La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Pio.uad.ac.id
Pharmacodynamic and Pharmacokinetic Study of Oral Extract in Patients with Colorectal Cancer Curcuma
Ricky A. Sharma, Heather R. McLelland, Kirsti A. Hill, et al. Updated Version
Access the most recent version of this article at:
Cited Articles
This article cites 44 articles, 15 of which you can access for free at:
Citing Articles
This article has been cited by 38 HighWire-hosted articles. Access the articles at:
E-mail alerts Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Subscriptions Permissions
To request permission to re-use all or part of this article, contact the AACR PublicationsDepartment at
1894 Vol. 7, 1894 –1900, July 2001 Pharmacodynamic and Pharmacokinetic Study of Oral Curcuma Extract in Patients with Colorectal Cancer1 Ricky A. Sharma,2 Heather R. McLelland, cuma extract can be administered safely to patients at doses Kirsti A. Hill, Christopher R. Ireson, of up to 2.2 g daily, equivalent to 180 mg of curcumin; (b) curcumin has low oral bioavailability in humans and may Stephanie A. Euden, Margaret M. Manson, undergo intestinal metabolism; and (c) larger clinical trials Munir Pirmohamed, Lawrence J. Marnett, of Curcuma extract are merited. Andreas J. Gescher, and William P. Steward Oncology Department [R. A. S., H. R. M., K. A. H., S. A. E., INTRODUCTION
W. P. S.] and Medical Research Council Toxicology Unit [A. J. G.,
Curcumin (diferuloylmethane), a low molecular weight
C. R. I., M. M. M.], University of Leicester, Leicester LE1 9HN,United Kingdom; Department of Pharmacology and Therapeutics,
polyphenol derived from the rhizomes of Curcuma spp., has
University of Liverpool, Liverpool L69 3GE, United Kingdom
been shown to prevent cancer in the skin, forestomach, duode-
[M. P.]; and Vanderbilt Cancer Center, Nashville, Tennessee 37232
num, and colon of mice and in the tongue, colon, mammary
glands, and sebaceous glands of rats (1). Of particular interest isthe ability of dietary curcumin to interfere with colon carcino-
ABSTRACT
genesis in chemical and genetic rodent models (2– 4). Curcuminhas also been associated with regression of established malig-
Curcuma spp. extracts, particularly the dietary poly-
nancy in humans (5). Curcumin is the major constituent of the
phenol curcumin, prevent colon cancer in rodents. In view of
spice turmeric, which is abundantly used in the diet on the
the sparse information on the pharmacodynamics and phar-
Indian subcontinent, an area that has a low incidence of colo-
macokinetics of curcumin in humans, a dose-escalation pilot
rectal cancer (6). Mechanisms by which curcumin prevents
study of a novel standardized Curcuma extract in proprie-
cancer are thought to involve up-regulation of carcinogen-
tary capsule form was performed at doses between 440 and
detoxifying enzymes, such as GSTs3 (7–9), antioxidation (10 –
2200 mg/day, containing 36 –180 mg of curcumin. Fifteen
16), and suppression of expression of the enzyme cyclooxyge-
patients with advanced colorectal cancer refractory to
nase-2 (17, 18). The pharmacokinetic properties of curcumin in
standard chemotherapies received Curcuma extract daily
humans remain unexplored. In rodents, curcumin undergoes
for up to 4 months. Activity of glutathione S-transferase and
avid metabolism by conjugation and reduction, and its disposi-
levels of a DNA adduct (M G) formed by malondialdehyde,
tion after oral dosing is characterized by poor systemic bioavail-
a product of lipid peroxidation and prostaglandin biosyn- thesis, were measured in patients’ blood cells. Oral Curcuma
In view of the paucity of pharmacodynamic and pharma-
extract was well tolerated, and dose-limiting toxicity was not
cokinetic information regarding curcumin in humans, we con-
observed. Neither curcumin nor its metabolites were de-
ducted a dose-escalation pilot study of a standardized Curcumatected in blood or urine, but curcumin was recovered from
extract in patients with advanced colorectal cancer refractory to
feces. Curcumin sulfate was identified in the feces of one
standard chemotherapy. The aims of the study were threefold. patient. Ingestion of 440 mg of Curcuma extract for 29 days
Firstly, we wished to evaluate the safety of curcumin adminis-
was accompanied by a 59% decrease in lymphocytic gluta-
tered p.o. as Curcuma extracts. Secondly, we wanted to inves-
thione S-transferase activity. At higher dose levels, this ef-
tigate the suitability of two potential biomarkers of the pharma-
fect was not observed. Leukocytic M G levels were constant
cological efficacy of curcumin in patients’ blood leukocytes:
within each patient and unaffected by treatment. Radiolog-
GST activity and the levels of the adduct (M G) formed by the
ically stable disease was demonstrated in five patients for
reaction of malondialdehyde with deoxyguanosine in DNA. 2– 4 months of treatment. The results suggest that (a) Cur-
GST enzyme activity has been shown to be up- or down-regulated in rat tissues after oral curcumin treatment, dependingon the dose and route of administration (7–9). To aid theinterpretation of GST activity data, patients were genotyped for
Received 2/1/01; revised 4/10/01; accepted 4/13/01. GSTM1, GSTT1, and GSTP1. These represent the three major
The costs of publication of this article were defrayed in part by the
GST subclasses found in human lymphocytes, at least one of
payment of page charges. This article must therefore be hereby marked
which is relevant to colorectal cancer and resistance to chemo-
advertisement in accordance with 18 U.S.C. Section 1734 solely toindicate this fact. 1 Supported by program grants from the United Kingdom MedicalResearch Council (to A. J. G. and M. M. M.), funds from Phytopharmplc. (to W. P. S.), NIH Grant CA77839 (to L. J. M.), and a fellowshipfrom the University Hospitals of Leicester (to R. A. S.).
