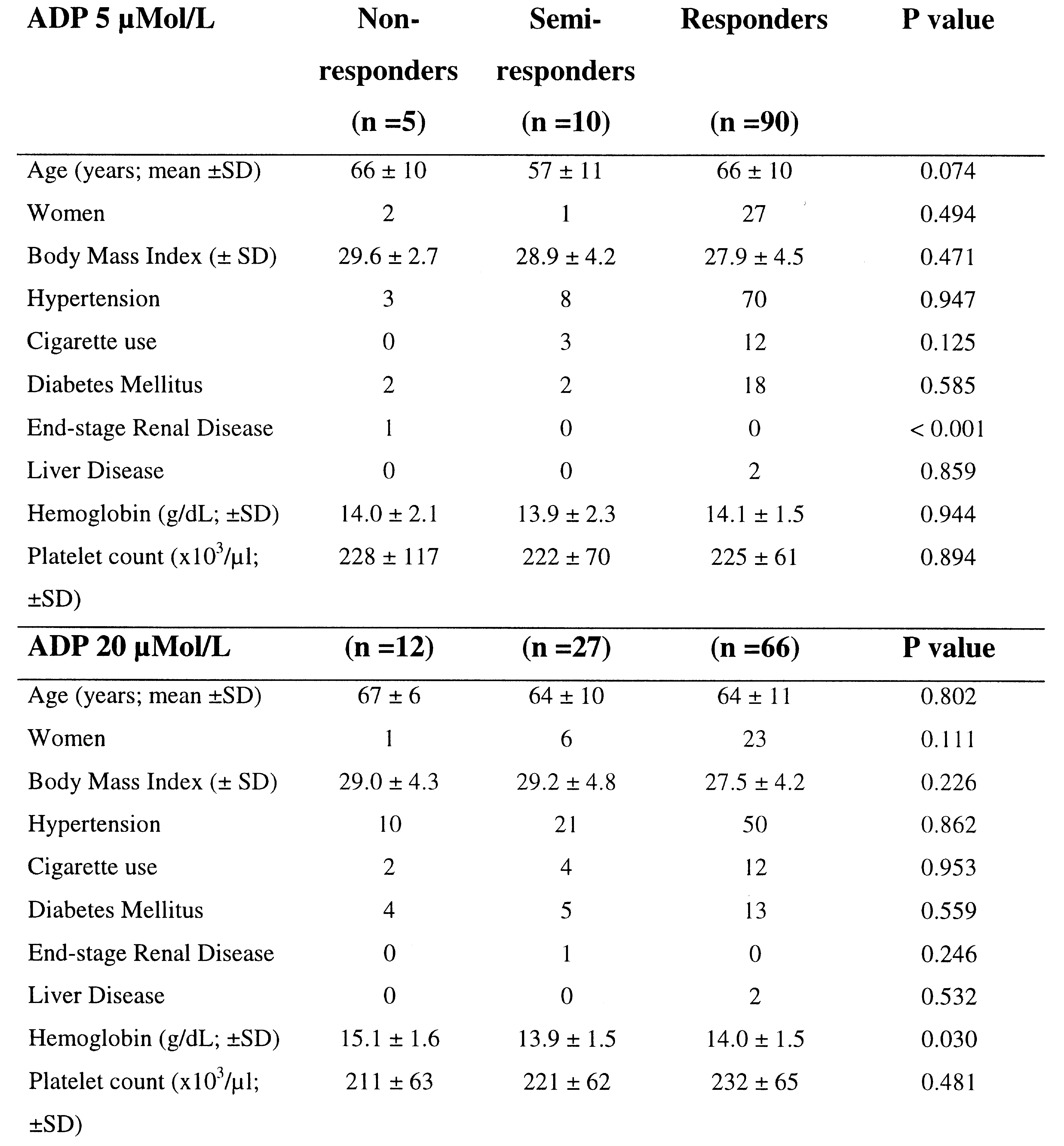
Table 1: Demographic and clinical character- istics of patients (n = 105)
Clopidogrel non-responders and coronary stenting
Table 2: Mean percentage of aggregation in non-responders, semi-responders, and responders prior to and 4 h after clopido- grel administration.
tests. Correlations were calculated by Pearson. P < 0.05 wasconsidered statistically significant. To adjust for multiple com-parisons, a significant level of 0.0125 was used.
