La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Unbekannt
Cancer Chemother Pharmacol (2004) 53: 220–224DOI 10.1007/s00280-003-0716-7
Eduardo Lasalvia-Prisco Æ Silvia CucchiJesu´s Va´zquez Æ Eduardo Lasalvia-GalanteWilson Golomar Æ William Gordon
Insulin-induced enhancement of antitumoral responseto methotrexate in breast cancer patients
Received: 31 March 2003 / Accepted: 29 August 2003 / Published online: 4 December 2003Ó Springer-Verlag 2003
Abstract Purpose: It has been reported that insulin in-
tumor in the three groups were compared statistically.
creases the cytotoxic effect in vitro of methotrexate by as
Results: Under the trial conditions, the methotrexate-
much as 10,000-fold. The purpose of this study was to
treated group and the insulin-treated group responded
explore the clinical value of insulin as a potentiator of
most frequently with progressive disease. The group
methotrexate. Patients and methods: Included in this
treated with insulin + methotrexate responded most
prospective, randomized clinical trial were 30 women
frequently with stable disease. The median increase in
with metastatic breast cancer resistant to fluorouracil +
tumor size was significantly lower with insulin +
Adriamycin + cyclophosphamide and also resistant to
methotrexate than with each drug used separately.
hormone therapy with measurable lesions. Three groups
Discussion: Our results confirmed in vivo the results of
each of ten patients received two 21-day courses of the
previous in vitro studies showing clinical evidence that
following treatments: insulin + methotrexate, metho-
insulin potentiates methotrexate under conditions where
trexate, and insulin, respectively. In each patient, the size
insulin alone does not promote an increase in tumor
of the target tumor was measured before and after
treatment according to the Response Evaluation Criteria
activity must have been enhanced by the biochemical
In Solid Tumors. The changes in the size of the target
events elicited in tumor cells by insulin. Conclusions: Inmultidrug-resistant metastatic breast cancer, metho-trexate + insulin produced a significant antitumoralresponse that was not seen with either methotrexate or
Department of Medicine, School of Medicine,University of Uruguay, Montevideo, Uruguay
Keywords Breast Cancer Æ Chemotherapy Æ Insulin Æ
S. Cucchi Æ J. Va´zquez Æ E. Lasalvia-Galante Æ W. Golomar
E. Lasalvia-PriscoInterdoctors Medical Center,Montevideo, Uruguay
E. Lasalvia-Prisco Æ J. Va´zquez Æ E. Lasalvia-GalanteW. GolomarNational Cancer Institute,
It is known that slowly growing cancers have tumor cell
populations with a low-growth fraction and are less
sensitive to chemotherapy than rapidly growing tumors
with high-growth fractions [11]. Slowly growing malig-
nancies have relatively more cells in a noncycling status
and fewer cells in a cycling status than rapidly growing
(Former Director of the Department of Medicine,
malignancies. It has been demonstrated that insulin as a
School of Medicine, University of Uruguay,
pharmacological agent induces the switch from a non-
Montevideo, Uruguay and National Cancer Institute,
cycling to a cycling status in tumor cells [5]. In MCF-7
Montevideo, Uruguay),Research & Development Department,
human breast cancer cells, insulin has been shown to
increase the cytotoxic effect of methotrexate up to
10,000-fold in vitro [1]. Ellipticine uptake is also
increased by insulin [9]. It has been suggested that
E-mail: research@pharmablood.comTel.: +1-305-9442544
insulin is effective in potentiating most chemotherapy
drugs. This insulin-induced potentiation has been
proposed as a strategy for breast cancer treatment, but
confirmed the committeeÕs criteria because no significant differences
confirmatory clinical trials are still lacking [2]. This
were found in tumor growth either between the insulin-alone groupand the methotrexate-alone group or between before and after
study was carried out to confirm insulin-induced clinical
treatment in the insulin-alone group.
potentiation of the antitumoral effect of methotrexate assuggested by preclinical studies and to establish amechanism of action for this antitumoral effect.