3 The abbreviations used are: GST, glutathione S-transferase; NSAID,
2 To whom requests for reprints should be addressed, at Chemopreven-
nonsteroidal anti-inflammatory drug; HPLC, high-performance liquid
tion Research Group, Oncology Department, University of Leicester,
chromatography; CEA, carcinoembryonic antigen; CT, computed to-
Leicester LE1 9HN, United Kingdom. Phone: 44-116-252-5541; Fax:
mography; CDNB, 1-chloro-2,4-dinitrobenzene; AUC, area under
44-116-252-5616; E-mail: ras20@le.ac.uk.
Clinical Cancer Research 1895
therapy (21–23). Malondialdehyde is a naturally occurring prod-
uct of lipid peroxidation and prostaglandin biosynthesis via
Daily dose of Curcuma extract (mg)
cyclooxygenase (24, 25). These two cellular processes impli-cated in the pathogenesis of colorectal cancer (26, 27) are
inhibited by curcumin in preclinical models (17, 28). In a recent
study in rats, dietary curcumin was shown to up-regulate GST
activity in the liver and diminish M G levels in colon mucosa,
and these effects were accompanied by measurable tissue levels
of curcumin (9). The third aim of the study described here was
therefore to test the hypothesis that curcumin or products of its
metabolism can be detected in blood or excreta of humans.
Overall, the study was designed to define parameters that might
help to optimize the clinical evaluation of curcumin in Phase I/II
PATIENTS AND METHODS Patients.
The trial was approved by the local ethics com-
mittee and the United Kingdom Medicines Control Agency.
Fifteen patients enrolled between September 1999 and Septem-
ber 2000 at the Leicester Royal Infirmary met the followingeligibility criteria: (a) histologically proven adenocarcinoma of
the colon or rectum for which no further conventional therapies
were available; (b) measurable or evaluable disease; (c) age Ͼ
18 years; (d) WHO performance status of 0 –2 and life expect-
ancy greater than 12 weeks; (e) absolute neutrophil count Ն1.5 ϫ 109/liter; (f) hemoglobin Ն 10 g/dl; (g) platelets Ն 100 ϫ109/liter; (h) aspartate aminotransferase and alanine aminotrans-ferase Ͻ 2.5 ϫ the upper limit of normal; (i) serum bilirubin and
three patients per dose level. After at least a 2-h fast, patients
creatinine Ͻ 1.5 ϫ the upper limit of normal; and (j) no previous
consumed 2, 4, 6, 8, or 10 capsules once daily with water. This
investigational or chemotherapeutic drugs within 28 days prior
translates to doses of 440, 880, 1320, 1760, and 2200 mg of
to enrollment. Exclusion criteria included: (a) active chronic
Curcuma extract per day containing 36, 72, 108, 144, and 180
inflammatory or autoimmune disease; (b) active infection, in-
mg of curcumin, respectively. Treatment was continued until
cluding viral infection; (c) significant impairment of gastroin-
disease progression was established or consent was withdrawn.
testinal function or absorption; (d) active peptic ulcer disease;
Clinical Measurements.
(e) known biliary obstruction or biliary insufficiency; and (f) use
collected on days 1, 2, 8, and 29 and protected from light and
of NSAIDs within 14 days of enrollment. Patients were asked to
stored at Ϫ80°C. Blood was collected before dose administra-
abstain from NSAID use and the consumption of foods contain-
tion and at 0.5, 1, 2, 3, 6, and 8 h after dose administration.
ing the spice turmeric during the study period, and their general
Samples were collected in tubes pretreated with lithium-heparin
practitioners were asked not to prescribe NSAIDs. Written in-
(Sarstedt, Loughborough, United Kingdom). Full blood cell
formed consent was obtained from each patient before enroll-
count and urea, electrolytes, liver, and bone function were
ment. Demographic and baseline characteristics of patients are
measured in venous samples, and physical examination was
shown in Table 1. All patients were Caucasian, and all had
performed before treatment and on treatment days 1, 2, 8, and
undergone previous surgery. Three patients stopped NSAID
29 and monthly thereafter. Venous blood levels of the tumor
medication 3 weeks before enrollment.
markers CEA and CA19.9 were measured before treatment and
Study Design and Treatment.
after every month of treatment. Radiological assessment of
soft gelatin capsules by Phytopharm plc. (Godmanchester,
target lesions was performed every 2 months by CT or magnetic
United Kingdom). Each capsule contained 20 mg of curcumi-
resonance imaging scan, in addition to monthly chest X-rays.
noids (18 mg of curcumin and 2 mg of desmethoxycurcumin)
