La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Untitled
PRINTER-FRIENDLY VERSION AT RHEUMATOLOGYPRACTICENEWS.COM June 2013
Rheumatology Practice News SPECIAL EDITION
All rights r Stanford University School of Medicine Copyright 2013 McMahon Publishing Gr Dr. Marcus is a retiree of Eli Lilly & Company and serves as an advisor to both Amgen Inc. and Lilly.eserved. Repr
Not long ago, FDA-approved pharmacologic
oduction in whole or in part without permission is pr
options for treating patients with osteoporosis
included an assortment of estrogen preparations
and calcitonins. Beginning in the mid-1990s, the
introduction of a potent aminobisphosphonate,
alendronate (Fosamax, Merck), and a selective
oup unless otherwise noted.
estradiol receptor modifier (SERM), raloxifene (Evista,
Eli Lilly), began a decade-long era of dominance
over the osteoporosis market by these 2 agents.
The past decade has witnessed field, with consideration of important
ber of approved drugs for the has accumulated. Finally, I will not dis-
excavated by resorbing cells, called remodeling event is slightly ineffi-
treatment of osteoporosis, giving cuss the hygienic measures, supple-
osteoclasts, which arise in the bone
ohibited.
concerns regarding drugs currently the concomitant adequate intake of
osteoclastic resorption is initiated, fol-
ment of osteoporosis in the United tion under which the clinical trials that
established efficacy of all approved stroma called preosteoblasts migrate
into the resorption cavity, acquire that any increase in the overall rate
process of breakdown and renewal Physiology: Bone Remodeling
ing osteoblasts, and begin to replace
eton. The literature on osteoporosis iarity with remodeling to understand
therapeutics is now enormous, and the mechanisms of action of osteopo-
between 6 and 8 weeks, and the subsequent bone formation response,
resulting hole, or lacuna, achieves antiresorptive therapy, regardless of
Hence, where possible I will refer tion—the antiresorptive drugs—and a depth of about 60 microns. The which agent is considered, ultimately the reader to pivotal studies of indi-
However, even in normal adults, siderable understanding about the
June 2013
Rheumatology Practice News SPECIAL EDITION
Table. FDA-Approved Agents for Osteoporosis Prevention and/or Treatment
clasts. Osteoclast precursor cells in the bone marrow contain the RANK
factor-κB) gene. RANK is ubiquitous in multiple cells in the macrophage
osteoclast response to a stimulatory protein produced by osteoblasts
All rights r
Prevention and treatment; administered annually by
Copyright 2013 McMahon Publishing Gr eserved. Repr
Prevention and treatment; administered every 6 mo
the dynamics of osteoclast produc-tion. OPG is considered a “decoy”
OPG restricts access to RANK, and
oduction in whole or in part without permission is pr
thereby puts a brake on osteoclast development. The great majority of
Treatment of patients with osteoporosis and GIOP
Teriparatide (hPTH[1-34]) (Forteo, Eli Lilly)
at high risk for fracture; administered as once-daily
agent, teriparatide (Forteo, Eli Lilly) is approved in the United States,
GIOP, glucocorticoid-induced osteoporosis; SERMs, selective estrogen receptor modulators
although others are undergoing clin-ical trials. oup unless otherwise noted. Agents Approved for the
Evidence from the Women’s Health clinical trials over the past 15 years, later, the optimal time for using ralox-
Prevention and Treatment of Osteoporosis
on nonvertebral fracture,2,3 but in that
agency policy, osteoporosis drugs ease4 and breast cancer5 tempered able toxicity in other organ systems,
therapy. For women with an intact 60 mg daily, raloxifene is consid-
istration of a progestin to prevent tive agent. Treatment leads rapidly hyperplasia. Some women respond endometrial hyperplasia. In the WHI,
tant contributor to the mentioned (BMD) of the lumbar spine, although
Various estrogen preparations side effects. Following release of the
ohibited.