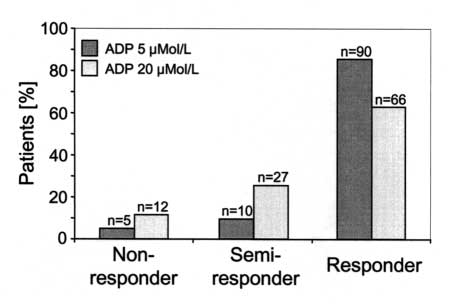
The demographic and clinical details of the 105 patients aregiven in the Table 1. Concomitant medication did not differ sig-nificantly between groups (not shown). Baseline aggregationvalues of all patients in response to 5 and 20 Mol/L ADP were65 ± 21% and 79 ± 19%, respectively. We found that 5 to 11%were clopidogrel non-responders and 9 to 26% were semi-responders, which was dependent on the concentration of ADPused to induce aggregation ex vivo (5 and 20 Mol/L). The distribution of non-responders, semi-responders, and respond-ers to clopidogrel among the 105 evaluated patients is given in
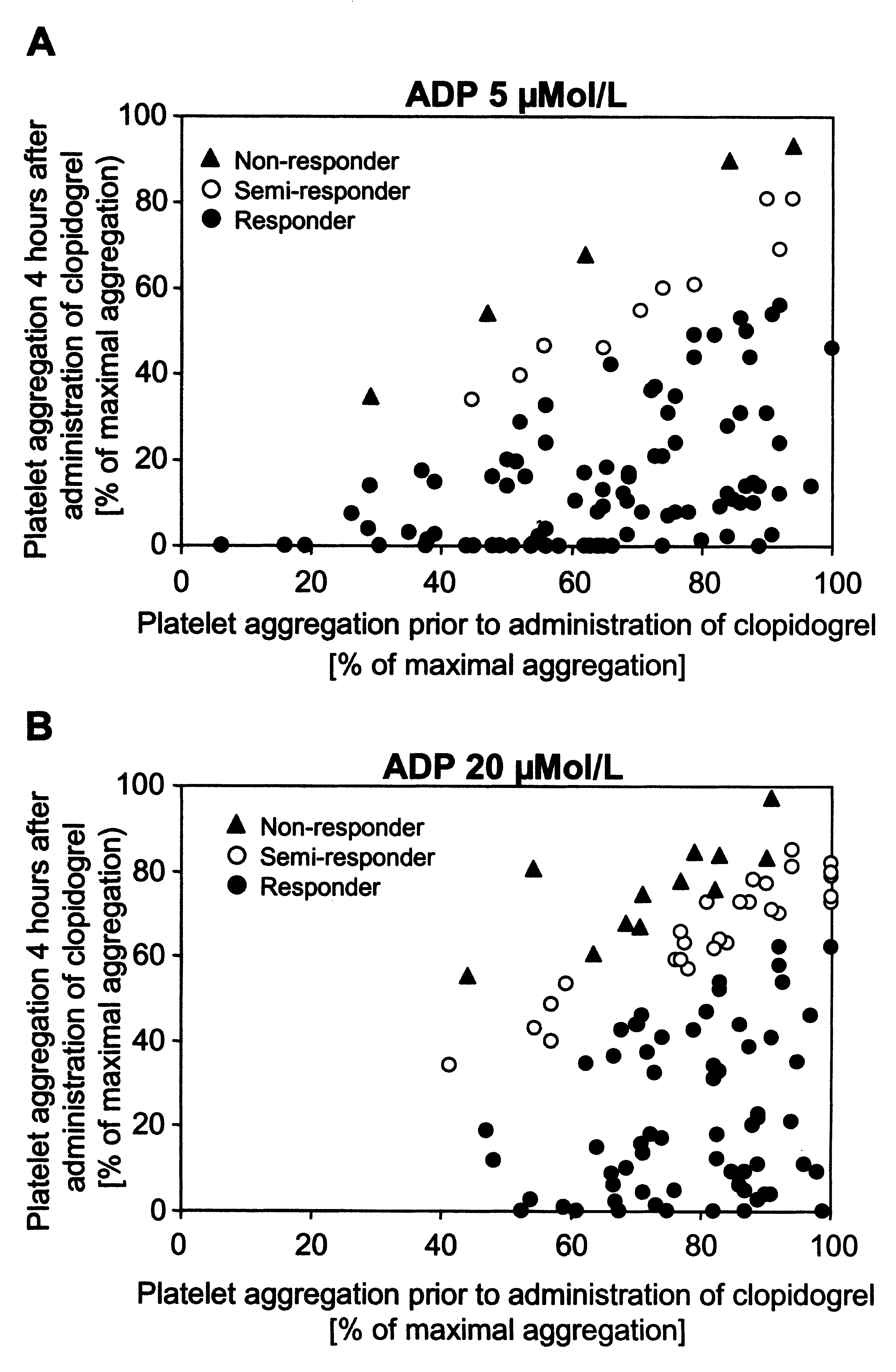
Figure 2: Effect of clopidogrel on ADP-induced platelet aggrega- tion. Depicted are individual values of maximal aggregation prior
figure 1. The mean percentage of aggregation of non-respond-
to and 4 h after clopidogrel administration in response to ADP
ers, semi-responders, and responders prior to and 4 h after
5 Mol/L (A) and ADP 20 Mol/L (B). Non-responders (trian-
clopidogrel administration is given in Table 2. Figure 2 shows
gle), semi-responders (open circle), responders (closed circle).