Blood samples for analysis of GST activity and M G levels
suspended in 200 mg of essential oils derived from Curcuma
were collected 1 week before treatment and on days 1, 2, 8, and
spp. Typical constituents of Curcuma essential oil mixtures are
29 of treatment, immediately before dosing for M G or imme-
tumerone, atlantone, and zingiberene. Chemical analysis by
diately before and 1 h after each dose for GST. Lymphocytes
HPLC/mass spectrometry confirmed the content of curcumi-
were separated from fresh blood using Ficoll-Paque Plus (Am-
noids. This formulation, which in the following text will be
ersham Pharmacia Biotech, Bucks, United Kingdom), resus-
referred to as “Curcuma extract,” was selected on account of the
pended in 1 ml of 10 mM Tris-HCl (pH 7.8), and stored at
curcumin dose, which equates to dietary intake of turmeric (see
Ϫ80°C. Patients completed the European Organization for Re-
below), the reproducibility of curcuminoid content, and the fact
search and Treatment of Cancer quality of life questionnaire
that the capsules contained extracts of Curcuma plants used in
GLQ-C30 (version 2.0) before treatment and monthly during
traditional Indian and Southeast Asian medicine. There were
1896 Study of Oral Curcuma in Patients with Colorectal Cancer Chemical Analysis.
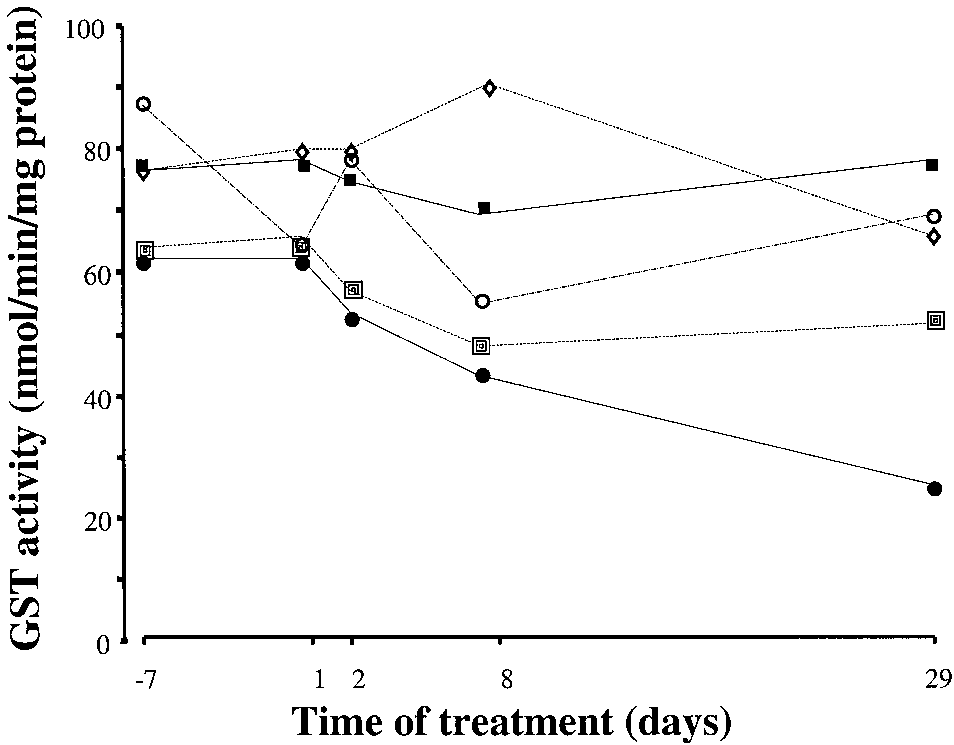
tabolites curcumin glucuronide, curcumin sulfate, hexahydro-curcumin, and hexahydrocurcuminol from plasma and urine wasperformed, and their recovery efficiency was established, asdescribed previously (17). Curcumin and curcumin sulfate wereextracted from feces with 2 parts (w/v) of acetonitrile:water(7:3). Curcuminoids were separated from other fecal constitu-ents by C18 solid phase extraction (Varian, Walton-on-Thames,United Kingdom) and eluted from the column with acetonitrile(2 ml). The reverse-phase HPLC method with UV-visible de-tection used to analyze curcuminoids in extracts of plasma,urine, or feces has been reported previously (17). The limit ofdetection for curcumin in plasma and urine was 5 pmol/ml. Thesynthesis of curcumin sulfate and its identification by electro-spray mass spectrometry were performed as described previ-ously (17). Measurement of GST Activity and M G Levels. Fig. 1 Mean lymphocytic GST levels for patients on the following
Glutathione and CDNB were purchased from Sigma Chemi-
daily doses of Curcuma extract: 440 (F), 880 (concentric squares),
cal Co. (Poole, United Kingdom). Once thawed, lymphocyte
1320 (छ), 1760 (f), and 2200 mg (E), containing 36, 72, 108, 144, and
samples were sonicated for 30 s (Fisher 550 sonicator; Fisher,
180 mg of curcumin, respectively. Each point represents means of
Pittsburgh, PA) on ice and centrifuged at 3000 ϫ g (15 min,
values for three patients, calculated from triplicate readings for two
4°C). Total GST activity in the supernatant was measured
samples per patient per day (immediately before dose administration and1 h after dose administration). Time is relative to first dose on day 1. The
spectrophotometrically using glutathione and CDNB as sub-
pooled SD, including all data points, is 10.9 nmol/min/mg protein. For
strates, in triplicate for each sample (30). Results were cor-
details of patients and measurement, see “Materials and Methods.”
rected for protein levels using the Bio-Rad protein assay(Bio-Rad, Hemel Hempstead, United Kingdom). The GSTactivity values were quoted as nmol CDNB conjugated withglutathione/min/mg
experienced nausea during the first month of treatment (Nation-
GSTT1, and GSTP1 genotypes were determined by PCR
al Cancer Institute toxicity grade 1), which resolved spontane-
methods described previously (31, 32). Murine M G mono-
ously despite continuation of treatment. Two patients (one each
clonal antibody D10A1 was prepared as described previously
on 880 and 2200 mg of Curcuma extract daily) developed
(33). Antirabbit and antimurine horseradish peroxidase anti-
diarrhea (National Cancer Institute grades 2 and 1, respectively)
bodies were purchased from Dako (Ely, United Kingdom).
4 months and 1 month into treatment, respectively. Both patients
M G standards were synthesized and characterized, genomic
withdrew from the study before the cause of the diarrhea could
DNA was extracted from whole blood, and leukocytic M G
adduct levels were analyzed by immunoslot blot in triplicate
Pretreatment GST and M G Levels in Relation to
as described previously (34). Discrepancies in the amount of
GST Polymorphisms.