osteoporosis in postmenopausal gen use in the United States quickly
plummeted and has not recovered. ture, but generally has not shown it does offer skeletal protection to
dominant form used in the United Estrogen remains the most effective
approach for managing hot flashes, sites.6 Large randomized clinical tri-
and current recommendations state als with nonvertebral fracture as an trial hyperplasia and is associated
erally based on anecdotal reports as short a time as is required. Such porosis do indicate a beneficial effect
among women in the most severe Bisphosphonates
sively more common even shortly pound, pyrophosphate, but have a
SERMs have undergone late-phase consideration until at least 2 decades
June 2013
Rheumatology Practice News SPECIAL EDITION
details of their molecular structure. some of these differences reflect only
All rights r
less of structure, bisphosphonates ing remains low as long as the drugs share certain characteristics. They are
Copyright 2013 McMahon Publishing Gr
tine (<2%), therefore patients must bisphosphonates lead within a few take special precautions when using
eserved. Repr
an oral form of the medications. bone formation and are thus entirely
able) when the drug is consumed, used as a surrogate marker for drug and remaining upright for 30 minutes
oduction in whole or in part without permission is pr Figure 1. The drawing represents a region of trabecular bone.
the initiation of therapy refill but are
All remodeling events occur on the bone surface. (a) 90% of bone surface is generally covered by a thin layer of dormant lining cells. (b) Coalescence
of osteoclast precursors at a site on the bone surface with creation of mul-
tinucleated osteoclasts. (c) Osteoclasts remove a divot of bone, reach-
All approved bisphosphonates rate, each trabecula has a longer
ing 60 microns in depth by 6 to 8 weeks. (d) Soluble factors released by
achieve a substantial reduction in period to acquire mineral until a sub-
osteoclastic resorption recruit a new wave of cell proliferation (preosteo-
vertebral compression fractures, sequent remodeling event affects it.
blasts) into the base of the resorption cavity. (e) Preosteoblasts acquire
oup unless otherwise noted.
the osteoblast phenotype. (f) Osteoblasts secrete new bone matrix, which
begins to acquire mineral after a thickness of approximately 20 microns is
reduce nonvertebral fractures as eral per unit of bone matrix increases
achieved. (g) New mineralized bone almost fully replaces resorbed bone
by approximately 6 months. Small deficits are left, reflecting remodeling
inefficiency and accounting for the process of age-related bone loss.
Similarly, in a large clinical trial, rise-
with osteoporosis, but a subset of fracture efficacy, and with raloxifene
crystallized over the appearance of nature of atypical fractures for those
older frail patients who had only this estimate is only about 11%. Other
The most dramatic effects of tion in the prevalence of osteoclast
tures are unusual, but appear to be incidenc
ohibited. e of fracture has persistently
observed with the parenteral agent bone, as these constitute regions of
fragility and increased fracture risk.
1,000 participants who already had nates incorporate tenaciously into distance between the upper end of constitute a small proportion of the experienced a hip fracture, this agent
bone and remain there for years. the femur and the knee. Hence, they
bisphosphonates rose with reports ical stress fractures. Atypical fractures
that some patients appeared with frequently are bilateral, the contralat-
complication was rare and, for the on the opposite femur. The fracture
not required additional label changes.
fracture site, localized periosteal reac-
Considerable pharmaceutical tine dental care if they were taking
tion, or “beaking,” of the lateral cortex
industry effort has been made to bisphosphonates.
More recently, concern has both cortices.11 Despite the serious in 2- and 3-year clinical trials, the
June 2013
Rheumatology Practice News SPECIAL EDITION
Denosumab (Prolia, Amgen) is calcitonin, which as a nasal spray is
a human monoclonal antibody to indicated for the treatment of post-RANKL that blocks its binding to menopausal osteoporosis. At the RANK and thereby inhibits the pro-
duction and actions of osteoclasts, nasal spray calcitonin inhibits osteo-leading to a substantial reduction in
at the approved dose of 60 mg. a decrease in vertebral, but not non-The pivotal 36-month clinical trial vertebral fracture; however, this trial
All rights r Copyright 2013 McMahon Publishing Gr
hip fracture.16 Denosumab was well that it is associated with an overall
eserved. Repr
tolerated, and showed no increase increased risk for malignancies, and in serious infections or malignancy.
