La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Jcp325927.qxd
Baseline Values and Sotalol-Induced Changes of Ventricular Repolarization Duration, Heterogeneity, and Instability in Patients With a History of Drug-Induced Torsades de Pointes
Jean-Philippe Couderc, Stefan Kaab, Martin Hinterseer, Scott McNitt, Xiaojuan Xia, Anthony Fossa, Britt M.
Beckmann, Slava Polonsky and Wojciech Zareba
2009; 49; 6 originally published online Oct 28, 2008;
The online version of this article can be found at:
http://www.jclinpharm.org/cgi/content/abstract/49/1/6
Additional services and information for can be found at: The Journal of Clinical Pharmacology CLINICAL STUDIES Baseline Values and Sotalol-Induced Changes of Ventricular Repolarization Duration, Heterogeneity, and Instability in Patients With a History of Drug-Induced Torsades de Pointes Jean-Philippe Couderc, PhD, MBA, Stefan Kaab, MD, PhD, Martin Hinterseer, MD,Scott McNitt, MS, Xiaojuan Xia, MS, Anthony Fossa, PhD, Britt M. Beckmann, MD,Slava Polonsky, MS, and Wojciech Zareba, MD, PhD, FACCThe authors investigated whether computerized parame-patients with a history of Torsades de Pointes had a longerters quantifying ventricular repolarization delay, hetero-QTc and an increased repolarization heterogeneity ofgeneity, and instability characterize individuals who: 44 ± 13 vs 35 ± 8 ms,developed drug-induced Torsades de Pointes. Assessing
P = .02). On sotalol, the electrocardiograms from individ-an individual’s propensity to Torsades de Pointes whenuals with Torsades de Pointes revealed a delay of the ter-exposed to a QT-prolonging drug is challenging becauseminal part of the T wave that was not present in patientsbaseline QT prolongation has limited predictive value.without Torsades de Pointes (TpTe: 27 ± 40 vs –2 ± 21 ms,Five-minute digital 12-lead electrocardiograms were: 20 ± 29 vs 2 ± 4 ms, P = .04). Results sug-acquired at baseline and after a sotalol challenge in 16gest that the electrocardiogram abnormalities characteriz-patients who had a history of Torsades de Pointes in theing patients with a history of Torsades de Pointes are (1)context of a QT-prolonging drug and 17 patients who didan increased repolarization heterogeneity at baseline andnot have such history. Computerized measurements of QTc,(2) a sotalol-induced prolongation of the terminal part ofT peak to T end intervals (TpTe), TpTe/QTc, and QT vari-ability were implemented, and novel quantifiers of ventric-ular repolarization heterogeneity from the early (ERD) andKeywords: QT interval; Torsades de Pointes; electrocar- late (LRD) part of the T wave were investigated. Comparedwith electrocardiograms of patients without a history ofJournal of Clinical Pharmacology, 2009;49:6-16 Torsades de Pointes, the baseline electrocardiograms of2009 the American College of Clinical Pharmacology
From the Heart Research Follow-Up Program, Cardiology Department,University of Rochester Medical Center, Rochester, New York (Dr Couderc, Mr
Drug-induced Torsades de Pointes (TdP) have been
associated with an increasing number of cardiac
McNitt, Mr Xia, Mr Polonsky, Dr Zareba); Ludwig-Maximilians-University,
and noncardiac marketed drugs commonly affecting
Munich, Klinikum Grosshadern, Department of Medicine 1, Munich,
the rapid components of the delayed rectifier potas-
Germany (Dr Kaab, Dr Hinterseer, Dr Beckmann); and iCardiac
sium current (I ) of the myocardial cells. However, if
Technologies Inc, Rochester, New York (Dr Fossa). Submitted for publication
I inhibition and QT interval prolongation are asso-
April 2, 2008; revised version accepted September 1, 2008. Address for cor-
ciated with the occurrence of drug-induced TdP,
respondence: Jean-Philippe Couderc, PhD, MBA, Box 653, Heart Research
they should not constitute a reason for considering a
Follow-Up Program, Cardiology Department, University of Rochester
drug to be proarrhythmic.1 The dissociation between
Medical Center, Rochester, NY 14642; e-mail: jean-philippe.couderc@heart.rochester.edu.
drug-induced QT interval prolongation2 and an
increased risk of arrhythmias is supported by the
6 • J Clin Pharmacol 2009;49:6-16 VENTRICULAR REPOLARIZATION AND HISTORY OF TORSADES DE POINTES
existence of drugs associated with a QT interval pro-
documented TdP in the context of a drug with QT-
longation but a limited history of TdP such as tamox-
prolonging potential: sotalol, sumatriptan, amiodarone,
ifen,3 carvedilol,4 and, more recently, ranolazine,
bisacodyl, cipramil, furosemide, clarithromycin,
which seems to prolong the QT interval duration while
erythromycin, or roxythromicin. The patients were
reducing ventricular heterogeneity.5 Consequently, the
enrolled for an evaluation of the individual level of
rejection of a novel drug because of its QT-prolong-
repolarization reserve, and all patients signed informed
ing effect is a rather dubious strategy because it
consent to receive doses of sotalol as described pre-
might deprive patients of a valuable medication.
viously.12 They were all genetically tested for the pres-
Improving the assessment of drug cardiotoxicity
ence of a mutation of the major LQTS genes using
linked to the ventricular repolarization process
standard genotyping techniques (genomic DNA was
could depend on the development of better electro-
prepared from lymphocytes, and amplification of
cardiographic markers than QT prolongation.