DNA/slot were corrected for by staining the nitrocellulose
leukocytic M G levels differed substantially between patients
filter with propidium iodide and performing UV light densi-
(Figs. 1 and 2). Patients were genotyped for GST isoenzymes
tometry (9). The detection limit for M G was 5 adducts/108
GSTM1, GSTP1,and GSTT1. Two-thirds of the patients
nucleotides. The assay had been validated previously by
lacked GSTM1, slightly more than the 40 – 60% proportion
collaborating laboratories at the University of Leicester and
expected in healthy Caucasians (21), with an even distribu-
the Vanderbilt Cancer Center by exchange of samples.
tion across the five dose levels. In patients who displayed the
Statistical Evaluation.
null genotype for GSTM1, pretreatment levels of leukocytic
jected to a balanced repeated measure ANOVA and linear
M G were 7.6 Ϯ 4.3 adducts/107 nucleotides, 74% higher
regression analysis using Minitab (version 10.2) software pack-
than those in patients expressing GSTM1, in whom adduct
age. Plots of residuals were used to ensure that variances were
levels were 4.3 Ϯ 2.6 adducts/107 nucleotides (P Ͻ 0.001 by
homogeneous and that the residuals had a normal distribution.
ANOVA). Two patients were null for GSTT1. Their pretreat-ment levels of leukocytic M G (mean levels pooling triplicate
readings from both time points, 5.8 Ϯ 1.6 adducts/107 nu-
cleotides) were marginally lower than those in patients ex-
Tolerability of Oral Curcuma Extract.
pressing GSTT1 (6.6 Ϯ 4.3 adducts/107 nucleotides; P ϭ 0.02
advanced colorectal cancer ingested P54FP capsules once daily
by ANOVA). Leukocytic levels of M G did not correlate
for up to 4 months at doses between 440 and 2200 mg of
with total GST activity, active smoking status (n ϭ 2),
Curcuma extract containing between 36 and 180 mg of curcu-
vegetarianism (n ϭ 2), or age.
min. The treatment was well tolerated at all dose levels, and
Biological Effects of Oral Curcuma Extract.
there was no dose-limiting toxicity. Two types of adverse
taking 440 mg of Curcuma extract (36 mg of curcumin) daily,
events, both gastrointestinal, were possibly related to Curcuma
lymphocytic GST activity decreased gradually with time from a
consumption. One patient on 1320 mg of Curcuma extract daily
pretreatment GST value of 64 Ϯ 19 nmol/min/mg protein
Clinical Cancer Research 1897 Curcuma extract daily (containing 144 and 180 mg of curcumin)were between 144 and 519 nmol/g dried feces at the lower doseand between 64 and 1054 nmol/g dried feces at the higher dose. The feces of one of the patients on the highest dose contained aspecies which on HPLC analysis coeluted with curcumin sul-fate. Mass spectral investigation of the HPLC peak by selectedion monitoring afforded the molecular ion of m/z ϭ 447, and thefragmentation pattern was compatible with that of the authenticreference compound, corroborating the identity of the peak ascurcumin sulfate. Chemotherapeutic Efficacy of Oral Curcuma Extract.
All patients enrolled exhibited radiological evidence of progres-sive malignant disease before recruitment. Levels of the tumormarker CEA in venous blood were above the normal range in allpatients, and those of CA19.9 were abnormal in 80% of patients. In one patient, who received 440 mg of Curcuma extract (equiv-
Fig. 2 Leukocytic M G adduct levels for patients on Curcuma extract
alent to 36 mg of curcumin) daily, venous blood CEA levels
over a 5-week period. Each line represents one patient; each point is the
decreased from a pretreatment value of 310 Ϯ 15 to 175 Ϯ 9
mean of three to five readings from one sample taken before dose
g/liter after 2 months of treatment. This patient experienced
administration on each day (shown relative to first dose on day 1). Forexperimental details, see “Materials and Methods.” The interpatient
stabilization of disease in the colon but progression in the liver,
variation is significant (P Ͻ 0.001 by ANOVA), but there is no signif-
as demonstrated on CT scan. None of the other patients had
icant intrapatient change with time. The pooled SD, including all data
measurable disease in the colon because the primary tumor had
points, is 5.4 adducts/107 nucleotides.
been resected previously. Levels of CA19.9 did not change withtreatment. Five patients exhibited stable disease on CT scan[three (on 440, 880, and 1760 mg of Curcuma extract) for 3
(measured in triplicate at two time points for each patient) to
months and two (on 880 and 1320 mg of Curcuma extract) for
26 Ϯ 13 nmol/min/mg protein on day 29 of Curcuma consump-
4 months of treatment]. Significant changes in quality of life
tion (P Ͻ 0.001 by ANOVA; Fig. 1). This decline was not
observed at the higher dose levels. Retrospective subset analysisrevealed that pretreatment lymphocytic GST levels (53 Ϯ 10nmol/min/mg protein) in the five patients who subsequently
DISCUSSION
exhibited stable disease radiologically for more than 3 months
The study presented here constitutes the first clinical eval-
of treatment were lower (P ϭ 0.001 by ANOVA) than those in
uation of a standardized Curcuma extract in patients with cancer
the other 10 patients (84 Ϯ 25 nmol/min/mg protein). Leuko-
including pharmacodynamic and pharmacokinetic measure-
cytic M G levels varied considerably between patients, with no
ments. The results allow three conclusions, which will help to
significant difference between subsets of patients as defined by
optimize the design of future clinical trials of curcumin or
GST polymorphisms or radiological criteria. Consumption of
Curcuma extracts: (a) oral administration of Curcuma extract
Curcuma extract did not affect M G levels (Fig. 2).
for several months at doses of up to 2.2 g daily (equivalent to
Levels of Curcuminoids in Blood and Excreta.