All the patients included in the study received two 21-day courses
of treatment separated by a 7-day interval without treatment be-tween courses. In group 1, the treatment course was intravenoushuman recombinant insulin (0.3 U/kg body weight every other
day) followed 20 min later by a 15-min intravenous infusion ofmethotrexate (2.5 mg/m2 in 50 ml 30% glucose). If symptomatic
The study was conducted in 30 patients with breast cancer admitted
hypoglycemia was observed, the 30% glucose solution containing
to medical centers that reported medical data to the Cooperative
methotrexate was infused immediately. An oral glucose supplement
Trials Center (CTC) of PharmaBlood, R&D Department, Florida.
was also prescribed to prevent delayed hypoglycemic symptoms. In
A prospective, randomized trial was carried out. All patients met
group 2, insulin was omitted and methotrexate was administered
the following eligibility criteria: histologically confirmed breast
intravenously at the same dose and in the same solution (2.5 mg/m2
carcinoma, metastatic stage (M1); Eastern Cooperative Oncology
in 50 ml 30% glucose) as in group 1. In group 3, methotrexate was
Group (ECOG) performance status (PS) £ 2; age £ 74 years; and
omitted, insulin was administered at the same dose as in group 1,
adequate hematological function (WBC count ‡4000/ll, neutrophil
and 30% glucose solution was also administered intravenously
‡2000/ll, hemoglobin level ‡9.0 g/dl, platelet count
20 min after insulin or sooner if hypoglycemic symptoms were
‡10·104/ll), renal function (serum creatinine £ 1.5 mg/dl, 24-h
creatinine clearance £ 60 ml/min), liver function (total bilirubin£ 2.0 mg/dl, serum transaminases not more than twice the upperlimit of the normal range), and respiratory function (PaO2‡60 Torr). The patients included had measurable lesions, as
required by the Response Evaluation Criteria In Solid Tumors(RECIST) system of tumor assessment [13], and if they had a
After 8 weeks (two 3-week courses plus 1 week interval after each
positive estrogen receptor status, they had been treated with and
course), the response to treatment was assessed in each patient
become resistant to hormone therapy.
using RECIST criteria [13]. The sum of the longest diameter of
All patients included in the study had progressive disease
measurable target lesions and the number of non-target lesions
(RECIST criteria) after chemotherapy with at least four series of
were recorded immediately before and after this 8-week period.
fluorouracil + Adriamycin + cyclophosphamide (FAC) and had
Skin nodules and palpable lymph nodes were measured using
not been treated with any other chemotherapy. They were ran-
calipers. Lung and liver target lesions were measured by a CAT
domly allocated to three groups of ten patients each: group 1 was
scan. Responses were confirmed by repeating the assessment
treated with insulin + methotrexate as described below, group 2
4 weeks after status assignment. Three independent reviewers per-
was treated with methotrexate without insulin, and group 3 was
formed all image measures (Telemedical Organization, North
treated with insulin without methotrexate. Written informed con-
sent, including detailed information about risks and benefits, was
The distribution of RECIST status (progressive disease, stable
approved and signed by all the patients included in the study.
disease, or remission) in each group was recorded. This distribution
Central computerized remote randomization was performed, with
was dependent on treatments that showed statistical significance
patients being allocated to one of the groups through random se-
according to the Chi-squared test. The data from the RECIST
quence generation by the permuted block method. An assessment
measurements of the change in tumor size of the patients in each
of the results after 30 patients had completed the trial showed that
treatment group, expressed as a percentage of pretreatment
this sample size was enough. The patients were recruited from two
measurements, were compared using StudentÕs t-test. Additionally,
oncological medical centers in Montevideo, Uruguay (first at the
increases in tumor size were expressed as a proportion of the initial
National Cancer Institute and then at Interdoctors Medical Cen-
value and analyzed by the two-proportion test comparing pairs of
ter), both of which participated with their data in the network
groups: group 3 vs group 1, and group 2 vs group 1. The sample
operated and sponsored by the Cooperative Trials Center (CTC) of
size was assessed after analysis of the results when the trial was
finished for the 30 patients allocated to the three groups. The above
The institutional ethics committee of PharmaBlood and the
pairs of groups were analyzed for the proportion of progressive
institutional review boards of the participating medical centers
disease in each. Ten patients in each group was the required sample
approved the trial. The ethical reviewers considered that an 8-week
size for an 80% chance of rejecting the hypothesis of equal pro-
delay before starting second-line chemotherapy after FAC had
portions at the 0.05 level of significance when the true proportions
failed in all the patients included in the trial was acceptable. This
were those shown by the study. Statistical analysis was performed
determination was consistent with the standard of care in this
using StatsDirect software and an independent expert was con-
clinical situation which has been recently well summarized [3]:
Despite almost 30 years of clinical cancer research, the trueimpact of second and subsequent lines of chemotherapy on theoutcome of metastatic breast cancer patients, especially on the
duration of survival, is still unknown. In the virtually incurablemetastatic setting, issues like quality of life and patientsÕ pref-
The characteristics of the patients included are shown in
Table 1. The three groups were comparable in the most
The accepted protocol was resubmitted to the committee for
relevant prognostic parameters for the clinical condition
review in order to obtain approval for treatment of patients with
studied. Previous treatments were also comparable. The
insulin alone considering the potentially harmful effect through the
similar range of sizes of target lesions measured before
activation of receptors for insulin/insulin-like growth factors. Thecommittee confirmed the approval on the basis of reports of no
treatment was especially significant, allowing the change
harmful effect of this treatment [6, 7]. The results of the study
in size to be measured as a percentage of initial size.