KCNQ1, KCNH2, KCNE1, KCNE2, and SCN5A using
The triggering mechanism(s) of drug-induced TdP
polymerase chain reactions was performed, followed
remains to be elucidated, but there are several inter-
by direct sequencing of these major LQT-disease
esting alternatives currently proposed: Hondeghem
genes). The control group consisted of patients who
et al suggested the TRiaD concept, emphasizing the
were started on sotalol for the prevention of parox-
role of action potential triangulation, reverse use
ysmal atrial fibrillation and had given informed
dependence of the drug, and repolarization instabil-
ity.6,7 The triangulation of the action potential andthe heterogeneity of electrical properties of the cells
Study Protocol and Electrocardiogram Recordings
across the myocardium are consistent with theproarrhythmic factors described by Belardinelli
The study protocol was described by Kaab et al.12
et al8: the transmural dispersion of repolarization and
Briefly, dl-sotalol was given intravenously at a constant
the promoting role of early after-depolarization.9,10
rate over a 20-minute interval at a dose of 2 mg/kg body
Finally, the concept of repolarization reserve described
weight in 50 mL of a 0.9% saline solution in a group of
by Roden11 emphasizes the role of the interplay
individuals with (+TdP) and without (-TdP) a history
of ion currents involved in cardiac repolarization.
of drug-induced TdP. Tests were performed in the
These currents provide functional redundancy, or
morning. Sotalol was injected to unmask latent repo-
“reserve,” and can protect an individual against
larization abnormalities while patients were closely
excessive QT prolongation by drugs. Also, gender,
and continuously monitored in the intensive care unit.
hypokalemia, predisposing DNA polymorphism,
Continuous 5-minute surface 12-lead ECG recordings
and environmental factors are recognized to be
(Mortara Instrument, Milwaukee, Wisconsin) were
potential modulators of the ventricular repolariza-
acquired at rest in the supine position at baseline and
tion process. They can lead to a reduced repolariza-
at 20-minute steady-state phase after injection. We
tion reserve and an increased propensity to
obtained access to 2 ECG tracings per individual at
baseline and on peak concentration of the drug.
In this study, we hypothesize that patients with a
The measurements of the PR and QRS durations
history of drug-induced TdP have a certain level of
from the 5-minute ECGs were provided by the
repolarization impairment (heterogeneity, reduced
Mortara SuperECG software (SuperECG, Mortara
repolarization reserve, and instability) that can be
Instrument). The RR intervals and repolarization
measured from their digital surface electrocardio-
intervals were based on technology developed at the
gram (ECG). Increased QT duration, repolarization
University of Rochester Medical Center (Rochester,
heterogeneity, and QT variability are investigated at
New York). The COMPAS software provided the loca-
baseline and when the patients are exposed to a tor-
tion of the end of the T wave based on a technique
identifying the crossing point between the baselineand the descending slope of the T wave (least squares
technique).13 The apex of the T wave relied on amethod using a parabola fit of the T wave where the
Study Population
maximum of the parabola identified the location ofthe apex. Baseline wandering was adjusted using
The patients were enrolled after being admitted to
Spline interpolation.13 The amplitude of the T wave
the University Hospital of Munich, Germany, for
was measured at the apex of the T wave.14
Description of the vectocardiographic measurements of the early (ERD) and late (LRD) repolarization measurement. The, with 30% representing the threshold used for identifying the length of these intervals from the Tloop (upper panel) and its corresponding intervals on the first eigenvector (lower panel). ERD encompasses an interval spreading towardthe QRS complex, whereas LRD encompasses an interval toward the end of the T-wave.QT Interval Measurements From the
repolarization signal, and (2) it is independent from
Scalar Electrocardiograms
the determination of the end of the T wave. Suchapproach requires that the patients remain at rest
The computer-based end of the T wave was visually
during the ECG recording to avoid high heart rates
checked by trained technicians and manually
(ie, short RR intervals in which the T wave would be
adjusted using the on-screen caliper available in the
encompassed 220 ms prior to the next R peak).
COMPAS software, if the automatic algorithm failed
The method is based on the singular value
to correctly identify the end of the T wave (semi-
decomposition (SVD) of the RIs from the 12-lead
computerized method). The QT interval measure-
signals. SVD is used to reduce the dimension of
ments were done in 3 cardiac beats in sinus rhythm
the ECG lead systems from 12 leads to 2 leads.16
from lead V5 (or II), and the median value from these
We refer to the resulting 2 leads as the eigenvectors
3 measures was computed. We report both the scalar
1 (ev ) and 2 (ev ). We measured the QT, QTapex,
computerized and semi-computerized QT interval
and the TpTe intervals (TpTe = QT – QTapex) from
measurements expressed in milliseconds. Recently,
ev . The apex and the end of the T wave were iden-
Liu et al9 reported the presence of an increased T
tified in a fully computerized manner using the
peak to T end interval (TpTe)/QT ratio prior to the
method described above for scalar measurements.
development of TdP in a rabbit wedge preparation.