180 mg of curcumin) appears safe in the framework of this
curcumin nor its metabolites curcumin glucuronide, curcumin
Phase I study; (b) the systemic bioavailability of p.o. adminis-
sulfate, hexahydrocurcumin, or hexahydrocurcuminol were
tered curcumin is low in humans; and (c) Curcuma extract may
found in the plasma or urine at up to 29 days of daily treatment.
cause clinical benefit in patients with advanced refractory colo-
Incubation of plasma and urine samples with glucuronidase andsulfatase enzymes, which would hydrolyze curcumin conju-
gates, did not generate measurable amounts of curcumin. To test
Our first conclusion regarding the apparent safety of Cur-
the hypothesis that curcumin, a very lipophilic molecule, is
cuma extracts is consistent with previous reports of clinical
sequestered in blood cells and/or total blood lipoproteins, which
studies of curcumin and turmeric. Soni and Kuttan (35) treated
may confound its detection in the plasma, these fractions were
10 volunteers with 500 mg of curcumin daily for 7 days and
also analyzed. Curcuminoids were not detected. Feces obtained
failed to observe clinical toxicity. Two clinical trials designed to
from patients on days 8 and 29 of consumption of Curcuma
study the efficacy of curcumin as an anti-inflammatory agent in
extract were investigated for the presence of curcuminoids.
the treatment of arthritis or postoperative inflammation found
HPLC analysis furnished a prominent peak in fecal samples
that daily doses of 1.2–2.1 g of curcumin for 2– 6 weeks did not
from all patients, which coeluted with curcumin. The mass
cause adverse effects (36, 37). In a pilot study published in
spectrum of this peak was characterized by the presence of the
abstract form (38), tablets of turmeric extract containing 99.8%
molecular ion (m/z ϭ 367) and major fragments of authentic
curcumin did not cause any treatment-related toxicity at doses as
curcumin including its base peak (m/z ϭ 149), confirming the
high as 8 g/day. Furthermore, a single dose of 50 –200 mg of
identity of this species as curcumin. Levels of curcumin in day
micronized curcumin formulated as capsules or sachets was
29 fecal samples from patients consuming 1760 and 2200 mg of
administered to 18 volunteers without causing significant tox-
1898 Study of Oral Curcuma in Patients with Colorectal Cancer
icity.4 Clinical trials of oral curcumin incorporating larger sub-
levels in patients with colorectal cancer. The lower levels shown
ject populations will be required to establish the safety of
in Fig. 2 are comparable with those reported previously in
chronic administration. Although certain communities in the
healthy volunteers, whereas the highest levels resemble those
Indian subcontinent consume up to 1.5 g of dietary turmeric per
seen in humans on pro-oxidant diets (45). M G adduct levels
person per day, curcumin constitutes only 2– 8% of most tur-
were unaffected by Curcuma consumption. It is conceivable that
meric preparations (39). The acceptable daily intake of curcu-
higher doses of curcumin, which furnish measurable plasma
min as an additive has been defined by the WHO as 0 –1 mg/kg
curcumin concentrations, are required to elicit an antilipid per-
body weight (40). Thus the largest dose administered in the
oxidative effect in the blood. Nevertheless, the intraindividual
study presented here (2.2 g of Curcuma extract, containing 180
reproducibility over time of M G adduct levels supports the
mg of curcumin) exceeds that of dietary consumption.
potential suitability of this adduct as a biomarker of the systemic
Our finding that curcumin was detectable only in the feces
effects of curcumin or other chemopreventive antioxidants. The
of patients and not in plasma, blood cells, or urine is in keeping
putative link between the GSTM1 null genotype and elevated
with the low systemic bioavailability of p.o. administered cur-
leukocytic M G adduct levels observed in the patients in this
cumin seen in rodents (9, 17, 19, 20) and suspected in humans
trial is congruous with associations reported previously between
(38).4 After a single oral dose of 2 g, curcumin levels were
GSTM1 genotype and levels of aflatoxin B -induced DNA ad-
transiently detectable in the serum of healthy volunteers (41). In
ducts (46) but is the first suggestion of such an association for
that study, coingestion of curcumin with the pepper constituent
an adduct formed by an endogenous product of lipid peroxida-
l-piperoylpiperidine, which is thought to inhibit xenobiotic glu-
curonidation, appeared to increase curcumin serum AUC by a
One-third of the patients in this study experienced stable
factor of 20. The presence of curcumin sulfate in the feces of
disease for 3 months or longer, and in one additional patient,
one patient at the highest dose level described here is consistent
Curcuma extract may have been linked to a decrease in venous
with the suspicion that curcumin can undergo metabolic conju-
tumor marker level and abatement of progression of the primary
gation in the gut (42). We are currently testing the hypothesis
colon tumor without a cytostatic effect on liver metastases. The
that sulfation is the major biotransformation route of the curcu-
possibility that patients with colorectal cancer may benefit from
min molecule catalyzed by intestinal tissue.
consumption of Curcuma extract merits evaluation at higher
Two potential biomarkers of the systemic efficacy of cur-
dose levels and ultimately within the framework of larger stud-
cumin were evaluated in the pilot study described here. Lym-
phocytic GST activity decreased with time in the three patients
In conclusion, despite the lack of reproducible effects of
who received the lowest dose level of Curcuma extract. This
Curcuma extracts on the biomarkers studied, this pilot study of
decrease may have been associated with the treatment, but in
Curcuma extract in patients with colorectal cancer provides
light of the small number of patients studied and the fact that
information that might help optimize the design of the future
GST activity was not decreased in patients on higher dose
clinical evaluation of curcumin. Doses of up to 2.2 g of Cur-
levels, the interpretation of this observation has to be tentative. cuma extract (containing 180 mg of curcumin) per day can be
Rats fed dietary curcumin at approximately 250 mg/kg body
administered to patients with cancer for up to 4 months, and in
weight and above were found to have decreased hepatic GST
this pilot study, such treatment was safe. Clinical trials of
activity compared to controls, and competitive enzyme inhibi-
Curcuma extracts as potential cancer chemopreventive agents
tion by the curcumin molecule was thought to be responsible
should focus on the effects of such doses in target tissues,
(7). It is unlikely that this observation can be used to rationalize
particularly colon epithelium. Moreover, because consumption
the decline observed in our patients because the dose used in the
of Curcuma extract was not detrimental to patients with ad-
rats was more than 60-fold higher than that given to the patients.
vanced cancer, future trials of Curcuma extracts as potential
Lymphocytic GST activity, as measured by the CDNB assay,
cancer chemotherapeutic agents should study the systemic ef-
has been shown to be independent of age and gender (43) and
fects of higher dose levels. Leukocytic GST activity and M G
constant within subjects, as borne out by measurements on at
levels merit further exploration as potentially suitable biomar-
least three occasions over a 2– 4-week period in normal indi-
kers of pharmacological efficacy in this regard.
viduals and those at increased risk of developing colorectalcancer (44). The observations made in the study reported here
ACKNOWLEDGMENTS
propose similar consistency for patients with advanced cancer.