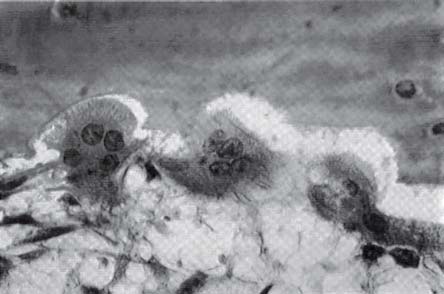
Figure 2. Osteoclasts in resorption lacunae.
Reproduced from Lee C, Einhorn T: In Marcus R, Feldman D, Kelsey J
RANK is an active participant in the
(Eds.). Osteoporosis, 2nd Edition, Academic Press 2001, with permission
action likely will result in limitation or
oduction in whole or in part without permission is pr
A key feature of denosumab is the United States, but as of this writ-
that, unlike bisphosphonates, the ing the FDA has not rendered a final
little additional therapeutic effect drug does not accumulate in the skel-
and even less-frequent regimens. concept, but a reasonable approach
to make significant inroads on the First, it can be argued that some ceptible to ONJ and atypical frac-
patients who originally had mild tures, but that has not been the end” of the molecule
oup unless otherwise noted.
Alendronate was the first oral deficits in BMD (ie, BMD T scores case; the occurrence of both events
porosis market, and consequently qualify for the designation of osteo-
tion it still occupies. In recent years,
scribed bisphosphonates to begin with denosumab has not been exten-
alendronate has been available as with. In such cases, termination of sive, and the causality of this drug for
a generic oral product. Although therapy after 4 to 5 years is appro-
generic drugs must show identical priate. In others, a good therapeutic
a lower risk for fracture, and it should
gle-chain polypeptide hormones sequence and understand the struc-
ohibited.
over time. However, some patients the primary secretory product of the
lished that generic alendronate despite a substantial improvement cies, and in humans they are pro-
duced and secreted by the C cells species. Trials of this peptide con-
ing gastrointestinal symptoms, and tion, it seems inappropriate to termi-
appear primarily to be involved in osteoporosis throughout the 1980s
calcium homeostasis, inhibiting the and 1990s demonstrated substan-
non-bisphosphonate) of drug may actions of mature osteoclasts and tial increases in BMD at the spine
showing phosphaturic effects on and proximal femur. The pivotal trial
the renal tubule. Demonstrating an of recombinantly produced TPTD
term bisphosphonate use, many and atypical fractures have been as even individuals who have under-
gone total thyroidectomy—and incidence of moderate and severe
patients stop therapy after 4 to 5 resorptive therapy, although it is therefore produce no calcitonin—
still too early to know the extent have normal skeletal physiology.
ies widely among animal species; tered daily subcutaneous injection at
June 2013
Rheumatology Practice News SPECIAL EDITION
antifracture efficacy is essential. In the
men and postmenopausal women apy, the important feature is simply to
therapy. Eur Radiol. 2012;23(1):222-227.
induced osteoporosis. The duration sorptive agent should be useful.
Several studies have addressed future therapies in medical practice
months. This limit reflects the fact that
Mineral Research. J Bone Miner Res.
treatment efficacy and safety have therapy with TPTD and an antire-
not been established beyond that sorptive drug might offer additive or
References
femoral fractures: report of a task force
All rights r
ies have not achieved encouraging 1. Lindsay R, Hart DM, Forrest C, Baird
Mineral Research. J Bone Miner Res.
in oöphorectomized women. Lancet. Copyright 2013 McMahon Publishing Gr
Effects of estrogen plus progestin on risk
of fracture and bone mineral density: the
eserved. Repr
certainty, although it is reassuring that
Women’s Health Initiative randomized trial.