We called the T loop the representation of the RI in
This novel parameter was included in our analysis
the 2-dimensional space, defined by ev and ev
to investigate its interest when measured from
(upper panel of Figure 1). The vector describing
the T loop path across time is the repolarizationvector. T Loop Measurements
The early repolarization duration (ERD) and the
late repolarization duration (LRD) are measurements
In our analysis, the repolarization interval (RI) is
of interval duration based on the T loop. The start-
defined between the J point and the point located
ing point of these intervals is the time at which the
220 ms before the next R peak. The determination of
length of the repolarization vector is maximized
the J point was based on an algorithm developed
in the upper panel of Figure 1). The ending
by Zong at al.15 This ensures that (1) the analysis
point of these intervals is delimited by a circle of
encompasses all components of the ventricular
8 • J Clin Pharmacol 2009;49:6-16 VENTRICULAR REPOLARIZATION AND HISTORY OF TORSADES DE POINTES
(Figure 1). Consequently, these parameters mea-
Statistical Analysis
sure the time needed for the heart vector to varyfrom its maximum length to a time point corre-
Differences between groups were expressed as mean
sponding to a 30% reduction of its maximum length
± standard deviation. The analysis of correlation
between values of various parameters was based on
sure toward the end of the RI, and ERD is directed
Spearman rank correlation, and we report its associ-
toward the J point (see Figure 1, lower panel). The
ated coefficients (ρ). P values less than or equal to
duration of these time intervals increases when the
.05 were considered statistically significant. We
heart vector slows down or/and the roundness of the
used logistic regression models to describe the asso-
T loop increases. Consequently, these parameters
ciation between baseline ECG measures and the
measure repolarization duration (reflected in the
level of drug-induced ECG changes. When we inves-
velocity of the heart vector) and the repolarization
tigated the presence of a history of TdP as the pri-
heterogeneity (reflected in the path of the heart vec-
mary endpoint, binary logistic regression models
were used, and both the best subsets regression pro-cedure and the stepwise procedure were used to
Heart Rate Correction
select the optimal models. The statistical analyseswere done using SAS (SAS Institute, Cary, North
All repolarization measurements were heart rate cor-
rected using the pooled technique. A linear regres-sion analysis was used to model the relationship
between repolarization measurements and RR inter-vals during baseline periods. The slope (β) charac-
Study Population
terizing this relationship was used to correct therepolarization measurements such as QTc = QT +
The clinical characteristics of the study population
β(1 – RR) for the QT interval. The same heart rate
are provided in Table I. The average ages of the pop-
correction technique was applied to all other
ulations were not significantly different between the
2 groups: 59 ± 13 years versus 61 ± 12 years. Thenumber of women was slightly higher (n = 12) in
QT Variability
the group of individuals without TdP than in thegroup with TdP (n = 9). Presence of a history of
The instability of the repolarization was estimated
myocardial infarction, coronary artery disease, and
using the median absolute deviation (MAD) of the
hypertension was similar between the study groups.
beat-to-beat measurements of the semi-computerized
There were several patients with a history of atrial
QT and QTapex parameters after heart rate correc-
fibrillation in both groups (+TdP: n = 11 and –TdP:
tion based on the pooled formula. To further control
n = 17, P < .05). One of the patients had atrial fibril-
for the effect of RR variation, we divided these MAD
lation during the ECG recording. This ECG was
values by the MAD of the RR intervals (MAD
removed from the analysis, resulting in a group of 16
patients with a history of TdP and 17 individualsfree of such history. Heart Rate Variability
The group of individuals with a history of drug-
induced TdP has been reported using a heteroge-
The heart rate variability (HRV) was estimated
neous list of medications. Seven of the patients had
from the 5-minute recordings using an autoregres-
sotalol-induced TdP. None of the patients in the
sive method. The normalized high- (HFnorm)
study experienced episodes of TdP during the sotalol
and low-frequency (LFnorm) components, expre-
challenge, and none of them carried a mutation
ssed in percentages, were computed using the
linked to the major congenital forms of the LQTS.
SuperECG software (Mortara Instrument). The def-
Tables II and III provide the ECG-based parame-
inition of the frequency bands for the HF and LF
ters across populations for the baseline recordings
components was recommended by the European
and for the sotalol-induced changes, respectively. PR
Task Force.17 The standard deviation from normal-
and QRS durations were not significantly different
to-normal intervals (SDNN) was also computed in
between groups at baseline and after drug. As shown
in Table III, the RR intervals were significantly
results using the semi- or fully computerized
method in baseline conditions (Table II). The groupof +TdP patients had a longer QT interval duration
Drug Inducing TdP
(~25 ms) than –TdP patients. We identified 6 patientswith a QTc duration above the gender-specific
Group With History of Torsades de Pointes
QTc >470 ms in men). One of them was a woman
from the control group (-TdP); the remaining ones
were from the +TdP group and included 3 men and
Vectorial measurements. At baseline, the vectorial
QT measurements (from ev ) were slightly longer
than the scalar QT intervals, but the difference
between the study groups remained consistent (26
ms). According to the vectorial parameters, this pro-
longation was localized within the early part of the
(P = .02), and this prolongation reached 14 ms with
(P = .03). Interestingly, this delay in the early
phase of the repolarization segment was not cap-
Group Without History of Torsades de Pointes
tured by the QTapex interval (from ev ), suggesting
that the morphology of the T loop (ventricular het-
erogeneity) primarily drives this delay.
Our investigation of QT variability reveals a trend
toward larger variability in baseline ECGs of +TdP
patients, but this difference did not reach statistical
Sotalol-Induced Prolongation, Heterogeneity, and Instability of Repolarization Scalar measurements. Sotalol is associated with
strong prolongation of the QTc interval duration,
and this was true for the 2 groups (+TdP: 85 ± 42 and
–TdP: 65 ± 47 ms). These changes were statistically
different from zero (P < .0001) but not statisticallydifferent between groups (P = .22) when considering
Y/N, yes/no; EF, left ventricular ejection fraction; CAD, coronary artery
single lead-based measurements. Similar results
disease; MI, myocardial infarction; HT, history of hypertension; AF,history of atrial fibrillation; TdP, Torsades de Pointes.
were found using the scalar computerized technique(+TdP: 63 ± 57 and –TdP: 56 ± 41 ms, P = .70).