Table 1 Clinical characteristicsof the 30 women with
Fig. 1 Post-treatment RECIST status of measurable target lesions. After the respective treatment, the change in the measurable lesions
Fig. 2 Increase in size of measurable target lesions (RECIST
selected as targets in each patient was evaluated and the status of
assessment). After each treatment, the change in the measurable
therapeutic response, defined in terms of the RECIST criteria, was
lesions selected as targets in each patient was evaluated in terms of
recorded. Under the conditions of this study, two response statuses
the RECIST criteria and expressed as a percentage of the measured
were recorded: stable disease (less than 20% increase or less than
pretreatment size. For each treatment group, the mean±SD and
30% decrease in the sum of largest diameters of targets) and
95% CI for the values of this response were calculated: group 1
progressive disease (more than 20% increase in the sum of
(insulin + methotrexate) 13.51±3.01% (95% CI 11.35–15.67%);
diameters). Stable disease, the best response obtained, was more
group 2 (methotrexate) 20.21±2.27% (95% CI 18.58–21.84%);
frequent in the group treated with insulin + methotrexate (nine of
group 3 (insulin) 21.04±2.17% (95% CI 19.49–22.59%). The
ten) than in methotrexate-treated group (three of ten) or insulin-
increase in size of lesions in group 1 (insulin + methotrexate) was
treated group (two of ten). The distribution of RECIST type
significantly lower (StudentÕs t-test) than the increase in size in
responses (stable disease or progressive disease) was dependent on
the treatments tested and statistically significant (P<0.01, Chi-
(P<0.001). Group 2 showed no significant difference from group
Figure 1 shows the RECIST status assessed under the
insulin + methotrexate than in those treated with
study conditions. Progressive disease was the most fre-
insulin alone and significantly lower than in those trea-
quent response in two of the three groups: in group 2
(treated with methotrexate alone) there were seven
From the same set of measurements, Figs. 1 and 2
progressive disease and three stable disease, and in
show the clinical and biological effects of the treatments,
group 3 (treated with insulin alone) there were eight
respectively. Figure 1 indicates that the decrease in tu-
progressive disease and two stable disease. In group 1
mor growth induced by insulin + methotrexate reached
(treated with insulin + methotrexate), stable disease was
the level of a clinically confirmed antitumoral response
the most frequent response (nine stable disease, one
because more patients in this group achieved stable
progressive disease). The distribution of RECIST type
disease. Figure 2 shows that insulin + methotrexate
responses (stable disease and progressive disease) was
treatment reduced tumor growth. All patients completed
dependent on the treatments tested, and was statistically
the study. Hypoglycemia was induced in all patients
significant (P<0.01, Chi-squared test).
receiving insulin as part of their protocol. Eight patients
Figure 2 shows the means and 95% confidence
in group 1 and nine patients in group 3 showed no
intervals (CI) of the percentage increase in tumor size
hypoglycemic symptoms during the 20 min after insulin
after treatment in the three groups. Increases in tumor
injection; they showed a mean blood glucose level of
size were significantly lower in patients treated with
456 mg/dl (range 376–520 mg/dl). Two patients in group
Table 2 Maximum recorded WHO toxicity grade in the patients
used here as a description of the clinical effect of a
included in the trial comparing insulin + methotrexate (group 1),
reduction in the proportion of patients showing pro-
methotrexate (group 2) and insulin (group 3). The numbers of
patients with each toxicity grade (0 to 4) in the three groups areshown. No other toxicities referred to in the WHO criteria were
Therefore, as reported previously, our results support
the hypothesis that insulin can potentiate the antitu-moral effect of methotrexate [2] and confirm in vivo
previously reported in vitro results [10]. Our results also
show insulin potentiation of methotrexate in this con-dition, where insulin alone did not promote an increase
in tumor growth (group 3). This effect is in agreement
with previous results from in vitro models where insulin
enhancement of cytotoxicity was not a direct conse-
quence of an insulin-dependent increase in the growth
rate of tumor cells [1, 10]. The same in vitro models do
not allow an explanation of the insulin potentiation of
methotrexate in terms of the known effects of insulintreatment upon the specific metabolism of methotrexate
which include a decrease in intracellular pH induced by
glucose metabolism and tight binding of the drug to its
target, dihydrofolate reductase. Insulin potentiation of
other antitumoral drugs has been reported [9].