We thank the following: the patients who participated in this study;
Whether or not lymphocytic GST activity correlates with colon
N. Rush, C. Sanganee, A. Alfirevic, and S. Feehan (Leicester and
mucosal GST levels in patients with colon cancer, as was
Liverpool Universities) for help with the patients’ samples; Drs. R.
demonstrated in individuals at risk of developing colon cancer
Singh, D. Jones, S. Plummer, M. Festing, M. Williams, and C. K. Lim
and Profs. D. Shuker and P. B. Farmer (MRC Toxicology Unit) for help
This study provides the first description of leukocytic M G
with experiments and useful discussions; Prof. D. Barnett and Dr. P. Woll for reviewing the case report forms; and Phytopharm plc., partic-ularly Drs. R. Grover and A. Kelly, for advice and provision of P54FPcapsules.
4 D. E. Brenner, I. Shureiqi, J. Bailey, D. Normolle, G. Kelloff,
REFERENCES
J. Crowell, C. Ireson, A. Gescher, C. L. Rock, and M. T. Ruffin. APhase I study of curcumin: bioavailability and safety profile for low
1. Kelloff, G. J., Crowell, J. A., Hawk, E. T., Steel, V. E., Lubet, R. A.,
Boone, C. W., Covey, J. M., Doody, L. A., Omenn, G. S., Greenwald,
Clinical Cancer Research 1899
P., Hong, W. K., Parkinson, D. R., Bagheri, D., Baxter, G. T., Blunden,
19. Holder, G. M., Plummer, J. L., and Ryan, A. J. The metabolism and
M., Doeltz, M. K., Eisenhauer, K. M., Johnson, K., Knapp, G. G.,
(1,7-bis-(4-hydroxy-3-methoxyphenyl)-1,6-
Longfellow, D. G., Malone, W. F., Nayfield, S. G., Seifried, H. E.,
heptadiene-3,5-dione) in the rat. Xenobiotica, 8: 761–768, 1978.
Swall, L. M., and Sigman, C. C. Strategy and planning for chemopre-
20. Wahlstrom, B., and Blennow, G. A study on the fate of curcumin in
ventive drug development: clinical development plans II. J. Cell. Bio-
the rat. Acta Pharmacol. Toxicol., 43: 86 –92, 1978.
21. Hayes, J. D., and Pulford, D. J. The glutathione S-transferase
2. Rao, C. V., Rivenson, A., Simi, B., and Reddy, B. S. Chemopreven-
supergene family: regulation of GST and contribution of the isoenzymes
tion of colon carcinogenesis by dietary curcumin, a naturally occurring
to cancer chemoprevention and drug resistance. Crit. Rev. Biochem.
plant phenolic compound. Cancer Res., 55: 259 –266, 1995.
Mol. Biol., 30: 445– 600, 1995.
3. Kawamori, T., Lubet, R., Steele, V. E., Kelloff, G. J., Kaskey, R. B.,
22. Mulder, T. P. J., Verspaget, H. W., Sier, C. F. M., Roelofs, H. M.,
Rao, C. V., and Reddy, B. S. Chemopreventative effect of curcumin, a
Ganesh, S., Griffioen, G., and Peters, W. H. Glutathione S-transferase
naturally occurring anti-inflammatory agent, during the promotion/pro-
in colorectal tumors is predictive for overall survival. Cancer Res., 55:
gression stages of colon cancer. Cancer Res., 59: 597– 601, 1999.
4. Mahmoud, N. N., Carothers, A. M., Grunberger, D., Bilinski, R. T.,
23. Tew, K. D. Gluathione-associated enzymes in anticancer drug re-
Churchill, M. R., Martucci, C., Newmark, H. L., and Bertagnolli, M. M.
sistance. Cancer Res., 54: 4313– 4320, 1994.
Plant phenolics decrease intestinal tumors in an animal model of familial
24. Marnett, L. J. Lipid peroxidation: DNA damage by malondialde-
adenomatous polyposis. Carcinogenesis (Lond.), 21: 921–927, 2000.
hyde. Mutat. Res., 424: 83–95, 1999.
5. Kuttan, R., Sudheeran, P. C., and Josph, C. D. Turmeric and curcu-
25. Diczfalusy, U., Falardeau, P., and Hammarstrom, S. Conversion of
min as topical agents in cancer therapy. Tumori, 73: 29 –31, 1987.
prostaglandin endoperoxides to C17-hydroxy acids catalyzed by human
6. Greenlee, R. T., Murray, R., Bolden, S., and Wingo, P. A. Cancer
platelet thromboxane synthase. FEBS Lett., 84: 271–274, 1977.
statistics, 2000. CA Cancer J. Clin., 50: 7–33, 2000.
26. Taketo, M. M. Cyclooxygenase-2 inhibitors in tumorigenesis (part
7. Piper, J. T., Singhal, S. S., Salameh, M., Torman, R. T., Awasthi,
II). J. Natl. Cancer Inst. (Bethesda), 90: 1609 –1620, 1998.
Y. C., and Awasthi, S. Mechanisms of anticarcinogenic properties of
27. Hendrickse, C. W., Kelly, R. W., Radley, S., Donovan, I. A.,
curcumin: the effect of curcumin on glutathione linked detoxification
Keighley, M. R. B., and Neoptolemos, J. P. Lipid peroxidation and
enzymes in rat liver. Int. J. Biochem. Cell. Biol., 30: 445– 456, 1998.
prostaglandins in colorectal cancer. Br. J. Surg., 81: 1219 –1223, 1994.