The ratio of the terminal part of the T wave to the
QTc interval was not significantly different between
longer after sotalol (+TdP: 201 ± 101 ms and -TdP:
175 ± 98 ms, P < .05), but the bradycardic effect ofthe drug was not different between groups (P = .45). Vectorial measurements. There was a significantsotalol-induced QTc and QTc apex prolongation (P <
Baseline Duration, Heterogeneity,
.01) within the 2 study groups. It is noteworthy that
and Instability of Repolarization
QTc measured from ev did reveal statistically sig-
nificant prolongation in the +TdP group (75 ± 44 vs
Scalar measurements. In comparison to the scalar
37 ± 26 ms, P = .008). This observation is consistent
QTc interval measurements, we found similar
with Kaab and coworkers’ results12 evidencing
10 • J Clin Pharmacol 2009;49:6-16 VENTRICULAR REPOLARIZATION AND HISTORY OF TORSADES DE POINTES
Description of Baseline Values of Electrocardiographic Parameters
Baseline (Absolute Values)
−TdP (n = 17)
+TdP (n = 16) P Values
-TdP, patients without a history of TdP; +TdP, patients with a history of TdP; TpTe, T peak to T end interval in lead II; ERD, early repolarization dura-tion; LRD, late repolarization duration (for definition of the ERD and LRD parameters, see text); HF, high frequency; LF, low frequency; MAD, medianabsolute deviation; HRV, heart rate variability; SDNN, standard deviation from normal-to-normal intervals; TdP, Torsades de Pointes. Values associatedwith P < .05 are in bold. NU, no unit. a. These measurements are corrected using the pooled formula and expressed in milliseconds.
significantly larger sotalol-induced QT prolongation
levels of QT variability was found in ECGs recorded
between patients with and without a history of TdP
using the maximum QT interval from all availableleads. More interestingly, sotalol significantly pro-
Characterizing Patients With a
longed the late part of the repolarization in the
History of Torsades de Pointes
group of patients with a history of TdP: their TpTeinterval prolongation was longer (23 ± 27 vs 4 ± 12
Binary logistic regressions were implemented to
find which baseline information could help predict
III) values were more prolonged (20 ± 29 vs 2 ± 14 ms,
the presence of a history of TdP in a multivariate
fashion. The QTc, QTc apex, TpTe, TpTe/QTc,
No significant changes in SDNN values and LF
norm values were found after sotalol in any of the
the design. Based on both stepwise and best subsets,
study groups. But the high-frequency norm revealed a
trend toward increased parasympathetic innervations
predictor of a history of TdP. For each incremental 1-
in the group of patients with a history of TdP (–TdP:
6.7% ± 11.7% vs +TdP: 14.5% ± 8.1%, P = .05).
odds of having a history of TdP (P = .016). The sec-
The variability of the QTc and QTc apex interval
durations, adjusted for heart rate, was measured
ated with a 41% increase for each 0.1 increase in
value (P = .066). Baseline QTc or TpTe intervals did
Table III
Description of Sotalol-Induced Changes in Values of Electrocardiographic Parameters
Sotalol Challenge (Sotalol-Induced Changes)
−TdP (n = 17)
+TdP (n = 16) P Values 6.7 ± 11.7 14.5 ± 8.1*
-TdP, patients without a history of TdP; +TdP, patients with a history of TdP; TpTe, T peak to T end interval in lead II; ERD, early repolarization dura-tion; LRD, late repolarization duration (for definition of the ERD and LRD parameters, see text); HF, high frequency; LF, low frequency; MAD, medianabsolute deviation; HRV, heart rate variability; SDNN, standard deviation from normal-to-normal intervals; TdP, Torsades de Pointes. Values associatedwith P < .05 are in bold. Testing if the average is different from 0: *P < .01. NU, no unit. a. These measurements are corrected using the pooled formula and expressed in milliseconds.
not contribute to the model despite the presence of
None of the other ECG measurements entered the
5 patients with a prolonged QTc interval at baseline
model—that is, neither baseline QT interval dura-
tion nor baseline TpTe interval contributed to the
A second logistic model was implemented consid-
prediction of sotalol-induced TpTe prolongation.
ering the sotalol-induced TpTe interval prolongation
On the basis of these results, we report in the
as a primary continuous endpoint and baseline ECG
upper panel of Figure 2 the scatterplots for ERD30%
measurements as covariates. Again, both ERD
and QT variability values in the 2 study groups at
history of TdP, one can separate the 2 groups with
was a 1.8-ms increment in TpTe interval value with a
100% specificity and 69% sensitivity. The 6 indi-
strong statistical significance (P = .0002). A univariate
viduals presented prolonged QT intervals on their
baseline ECGs (LQTS) based on the following clini-
induced prolongation of TpTe was significant (r2 = 31%,
cal criterion: QTc >480 ms in women and QTc >470
ms in men (see Figure 2). One may note that 7
patients without clinically identifiable LQTS were
detected by our novel parameters. Among them, 3
in the TpTe interval on sotalol (P = .01).
patients have borderline QTc (450 ms > QTC >470 ms),
12 • J Clin Pharmacol 2009;49:6-16 VENTRICULAR REPOLARIZATION AND HISTORY OF TORSADES DE POINTESDistribution of heart rate–corrected values for ERDand the values of QT variability (upper panel) in baseline electrocar-diograms (ECGs) for our study populations marking the patients with long QT interval duration (based on gender-specific criteria of thelong QT syndrome). The sotalol-induced changes of TpTe and QTc interval (computerized) are reported in the lower panel. The grayareas in both panels represent the range of values in which most patients without history of Torsades de Pointes (TdP) are located. Thevertical and horizontal lines define the values of the parameter thresholds.
and 4 have normal QTc interval duration.