If we discount the promotion of tumor cell growth
and the interaction with the specific target as the
mechanism of potentiation of methotrexate by insulin,we can hypothesize that this mechanism could involveanother general insulin-dependent biochemical pathway
1 and one patient in group 3 showed hypoglycemic
as has been previously suggested to explain the in vitro
symptoms within 20 min of insulin injection (13, 16 and
potentiation of methotrexate by insulin [1]: protein
19 min), but recovered immediately after starting the
synthesis in tumor cells is one of the biochemical path-
glucose infusion. There was no evidence of any harmful
ways activated by insulin [8]. Most chemotherapy drugs
sequelae attributable to the hypoglycemia induced.
that have been tested using insulin to increase cytotox-
Table 2 shows the toxicities associated with antitu-
icity are known modifiers of protein structure that act at
moral chemotherapy (according to WHO criteria)
the genetic or epigenetic level [12]. High levels of mu-
tated or epigenetically modified proteins could beresponsible for the cytotoxic mechanism elicited by theinsulin-dependent increase in protein synthesis associ-
ated with chemotherapy drugs. The relative selectivity ofthis mechanism of action for insulin + methotrexate in
The methotrexate dose used in this study was chosen
malignant cells is attributed to the agonism of insulin
because a similar dose of methotrexate had been used
and insulin-like receptors in tumor cells. Certainly, the
previously in patients receiving low-dose combined
response to insulin is more intense in most tested cancer
chemotherapy potentiated with insulin [2]. In addition,
cells than in most normal cells. This is probably because
the cumulative monthly dose was no higher than the
cancer cells are richer in receptors for insulin-like growth
monthly dose used in the well-known standard protocol
factors that are cross-stimulated by insulin [4].
of methotrexate + fluorouracil + cyclophosphamide(CMF). Indeed, each individual methotrexate injection(2.5 mg/m2) was less than the dose usually considered
optimal in non-potentiated protocols but is within thepresumed range of effective dose for a potentiation
The in vitro potentiation of methotrexate cytotoxicity by
similar to the one observed in vitro. The results of this
insulin in human breast cancer cell lines was previously
study confirmed the expected safety of the selected
known. We report the results of a randomized, con-
methotrexate dose. The toxicities in the methotrexate-
trolled trial that confirmed, at the clinical level, the
alone group were not relevant (WHO grades 1/2) and
potentiation by insulin of the antitumoral effect of
they were even lower when methotrexate was associated
methotrexate in women with advanced breast cancer.
with insulin, only producing a grade 1 mucositis. In this
The term antitumoral is used as a description of the
study, methotrexate at this safe low dose did not have an
clinical effect of a reduction in the proportion of patients
antitumoral effect when used alone (group 2), but it did
with progressive disease. Under the conditions of this
produce a significant antitumoral effect when adminis-
study, the dose of insulin used did not increase tumor
tered after insulin (group 1). The term antitumoral is
growth. Therefore, we suggest that, as has been reported
in vitro, methotrexate potentiation by insulin was not a
5. Gross GE, Boldt DH, Osborne CK (1984) Perturbation by
direct consequence of the expansion of the tumor cycling
insulin of human breast cancer cell kinetics. Cancer Res44:3570–3575
cell population but a consequence of some of the bio-
6. Kath R, Schiel R, Muller UA, Hoffken K (2000) Malignancies
chemical events that are simultaneously activated. The