8. Susan, M., and Rao, M. N. A. Induction of glutathione S-transferase
28. Venkatesan, P., and Rao, M. N. A. Structure-activity relationships
activity by curcumin in mice. Arzneim. Forsch., 42: 962–964, 1992.
for the inhibition of lipid peroxidation and the scavenging of freeradicals by synthetic symmetrical curcumin analogues. J. Pharm. Phar-
9. Sharma, R. A., Ireson, C. R., Verschoyle, R. D., Hill, K. A., Wil-
macol., 52: 1123–1128, 2000.
liams, M. L., Leuratti, C., Manson, M. M., Marnett, L. J., Steward,
29. Aaronson, N. K., Ahmedzai, S., Bergman, B., Bullinger, M., Cull,
W. P., and Gescher, A. Effects of dietary curcumin on glutathione
A., Duez, N. J., Filiberti, A., Flechtner, H., Fleishman, S. B., and de
S-transferase and malondialdehyde-DNA adducts in rat liver and colon
Haes, J. C. The European Organization for Research and Treatment of
mucosa: relationship with drug levels. Clin. Cancer Res., 7: 1542–1548,
Cancer QLQ-C30: a quality of life instrument for use in international
clinical trials in oncology. J. Natl. Cancer Inst. (Bethesda), 85: 365–376,
10. Subramanian, M., Sreejayan, M., Rao, M. N., Devasagayam, T. P.,
and Singh, B. B. Diminution of singlet oxygen induced DNA damage by
30. Habig, W. H., Pabst, M. J., and Jakoby W.B. Glutathione S-
curcumin and related antioxidants. Mutat. Res., 311: 249 –255, 1994.
transferases. J. Biol. Chem., 249: 7130 –7139, 1974.
11. Tonnesen, H. H., and Greenhill, J. V. Studies on curcumin and
31. DeSousa, M., Pirmohamed, M., Kitteringham, N. R., Woolf, T., and
curcuminoids. XXII. Curcumin as a reducing agent and as a radical
Park, B. K. No association between tacrine transaminitis and the gluta-
scavenger. Int. J. Pharm. (Amst.), 87: 79 – 87, 1992.
thione transferase genotype in patients with Alzheimer’s disease.
12. Kunchandy, E., and Rao, M. N. A. Oxygen radical scavenging
Pharmacogenetics, 8: 353–355, 1998.
activity of curcumin. Int. J. Pharm. (Amst.), 58: 237–240, 1990.
32. Harries, L. W., Stubbins, M. J., Forman, D., Howard, G. C., and
13. Reddy, A. C. H. P., and Lokesh, B. R. Studies on the inhibitory
Wolf, C. R. Identification of genetic polymorphisms at the glutathioneS-transferase locus and association with susceptibility to bladder,
effects of curcumin and eugenol on the formation of reactive oxygen
testicular and prostate cancer. Carcinogenesis (Lond.), 18: 641– 644,
species and the oxidation of ferrous iron. Mol. Cell. Biochem., 137:
33. Sevilla, C. L., Mahle, N. H., Eliezer, N., Uzieblo, A., O’Hara, S. M.,
14. Donatus, I. A., Sardjoko, X. X., and Vermeulen, N. P. E. Cytotoxic
Nokubo, M., Miller, R., Rouzer, C. A., and Marnett, L. J. Development
and cytoprotective activities of curcumin. Biochem. Pharmacol., 39:
of monoclonal antibodies to the malondialdehyde-deoxyguanosine ad-
duct, pyrimidopurinone. Chem. Res. Toxicol., 10: 172–180, 1997.
15. Mukhopadhary, A., Basu, N., Ghatak, N., and Gujral, P. K. Anti-
34. Leuratti, C., Singh, R., Lagneau, C., Farmer, P. B., Marnett, L. J.,
inflammatory and irritant activities of curcumin analogues in rats.
and Shuker, D. E. G. Determination of malondialdehyde-induced DNA
Agents Actions, 12: 508 –515, 1982.
damage in human tissues using an immunoslot blot assay. Carcinogen-
16. Sharma, S. C., Mukhtar, H., Sharma, S. K., and Krishna Murt, C. R.
esis (Lond.), 19: 1919 –1924, 1998.
Lipid peroxide formation in experimental inflammation. Biochem. Phar-
35. Soni, K. B., and Kuttan, R. Effect of oral curcumin administration
macol., 21: 1210 –1214, 1972.
on serum peroxides and cholesterol levels in human volunteers. Indian
17. Ireson, C. R., Orr, S., Jones, D. L., Verschoyle, R., Lim, C. K., Luo,
J. Physiol. Pharmacol., 36: 273–275, 1992.
J. L., Howells, L., Plummer, S. M., Jukes, R., Williams, M., Steward,
36. Deodhar, S. D., Sethi, R., and Srimal, R. C. Preliminary study on
W. P., and Gescher, A. Characterization of metabolites of the chemo-
antirheumatic activity of curcumin (diferuloyl methane). Indian J. Med.
preventive agent curcumin in humans and rat hepatocytes and in rat
plasma and evaluation of their ability to inhibit cyclooxygenase-2 ex-
37. Satoskar, R. R., Shah, S. J., and Shenoy, S. G. Evaluation of
pression. Cancer Res., 61: 1058 –1064, 2001.
anti-inflammatory property of curcumin (diferuloyl methane) in patients
18. Plummer, S. M., Holloway, K. A., Manson, M. M., Munks, R. J.,
with post-operative inflammation. Int. J. Clin. Pharmacol. Ther. Toxi-
Kaptein, A., Farrow, S., and Howells, L. Inhibition of cyclo-oxygenase
2 expression in colon cells by the chemopreventive agent curcumin
38. Cheng, A. L., Lin, J. K., Hsu, M. M., Shen, T. S., Ko, J. Y., Lin,
involves inhibition of NF-B activation via the NIK/IKK signalling
J. T., Wu, M. S., Yu, H. S., Jee, S. H., Chen, G. S., Chen, T. M., Chen,
complex. Oncogene, 18: 6013– 6020, 1999.