TdP had a specific repolarization profile similar to
Consequently, using a criterion based on QTc >450
the one we observed in ECGs of healthy participants
ms to identify patients with increased risk would
on moxifloxacin—namely, changes in morphology
provide a sensitivity of 50% and a specificity of
of the T wave prior to the T wave apex.16 It is note-
76%. This univariate analysis confirms our observa-
worthy that the T wave from LQT2 patients with
tions from the multivariate analysis that our novel
borderline QTc interval duration (390-440 ms) also
ECG parameters are bringing complementary infor-
shows an abnormal early portion of the T wave
(quantified using the left slope of the T wave). This
Figure 2 also provides the scatterplot of values of
information helps to better identify patients carrying
sotalol-induced changes for TpTe and QTc intervals.
the KCNH2 mutation from noncarrier family
We defined thresholds for maximizing the separa-
members.14 In this study group, patients did not
tion between the 2 groups as the sotalol-induced
carry any of the major LQTS mutations, but our
changes in TpTe >50 ms and in QTc >83 ms, and the
observations might also reveal the presence of a
groups can be separated with 94% specificity and
reduced repolarization reserve. Indeed, unrecog-
75% sensitivity based on these thresholds.
nized repolarization modulators could be presentsuch as nondocumented drugs, underlying cardiac
DISCUSSION
disease, and predisposing genetic factors (nonidenti-fied congenital long QT syndrome).
We report the analysis of ventricular repolarization
When patients with a history of TdP are exposed
duration, heterogeneity, and instability in a group of
to the torsadogenic compound sotalol, the repolar-
individuals with and without a history of drug-
ization abnormalities are not limited to the early part
induced TdP. We investigated ECG abnormalities
of the T wave but extend to the late portion of the T
that could be linked to arrhythmogenic factors con-
wave. Our results show that the late part of the T
tributing to trigger and maintain drug-induced TdP.
wave, measured either by the TpTe interval or the
Repolarization heterogeneity and instability were
parameters, is more significantly prolonged
assessed from surface ECGs based on the T loop
during an infusion of sotalol in patients with a
morphology (ERD and LRD parameters) and QT vari-
history of TdP than in patients without such history.
ability. The assessment of reverse use dependency of
In human studies, Smetana et al22 investigated the
sotalol using QT/RR modeling was not included in
TpTe interval duration in the European Myocardial
our analysis because the ECG recordings were too
Infarction Amiodarone Trial (EMIAT) population,
short to reliably assess the QT/RR relationship.18
comparing the length of this interval between
The baseline ECGs of patients with a history of
patients who died or did not die of cardiac arrhyth-
TdP revealed more pronounced repolarization
mic events. The results suggested a significant pro-
abnormalities in comparison to the ECGs of patients
longation of the TpTe interval in patients who died
without such history. This increased repolarization
in the placebo group (71 ± 3 vs 66 ± 1 ms, P = .04).
variability measured from baseline ECGs was not
Interestingly, this difference was not found in the
significantly different between the 2 study groups,
group of patients on amiodarone (both groups had
but the multivariate analysis suggested that this
long TpTe intervals of 79 ± 6 vs 73.2 ± 2 ms, P = .17).
variability contributed to better classify these
The ratio between TpTe and QT interval was not
groups. Such observation is consistent with the beat-
longer in patients with a history of TdP. This obser-
to-beat variability of QT described in the study
vation is not consistent with Liu et al’s work9 report-
reported by Hinterseer et al.19 This instability of
ing increased values of this ratio prior to the
repolarization is 1 of 3 components of the TriAD
occurrence of TdP in a rabbit model.
concept, and its proarrhythmic role has been docu-
Our study suggests that the prolongation of the
mented in several clinical studies that have reported
QT intervals at baseline and on sotalol in patients
their independent predicting value for appropriate
with a history of TdP is associated with an unevenly
implantable cardio-defibrillator therapy in postin-
distributed delay across the repolarization interval.
These observations fit the arrhythmogenic concept,
At baseline, our investigation revealed that the
enhancing the role of the TpTe interval prolongation
repolarization delay was prominently located in the
as an important proarrhythmic factor.9,10 Animal and
early part of the T wave prior to its apex. Thus, a
clinical investigations have emphasized that a pro-
large set of patients with a history of drug-induced
longation of the QT interval might be more or less
14 • J Clin Pharmacol 2009;49:6-16 VENTRICULAR REPOLARIZATION AND HISTORY OF TORSADES DE POINTES
malignant according to the location of the abnormal-
In this study, we used individuals with prior
ity inside the T wave in erythromycin-induced
documented TdP induced by various types of QT-
LQTS, in arterially perfused wedges from the canine
prolonging drugs. We do not have information about
left ventricle,23 and in cases of Brugada syndrome.24
drug level and triggering events in these patients.