in patients with insulin-treated diabetes mellitus. J Cancer Res
enhancement of methotrexate uptake by tumor cells
and/or the promotion of protein synthesis in a muta-
7. Mink PJ, Shahar E, Rosamond WD, Alberg AJ, Folsom AR
genic intracellular environment are hypothesized to be
(2002) Serum insulin and glucose levels and breast cancerincidence: the atherosclerosis risk in communities study. Am
mechanisms of potentiation. It is known that both
events are promoted by insulin acting as a cross-agonist
8. Osborne CK, Bolan G, Monaco ME, Lippman ME (1976)
of the highly expressed receptors for insulin-like growth
Hormone responsive human breast cancer in long-term tissue
culture: effect of insulin. Proc Natl Acad Sci U S A 73:4536–4540
These mechanisms, which are shared with other pri-
9. Oster JB, Creasey WA (1981) Enhancement of cellular uptake
mary tumor cells and with other chemotherapeutic
of ellipticine by insulin preincubation. Eur J Cancer Clin Oncol
agents suggest that it would be worthwhile to pursue
further study of these phenomena in other tumors and
10. Schilsky RL, Bailey BD, Chabner BA (1981) Characteristics of
membrane transport of methotrexate by cultured human breast
cancer cells. Biochem Pharmacol 30:1537–1542
11. Shackney SE, McCormack GW, Cocheral GJ (1978) Growth
rate patterns of solid tumors and their relation to responsive-
ness to therapy. Ann Intern Med 89:107–121
12. Silva JM, Garcia JM, Dominguez G, Silva J, Rodriguez R,
Portero JL, Corbacho C, Provencio M, Espana P, Bonilla F
1. Alabaster A, Vonderhaar B, Shafie S (1981) Metabolic modi-
Silva JM, Garcia JM, Dominguez G, et al (2000) DNA
fication by insulin enhances methotrexate cytotoxicity in
damage after chemotherapy correlates with tumor response
MCF-7 human breast cancer cells. Eur J Cancer Clin Oncol
and survival in small cell lung cancer patients. Mutat Res
2. Ayre SG, Perez Garcia y Bellon D, Perez Garcia D Jr (1990)
13. Therasse P, Arbuck SG, Eisenhauer EA, Wanders J, Kaplan
Neoadjuvant low-dose chemotherapy with Insulin in breast
RS, Rubinstein L, Verweij J, Van Glabbeke M, van
Oosterom AT, Christian MC, Gwyther SG (2000) New
3. Cardoso F, Di LA, Lohrisch C, Bernard C, Ferreira F, Piccart
guidelines to evaluate the response to treatment in solid tu-
M (2002) Second and subsequent lines of chemotherapy for
mors. European Organization for Research and Treatment of
metastatic breast cancer: what did we learn in the last two
Cancer, National Cancer Institute of the United States,
National Cancer Institute of Canada. J Natl Cancer Inst
4. Cullen KJ, Yee D, Sly WS, Perdue J, Hampton B, Lippman
ME, Rosen N (1990) Insulin-like growth factor receptorexpression and function in human breast cancer. Cancer Res50:48–53
ANALGESIA E SEDAÇÃO EM TERAPIA INTENSIVA: RECOMENDAÇÕES GERAIS ANALGESIA AND SEDATION IN INTENSIVE CARE: GENERAL RECOMMENDATIONS ANALGESIA Y SEDACÍON EN TERAPIA INTENSIVA: RECOMENDACIONES GENERALES RESUMO Trata-se de estudo descritivo e exploratório sobre analgesia e sedação em terapia intensiva. Os objetivos do presente estudo foram conceituar e caracterizar a intensidade dolor
Introduction : présentation de NanoSMS (Jérémie Léonard, IPCMS) Surfaces fonctionalisées et nanostructurées pour applications biomédicales : Nadia Jessel, UMR 595, Faculté de Chirurgie Dentaire: « Nanostructured and Multilayered Active Materials for Clinical Applications” Lydie Ploux, ICSI, Mulhouse : « Adhésion de cellules osseuses humaines et de bactéries sur des surfac
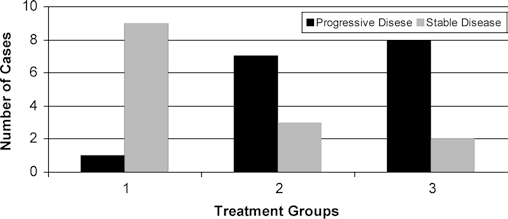
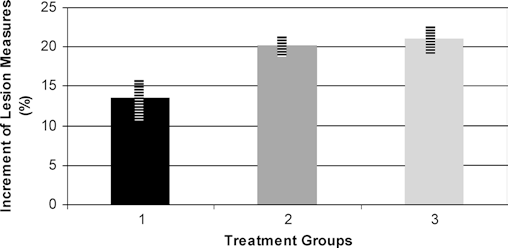 Table 1 Clinical characteristicsof the 30 women with
Fig. 1 Post-treatment RECIST status of measurable target lesions.
Table 1 Clinical characteristicsof the 30 women with
Fig. 1 Post-treatment RECIST status of measurable target lesions.