a scatter plot of individual aggregation values prior to and 4 hafter clopidogrel administration. Aggregation values in response
administration showed a significant intra-individual correla-
to 5 and 20 Mol/L ADP determined 4 h after clopidogrel
tion (r = 0.820; p <0.001) (Fig. 3). However, in response to 20 Mol/L, a higher number of non- and semi-responders wasfound (Fig. 2).
Platelet aggregation was additionally evaluated 24 h after
clopidogrel administration in a subgroup of patients (n = 29). Asdescribed previously (5) and as shown herein, we did not findenhanced platelet inhibition 24 h after clopidogrel administra-tion compared to the 4 h values (Fig. 4). This indicates, thatmaximal platelet inhibition is achieved already after 4 hourswhen clopidogrel is administered at an initial dose of 600 mg.
Subacute stent thrombosis occurred in two patients at day 6
and 7, respectively, after intracoronary stent placement. According to our definition both patients were non-responders(inhibition of platelet aggregation <10% after 4 h). In one of
Figure 1: Distribution of clopidogrel non-responders, semi-
these patients platelet aggregation was also assessed 14 days, in
the other patient 2 and 3 months after first administration of clo-
Figure 3: Correlation of platelet aggregation values in response Figure 4: Platelet aggregation of patients prior to (n = 105),
to 5 and 20 µMol/L ADP 4 h after administration of 600 mg clo-
4 h (n = 105) and 24 hours (n = 29) after clopidogrel adminis-
tration. Values are shown as mean ± standard deviation. An asterisksindicates a significant decrease in platelet aggregation relative tobaseline values (p <0.05).
pidogrel. In both patients platelet inhibition remained less than
ing complication after coronary stent placement and occurs in
15% (patient 1: 0% (4 h) and 6% (14 d); patient 2: 0% (4 h), 9%
approximately 1% of the patients according to studies per-
(2 months) and 13% (3 months) [% inhibition of platelet aggre-
formed in specialized interventional cardiology centers (12, 13).
However, recent data from the Duke Medical Center shows that
Retrospectively, we assessed platelet aggregation of 3 fur-
the incidence of stent thrombosis is up to approximately 5% in
ther patients, who developed subacute stent thrombosis at day 6,
unselected interventional centers (14).
8, and 28 after PCI. Platelet aggregation was assessed in the first
The present study shows that a high variability occurs in the
patient at day 15, in the second at day 24 and in the third patient
platelet inhibitory response to clopidogrel in patients with coro-
9 months after first administration of clopidogrel (patient 1:
nary artery disease. Thus, the effectiveness of combined aspi-
100%; patient 2: 100%, patient 3: 83 % [% of maximal possible
rin/clopidogrel therapy has to be questioned in a substantial sub-
platelet aggregation, ADP 20 Mol/L]). As platelet aggregation
group of patients that do not adequately respond to clopidogrel.
in these patients was subsequently assessed, no baseline value
Although the present study did not prospectively test the
prior to clopidogrel intake was available. Therefore inhibition
hypothesis that clopidogrel non-responders have an increased
of platelet aggregation could not be calculated.