Finally, a univariate analysis of the correlation
Also, none of the patients in the group with a history
between repolarization parameters at baseline and
of TdP had an episode of TdP while on sotalol. Even
if one does not fully understand the mechanisms
significantly correlated with sotalol-induced TpTe
involved in the triggering of drug-induced TdP, one
prolongation (r2 = 31%, P < .0001). Our logistic
could speculate that if sotalol strongly impaired the
models confirm this strong relationship and suggest
repolarization process, it might not set up all compo-
that a prolongation of the late and the early part of
nents needed for triggering TdP in our patients with
the repolarization signal are not independent. The
a torsadogenic predisposition. It has been shown in
mechanism underlying this dependency remains to
clinical studies of patients with the congenital long
QT syndrome that there are crucial environmental
The values of the time domain HRV parameter
factors known to trigger the occurrence of cardiac
and of the high-frequency components were very
arrhythmias. Schwartz et al28 observed that in LQT2
similar to the HRV indices reported in normal partic-
patients (patients with reduced I kinetics), most car-
ipants for short-term recordings using an autoregressive
diac events occur following an emotional stress event
method.25 But our study groups were characterized
(abrupt neurally mediated release of norepinehrine),
by a vagally driven regulation of the heart rate at
whereas LQT1 patients have events during exercise.
baseline. A parasympathetically driven regulation is
In LQT1 patients, the risk for arrhythmic events is
known to increase QT interval duration: Viitasalo
increased when the protective effect of the I current
and Karjalainen26 have shown an 18-ms QT prolon-
does not “kick in” at a high heart rate. Such cardiac
gation during night compared with day recordings
stress events were not included in our experiment
for the same level of heart rate (60 bpm). The pro-
but could have been crucial triggering events of TdP
longation of the QT interval under vagal influence
has been confirmed by Bexton et al,27 who investi-
Finally, Hong et al29 suggested that patients with
gated the influence of the autonomic nervous system
atrial fibrillation may have a shortening of the QT
(ANS) on the QT interval. For these reasons, we
interval. The KCNH3-K897T polymorphism associ-
believe it is important to combine information about
ated with atrial fibrillation30 is suggested to be also
the repolarization changes and the presence of an
associated with QT shortening based on large
“atypical” regulation of the heart by the ANS. In our
cohorts of patients from the MONICA, KORA, and
study, the group of patients with a history of TdP
Framingham Heart Studies.31 One must acknowl-
was associated with a statistically significant
edge that our study groups are both primarily con-
sotalol-induced increased parasympathetic regula-
stituted by patients with a history of atrial
tion of the heart rate that could mean that these
fibrillation: all -TdP patients and 11 of 16 patients in
patients might have an increased sensibility to a
beta-adrenergic blocking property of dl-sotalol,enhancing their increased propensity to repolariza-
Conclusion
tion delay and to ventricular heterogeneity.
It is important for clinicians and for pharmaceutical
Limitations of the Study
companies to be able to assess the level of predispo-sition to TdP of an individual. When comparing the
The size of the study population was rather small
ECGs from patients with and without a history of
but contained a large set of ECG recordings from
TdP, our results suggest that patients with a history
patients with history of TdP. As far as we know, it is
of drug-induced TdP have specific T wave mor-
the largest set of digital ECGs in a group of patients
phologies on their baseline ECGs. When challenged
with a history of such rare arrhythmias. The logistic
by sotalol, the patients with a history of TdP have
model developed in our study has a limited value as
a significantly longer late portion of the T wave
a predictive tool until it is validated on an indepen-
than the patients without such history. We believe
this information could help optimize therapeutic
strategies for cardiologists and improve the design of
15. Zong W, Moddy G, Jiang D. A robust open-source algorithm to
detect onset and duration of QRS complexes. Comput Cardiol. 2003;30:737-740.
We thank Meijian Zhou from iCardiac Technologies, Inc for
16. Couderc JP, Vaglio M, Xia X, McNitt S, Hyrien O.
valuable support during the analysis of these data.
Electrocardiographic method for identifying drug-induced repo-larization abnormalities associated with a reduction of the rapidly
Financial disclosure: This work has been partially funded
activating delayed rectifier potassium current. Conf Proc IEEE
from unrestricted grants from iCardiac Technologies, Inc and
Eng Med Biol Soc. 2006;1:4010-4015. 17. Heart rate variability: standards of measurement, physiologi- cal interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing REFERENCES
and Electrophysiology. Circulation. 1996;93:1043-1065. 18. Couderc JP, Xiaojuan X, Zareba W, Moss AJ. Assessment of the 1. Shah RR, Hondeghem LM. Refining detection of drug-induced
stability of the individual-based correction of QT interval for
proarrhythmia: QT interval and TRIaD. Heart Rhythm. 2005;2:
heart rate. Ann Noninvasive Electrocardiol. 2005;10:25-34. 19. Hinterseer M, Thomsen MB, Beckmann BM, et al. Beat-to-beat 2. Roden DM. Drug-induced prolongation of the QT interval. N
variability of QT intervals is increased in patients with drug-
Engl J Med. 2004;350:1013-1022.
induced long-QT syndrome: a case control pilot study. Eur Heart3. Liu XK, Katchman A, Ebert SN, Woosley RL. The antiestrogen
tamoxifen blocks the delayed rectifier potassium current, IKr, in
20. Couderc JP, Zareba W, Maison-Blanche P, Moss AJ.
rabbit ventricular myocytes. J Pharmacol Exp Ther. 1998;287:
Repolarization variability in the risk stratification of MADIT II
patients. Europace. 2007;9:717-723. 4. Akdeniz B, Guneri S, Savas IZ, et al. Effects of carvedilol ther- 21. Haigney MC, Zareba W, Gentlesk PJ, et al. QT interval vari-
apy on arrhythmia markers in patients with congestive heart fail-
ability and spontaneous ventricular tachycardia or fibrillation in
ure. Int Heart J. 2006;47:565-573.