JAMA. 2003;290(13):1729-1738.
regimen that has been shown to 3. Jackson RD, Wactawski-Wende J,
1-year results of a retrospective patient
LaCroix AZ, et al. Effects of conjugated
coma safety signal has been detected.
chart review analysis. Rheumatol Int.
equine estrogen on risk of fractures and
The anabolic action of TPTD is fracture is monotherapy with TPTD
BMD in postmenopausal women with hysterectomy: results from the Women’s
largely achieved through activation at a daily dose of 20 mcg.
15. Lai PS, Chua SS, Chong Y, Chan SP. The
Health Initiative randomized trial. J Bone oduction in whole or in part without permission is pr
effect of mandatory generic substitution
Miner Res. 2006;21(6):817-828.
patients’ adherence. Curr Med Res Opin.
et al. Postmenopausal hormone therapy and risk of cardiovascular disease by
blasts without an initial resorption other antiresorptive agents may
age and years since menopause. JAMA.
eling is not perfectly efficient, an than 400 postmenopausal women 5. Chlebowski RT, Hendrix SL, Langer RD,
et al. Infl uence of estrogen plus progestin
Trial. JAMA. 2003;289(24):3243-3253.
17. Chesnut CH III, Silverman S, Andriano K, et
oup unless otherwise noted.
al. A randomized trial of nasal spray salmon
3-year randomized clinical trial. JAMA.
study. PROOF Study Group. Am J Med.
7. Delmas PD, Genant HK, Crans GG, et al.
Severity of prevalent vertebral fractures
18. Neer RM, Arnaud CD, Zanchetta JR, et
and the risk of subsequent vertebral and
al. Effect of parathyroid hormone (1-34)
nonvertebral fractures: results from the MORE trial. Bone. 2003;33(4):522-532.
on fractures and bone mineral density in
8. Black D, Cummings SR, Karpf DB, et al.
the United States was not successful.
Alendronate reduces the risk of fractures
N Engl J Med. 2001;344(19):1434-1441.
in women with existing vertebral fractures:
After a course of TPTD therapy Conclusion
results of the Fracture Intervention Trial. Lancet. 1996;348(9041):1535-1541.
interpretation of rat carcinogenicity studies
9. McClung MR, Geusens P, Miller PD, et al.
for PTH (1–34) and human PTH (1–84).
Effect of risedronate on the risk of hip
J Bone Miner Res. 2008;23(6):803-811.
tive drug to maintain the benefits both the antiresorptive and anabolic
fracture in elderly women. N Engl J Med. ohibited.
20. Cosman F, Eriksen EF, Recknor C, et al.
that have been achieved. With this categories. Inhibitors of the enzyme
Effects of intravenous zoledronic acid plus
approach, treatment goals for the cathepsin-K, an important part of 10. Lyles KW, Colón-Emeric CS, Magaziner JS,
et al. Zoledronic acid and clinical fractures
in postmenopausal osteoporosis. J Bone
and mortality after hip fracture. N Engl J
from those applicable to first-line submitted for FDA approval within
Miner Res. 2011;26(3):503-511.
Levée des barrages à La Paz , après des semaines de contestations Levée des barrages à La Paz , après des semaines de contestations Date de mise en ligne : lundi 13 juin 2005 Levée des barrages à La Paz , après des semaines de contestations Les dirigeants de la banlieue pauvre d'El Alto qui surplombe La Paz à 4200 mètres d'altitude et où est née la contestation de c
on Christianity and understanding of its basic truths. At Muslims usually want to know God; this is your op-the same time, get to know his/her level of understanding of Islam; get to know how seriously they follow Islam and Do not be arrogant; it is not the strength of your ar-guments that will win the person, but the conviction of the Holy Spirit. Always be prepared to share the Gospel. Pre

 PRINTER-FRIENDLY VERSION AT RHEUMATOLOGYPRACTICENEWS.COM
PRINTER-FRIENDLY VERSION AT RHEUMATOLOGYPRACTICENEWS.COM


 June 2013
June 2013 

 June 2013
June 2013



 June 2013
June 2013