risk for stent thrombosis, our data showed that 5 patients whodeveloped a stent thrombosis were non-responders. This obser-
Discussion
vation suggests that clopidogrel resistance has clinical signifi-cance and that patients with a risk for stent thrombosis may be
The present study demonstrates, that 5 (ADP 5 Mol/L) to 11%
identified by point-of care testing. The number of clopidogrel
(ADP 20 Mol/L) of patients with stable coronary artery dis-
non-responders depended on the concentration of ADP used to
ease do not respond adequately to clopidogrel therapy. An effec-
induce aggregation ex vivo. The incidence of stent thrombosis is
tive combined antiplatelet therapy consisting of aspirin and clo-
between 1 to 5%, which is comparable to the rate of clopidogrel
pidogrel is critical to prevent subacute stent thrombosis in
non-responders (5%) when 5 Mol/L ADP are used to induce
patients undergoing coronary stenting and has become the stan-
platelet aggregation. Although further studies are necessary to
dard antiplatelet treatment. Thus, clopidogrel non-responders
compare the most sensitive platelet function test to identify non-
may have an increased risk to develop subacute stent thrombo-
responders, we would suggest, based on our present study, that
sis. Periinterventional evaluation of platelet inhibition identifies
5 Mol/L instead of 20 Mol/L ADP should be used in order to
non-responders and may justify the treatment of these patients
not overestimate the rate of non-responders.
with an alternative antiplatelet strategy.
Antiplatelet drug resistence has been previously described
Acknowledgements
for aspirin (8-10) and for clopidogrel (11, 12). However, data on
The authors are indebted to Sandra Kerstan and Kirsten Langenbrink forexpert technical assistance.
the clinical significance of clopidogrel non-responders is notavailable yet. Subacute stent thrombosis is a major life-threaten-
Clopidogrel non-responders and coronary stenting
References
1. Cutlip DE, Baim DS, Ho KK, et al. Stent
6. Gawaz M, Seyfarth M, Muller I, et al.
including 180 post-stroke patients. Thromb
thrombosis in the modern era: a pooled analy-
Comparison of effects of clopidogrel versus
sis of multicenter coronary stent clinical trials.
ticlopidine on platelet function in patients
11. Järemo P, Lindahl TL, Fransson SG, Richter
undergoing coronary stent placement. Am J
A. Individual variations of platelet inhibition
2. Schomig A, Neumann FJ, Kastrati A, et al. A
after loading doses of clopidogrel. J Intern
randomised comparison of antiplatelet and
7. Gawaz M, Ruf A, Pogatsa-Murray G, et al.
anticoagulant therapy after the placement of
Incomplete inhibition of platelet aggregation
12. Sokolova O, Schnurr A, Grossmann R, Kobsar
coronary artery stents. N Engl J Med 1996;
and glycoprotein IIb-IIIa receptor blockade by
A, Schwarz U, Barragan P, Bonz A, Walter U,
abciximab: Importance of internal pool of gly-
Eigenthaler M. Experiences with clopidogrel
3. Bhatt DL, Bertrand ME, Berger PB, et al.
coprotein IIb-IIIa receptors. Thromb Haemost
in patients with coronary heart disease: are all
platelets inhibited? Ann Hematol 2002; 81,
comparisons of ticlopidine with clopidogrel
8. Helgason CM, Bolin KM, Hoff JA, Winkler
after stenting. J Am Coll Cardiol 2002; 39: 9-
SR, Mangat A, Tortorice KL, Brace LD.
13. Dangas G, Mehran R, Abizaid AS, et al.
Development of aspirin resistance in persons
Combination therapy with aspirin plus clopid-
4. Steinhubl SR, Berger PB, Mann JT 3rd, et al.
with previous ischemic stroke. Stroke 1994;