C. A., Lai, M. K., Pu, Y. S., Pan, M. H., Wang, U. J., Tsai, C. C., and
1900 Study of Oral Curcuma in Patients with Colorectal Cancer
Hsieh, C. Y. Phase I chemoprevention clinical trial of curcumin. Proc.
43. van Lieshout, E. M. M., and Peters, W. H. M. Age and gender
Am. Soc. Clin. Oncol., 17: 558a, 1998.
dependent levels of glutathione and glutathione S-transferases in human
39. Sambaiah, K., Ratankumar, S., Kamanna, V. S., Satyanarayana,
lymphocytes. Carcinogenesis (Lond.), 19: 1873–1875, 1998.
M. N., and Rao, M. V. L. Influence of turmeric and curcumin on growth,
44. Szarka, C. E., Pfeiffer, G. R., Hum, S. T., Everley, L. C., Balshem,
blood constituents and serum enzymes in rats. J. Food Sci. Technol., 19:
A. M., Moore, D. F., Litwin, S., Goosenberg, E. B., Frucht, H., and
Engstrom, P. F. Glutathione S-transferase activity and glutathione S-transferase expression in subjects at risk for colorectal cancer. Cancer
40. Evaluation of Certain Food Additives: 51st Report of the Joint
Res., 55: 2789 –2793, 1995.
FAO/WHO Expert Committee on Food Additives, WHO Technical
45. Fang, J. L., Vaca, C. E., Valsta, L. M., and Mutanen, M. Determi-
Report Series 891. Geneva: WHO, 2000.
nation of DNA adducts of malondialdehyde in humans: effects of
41. Shoba, G., Joy, D., Joseph, T., Majeed, M., Rajendran, R., and Srini-
dietary fatty acid composition. Carcinogenesis (Lond.), 17: 1035–1040,
vas, P. S. S. R. Influence of piperine on the pharmacokinetics of curcumin
in animals and human volunteers. Planta Med., 64: 353–356, 1998.
46. Liu, Y. H., Taylor, J., Linko, P., Lucier, G. W., and Thompson,
42. Ravrindanath, V., and Chandrasekhara, N. In vitro studies on the
C. L. Gluathione S-transferase mu in human lymphocyte and liver: role
intestinal absorption of curcumin in rats. Toxicology, 20: 251–257,
in modulating formation of carcinogen-derived DNA adducts. Carcino-
genesis (Lond.), 12: 2269 –2275, 1991.
Poster Presentations (as of September 27) Presenting authors are requested to stay at their posters during the following hours. odd numbers : October 12(Tue), 17:30-18:30; October 13(Wed), 18:30-19:30 even numbers : October 12(Tue), 18:30-19:30; October 13(Wed), 17:30-18:30 P1 Text Mining P1-1 Apply of Textmining Method to Study the Roles in Improving the Health by Lactoferrin, a Mul
Health Information and History Patient’s Name : _______________________________________________________ Date of Birth : ______________ If You are Completing This form For Another Person: Your Name:________________________________________ Phone:________________ Relationship:__________________ Emergency Contact :(If Not Listed Above) Name:____________________________________________ P

 1896 Study of Oral Curcuma in Patients with Colorectal Cancer
1896 Study of Oral Curcuma in Patients with Colorectal Cancer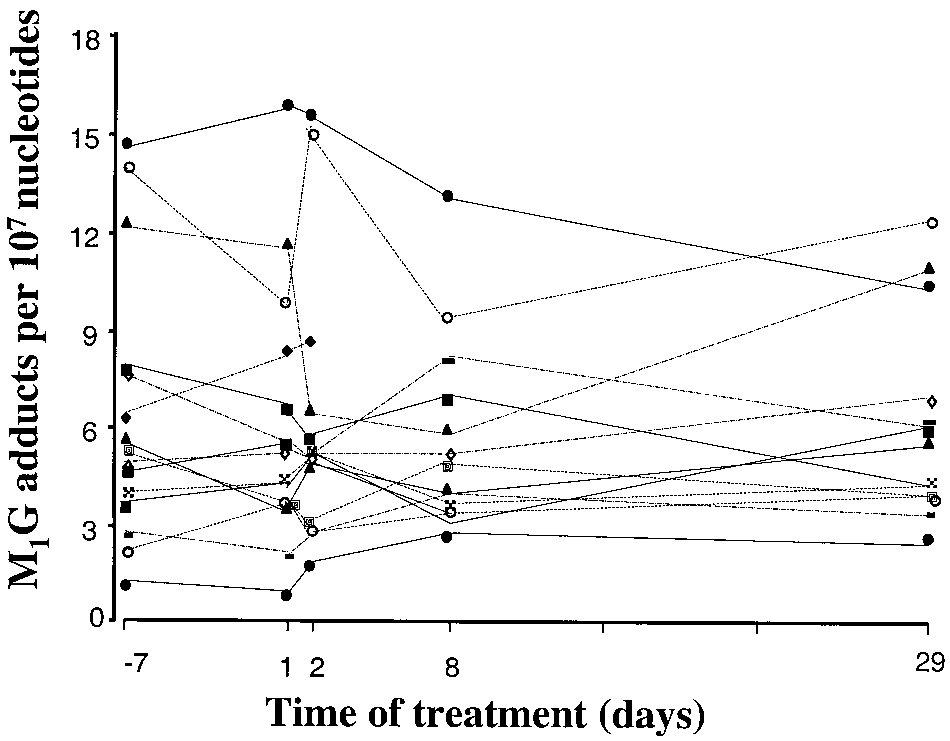 Clinical Cancer Research 1897
Clinical Cancer Research 1897