the Multicenter Automatic Defibrillator Implantation Trial
5. Antzelevitch C, Belardinelli L, Zygmunt AC, et al. Electro-
(MADIT) II patients. J Am Coll Cardiol. 2004;44:1481-1487.
physiological effects of ranolazine, a novel antianginal agent with
22. Smetana E, Pueyo K, Hnatkova V, et al. Effect of amiodarone on
antiarrhythmic properties. Circulation. 2004;110:904-910.
the descending limb of the T wave. Am J Cardiol. 2003;92:742-746. 6. Hondeghem LM, Carlsson L, Duker G. Instability and triangu- 23. Antzelevitch C, Sun ZQ, Zhang ZQ, Yan GX. Cellular and ionic
lation of the action potential predict serious proarrhythmia, but
mechanisms underlying erythromycin-induced long QT intervals
action potential duration prolongation is antiarrhythmic.
and Torsade de Pointes. J Am Coll Cardiol. 1996;28:1836-1848. Circulation. 2001;103:2004-2013. 24. Castro HJ, Antzelevitch C, Tornes BF, et al. Tpeak-Tend and 7. Hondeghem LM. TRIad: foundation for proarrhythmia (triangu-
Tpeak-Tend dispersion as risk factors for ventricular tachycar-
lation, reverse use dependence and instability). Novartis Found
dia/ventricular fibrillation in patients with the Brugada syn-
drome. J Am Coll Cardiol. 2006;47:1828-1834. 8. Belardinelli L, Antzelevitch C, Vos MA. Assessing predictors of 25. Pitzalis MV, Mastropasqua F, Massari F, et al. Short- and long-
drug-induced Torsade de Pointes. Trends Pharmacol Sci. 2003;24:
term reproducibility of time and frequency domain heart rate
variability measurements in normal subjects. Cardiovasc Res. 9. Liu T, Brown BS, Wu Y, Antzelevitch C, Kowey PR, Yan GX.
Blinded validation of the isolated arterially perfused rabbit ven-
26. Viitasalo M, Karjalainen J. QT intervals at heart rates from 50
tricular wedge in preclinical assessment of drug-induced proar-
to 120 beats per minute during 24-hour electrocardiographic
rhythmias. Heart Rhythm. 2006;3:948-956.
recordings in 100 healthy men: effects of atenolol. Circulation. 10. Yan GX, Wu Y, Liu T, Wang J, Marinchak RA, Kowey PR.
Phase 2 early afterdepolarization as a trigger of polymorphic ven-
27. Bexton RS, Vallin HO, Camm AJ. Diurnal variation of the QT
tricular tachycardia in acquired long-QT syndrome: direct evi-
interval: influence of the autonomic nervous system. Br Heart J.
dence from intracellular recordings in the intact left ventricular
wall. Circulation. 2001;103:2851-2856. 28. Schwartz PJ, Priori SG, Spazzolini C, et al. Genotype-phenotype 11. Roden DM. Long QT syndrome: reduced repolarization
correlation in the long-QT syndrome: gene-specific triggers for
reserve and the genetic link. J Intern Med. 2006;259:59-69.
life-threatening arrhythmias. Circulation. 2001;103:89-95. 12. Kaab S, Hinterseer M, Nabauer M, Steinbeck G. Sotalol testing 29. Hong K, Bjerregaard P, Gussak I, Brugada R. Short QT syn-
unmasks altered repolarization in patients with suspected
drome and atrial fibrillation caused by mutation in KCNH2. J
acquired long-QT-syndrome: a case-control pilot study using i.v. Cardiovasc Electrophysiol. 2005;16:394-396.
sotalol. Eur Heart J. 2003;24:649-657. 30. Sinner MF, Pfeufer A, Akyol M, et al. The non-synonymous 13. Lepeschkin E, Surawicz B. The measurement of the Q-T inter-
coding IKr-channel variant KCNH2-K897T is associated with
val of the electrocardiogram. Circulation. 1952;6:378-388.
atrial fibrillation: results from a systematic candidate gene-based
14. Couderc JP, McNitt S, Xia J, Zareba W, Moss AJ. Repolarization
analysis of KCNH2 (HERG). Eur Heart J. 2008;29:907-914.
morphology in adult LQT2 carriers with borderline prolonged QTc
31. Ellinor PT, Milan DJ. Polymorphisms and atrial fibrillation:
interval. Heart Rhythm. 2006;3:1460-1466.
sorting the wheat from the chaff. Eur Heart J. 2008;29:843-845. 16 • J Clin Pharmacol 2009;49:6-16
Environmental Management Unit, Monash University, NTRODUCTION DESIGN FOR THE SOUTH WEST SLOPES A design prepared in 1997 has been used to illustrateCommercial plantation forestry in Australia has beenthe concepts of analogue forestry. The property isfocused on producing timber products at minimal costlocated near Jindera on the southern margin of theand in the shortest time possible.