ogrel versus aspirin plus ticlopidine for pre-
Early and sustained dual oral antiplatelet ther-
vention of subacute thrombosis after success-
apy following percutaneous coronary inter-
9. Pappas JM, Westengard JC, Bull BS.
ful native coronary stenting. Am J Cardiol
vention: a randomized controlled trial. JAMA
Population variability in the effect of aspirin
on platelet function. Implications for clinical
5. Müller I, Seyfarth M, Rüdiger S, Wolf B,
trials and therapy. Arch Pathol Lab Med 1994;
Pogatsa-Murray G, Schömig A. Effect of a
high loading dose of clopidogrel on platelet
10. Grotemeyer KH, Scharafinski HW, Husstedt
function in patients undergoing coronary stent
IW. Two-year follow-up of aspirin responder
Gab Único RESIDÊNCIA MÉDICA – GASTROENTEROLOGIA – DEZEMBRO DE 2006 GA 08. Marque a droga de escolha para o tratamento GA 01. Paciente com sintomas dispépticos, apresenta à endoscopia digestiva alta, processo inflamatório comprometimento do antro gástrico e teste da urease positivo. Principal hipótese diagnóstica para esse GA 09. O tratamento da estrongiloidíase não complicada
Pfizer-Warner: One Drug Merger That Might Just Deliver The combo looks as if it will carry through with cost reductions, better marketing, and stronger R&D Whenever pharmaceutical companies merge, there’s often talk of huge cost-savings. That excites investors at first but later leaves them wondering: "Why did we believe that hype?" Case in point: Pharmacia’s merge
 platelet aggregation with maximal inhibition four hours after
Platelet aggregation and definition of clopido-
platelet aggregation with maximal inhibition four hours after
Platelet aggregation and definition of clopido-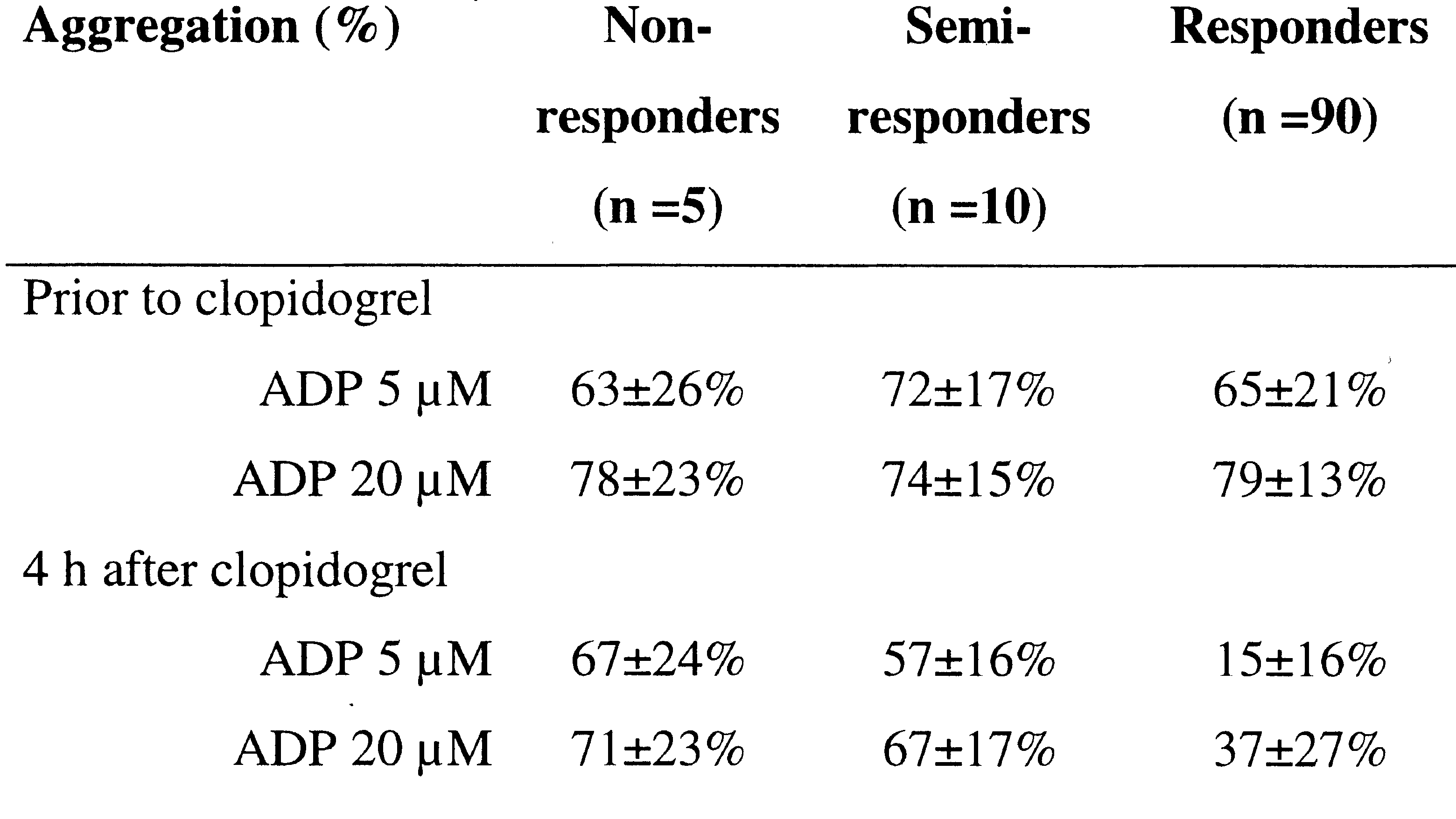
 Clopidogrel non-responders and coronary stenting
Table 2: Mean percentage of aggregation in non-responders,
Clopidogrel non-responders and coronary stenting
Table 2: Mean percentage of aggregation in non-responders,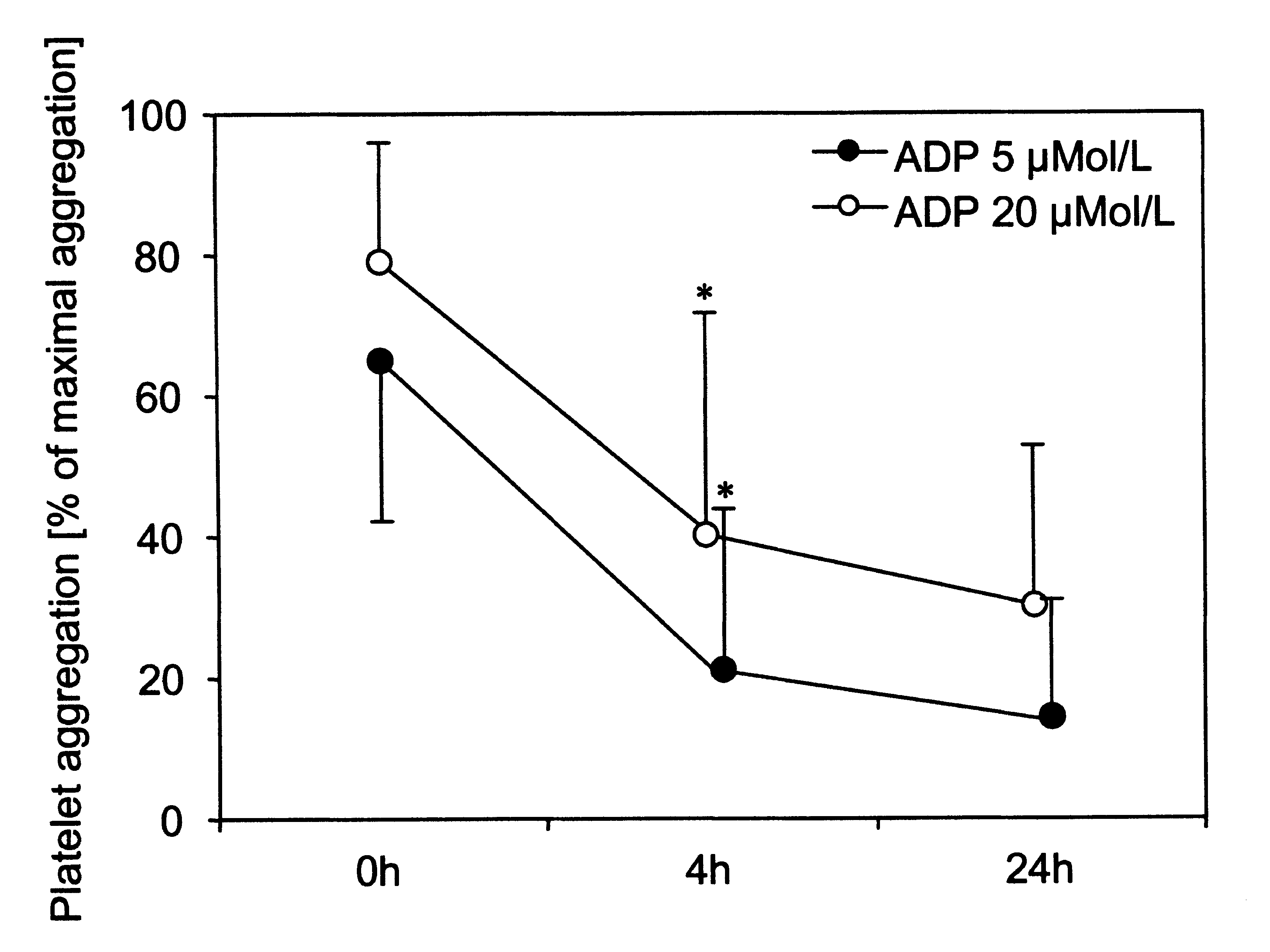
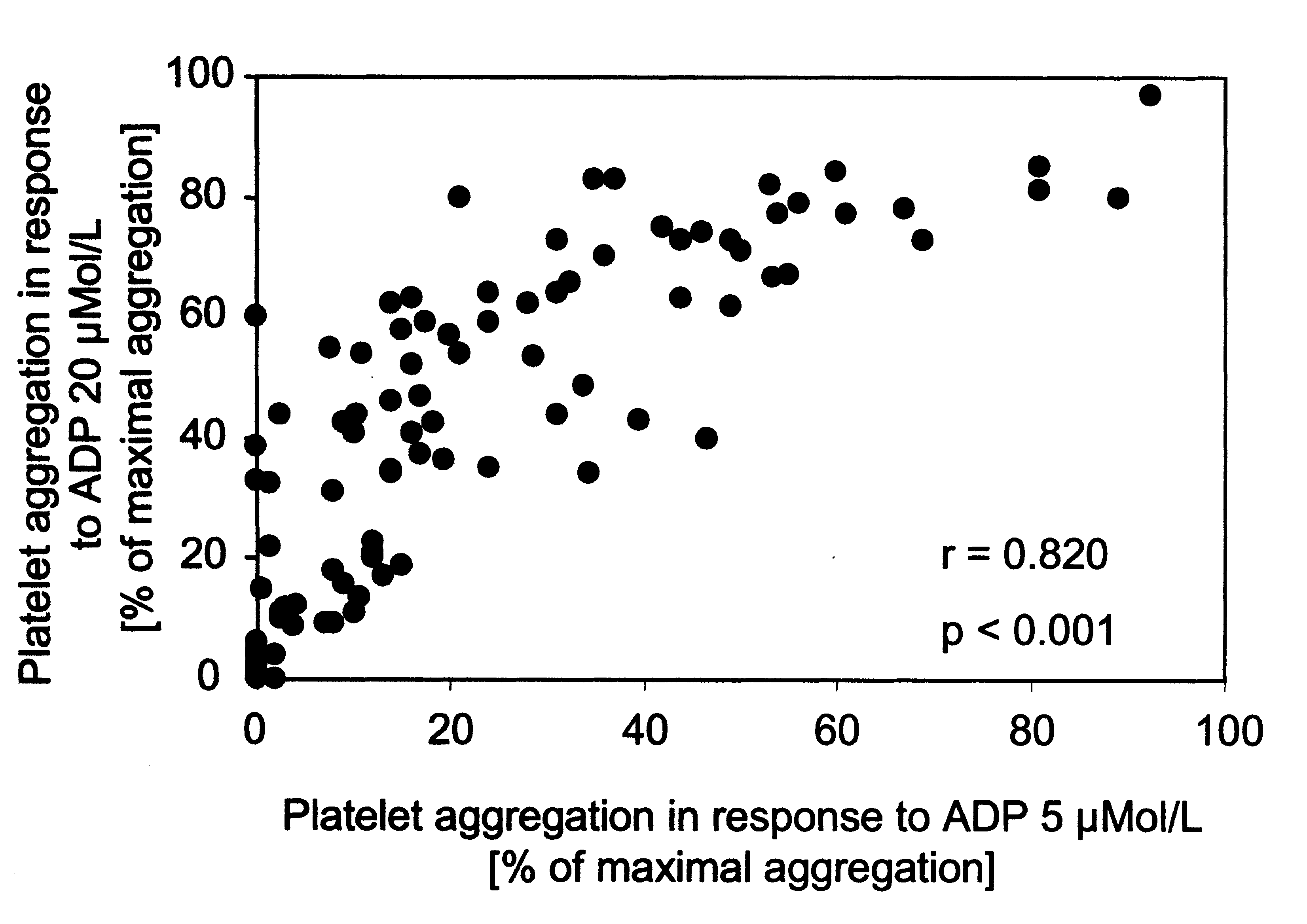 Figure 3: Correlation of platelet aggregation values in response
Figure 3: Correlation of platelet aggregation values in response