Política de Investimentos 2011 Sumário 1 – Introdução.03 2 – Características do RPPS.04 2.1 – Estrutura organizacional para tomada de decisões de 2.2 – Atribuições dos órgãos mencionados nos subitens 3 – Objetivos.07 4 – Diretrizes de alocação dos recursos.08 4.2 – Objetivos da gestão de alocação.08 4.3 – Faixas de alocação de r
 Baseline Values and Sotalol-Induced Changes of Ventricular Repolarization Duration,
Baseline Values and Sotalol-Induced Changes of Ventricular Repolarization Duration,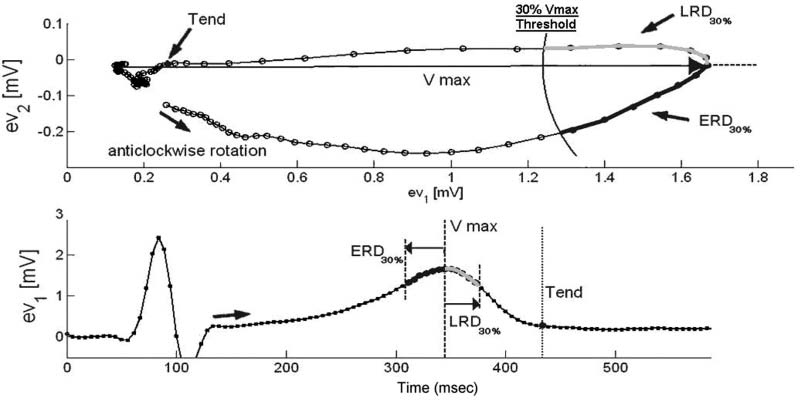 Description of the vectocardiographic measurements of the early (ERD) and late (LRD) repolarization measurement. The
, with 30% representing the threshold used for identifying the length of these intervals from the T
loop (upper panel) and its corresponding intervals on the first eigenvector (lower panel). ERD encompasses an interval spreading towardthe QRS complex, whereas LRD encompasses an interval toward the end of the T-wave.
QT Interval Measurements From the
Description of the vectocardiographic measurements of the early (ERD) and late (LRD) repolarization measurement. The
, with 30% representing the threshold used for identifying the length of these intervals from the T
loop (upper panel) and its corresponding intervals on the first eigenvector (lower panel). ERD encompasses an interval spreading towardthe QRS complex, whereas LRD encompasses an interval toward the end of the T-wave.
QT Interval Measurements From the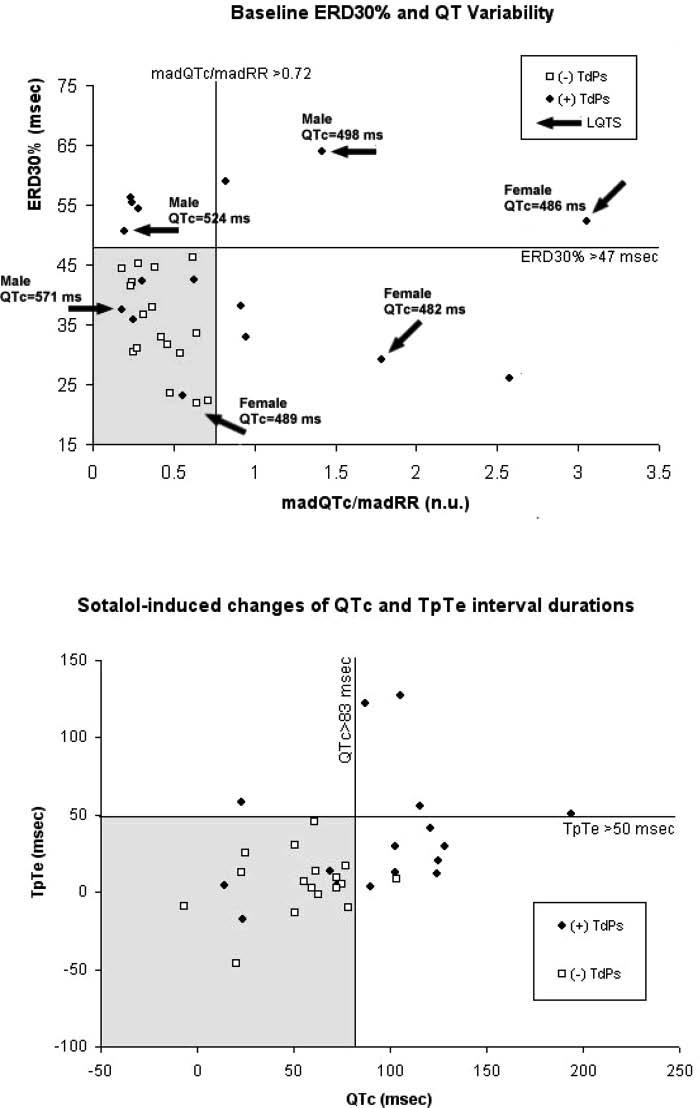 VENTRICULAR REPOLARIZATION AND HISTORY OF TORSADES DE POINTES
Distribution of heart rate–corrected values for ERD
and the values of QT variability (upper panel) in baseline electrocar-
diograms (ECGs) for our study populations marking the patients with long QT interval duration (based on gender-specific criteria of thelong QT syndrome). The sotalol-induced changes of TpTe and QTc interval (computerized) are reported in the lower panel. The grayareas in both panels represent the range of values in which most patients without history of Torsades de Pointes (TdP) are located. Thevertical and horizontal lines define the values of the parameter thresholds.
and 4 have normal QTc interval duration.
VENTRICULAR REPOLARIZATION AND HISTORY OF TORSADES DE POINTES
Distribution of heart rate–corrected values for ERD
and the values of QT variability (upper panel) in baseline electrocar-
diograms (ECGs) for our study populations marking the patients with long QT interval duration (based on gender-specific criteria of thelong QT syndrome). The sotalol-induced changes of TpTe and QTc interval (computerized) are reported in the lower panel. The grayareas in both panels represent the range of values in which most patients without history of Torsades de Pointes (TdP) are located. Thevertical and horizontal lines define the values of the parameter thresholds.
and 4 have normal QTc interval duration.