La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Microsoft word - exenatide shared care protocol december 2008 .doc
East & North NHS and West Hertfordshire Health Systems
EXENATIDE (BYETTA®) IN TYPE 2 DIABETES SHARED CARE CRITERIA Patients will have been stabilised, receiving a therapeutic dose of EXENATIDE allowed for common adverse events and side effects to have occurred before referral to the GP. A minimum period of 1 month stabilisation is necessary prior to sharing care. RESPONSIBILITIES
Consultant 1. Send a standard letter (giving patient pilot number) to GP requesting shared care for this patient. 2. Initiate treatment and prescribe the first 1 month treatment. 3. Clinical and laboratory supervision (as per proforma) of patient by routine clinic follow-up. 4. Advise GP on review, duration and discontinuation of treatment where necessary. 5. To discuss with patient the risks versus the benefits of the treatment. 6. Evaluation of any adverse effects reported by GP or patient. 7. Ensure that back-up advice is available at all times. General Practitioner 1. Monitoring patient’s overall health and well being. 2. Report any adverse events reported by the patient to consultant and CSM where appropriate. 3. Prescribe maintenance exenatide therapy as described above. 4. To return a copy of the standard letter to the consultant and Primary Care Trust accepting or
Primary Care Trust 1. To provide manage the audit process by ensuring that a copy of the letter to GP is sent to
Rasila.shah@herts-pcts.nhs.uk giving patient i.d. and pilot number.
2. To support GPs in making the decision whether or not to accept clinical responsibility for
3. To support trusts in resolving issues that may arise as a result of shared care.
LICENSED INDICATIONS (relevant to this Shared Care Guideline)
For the treatment of Type 2 diabetes mellitus in combination with metformin and/or sulphonylureas in patients who have not achieved adequate glycaemic control on maximally tolerated doses of these oral therapies.
DOSE AND ADMINISTRATION
Starting dose 5ug twice a day. Maximum dose 10ug twice a day
Patients aged between 40 years to 70 years who fit the following criteria
Obese patients (BMI≥30kg/m2) who failed maximal dose of dual therapy (Metformin+Sulphonylurea, Metformin+Glitazone or Sulphonylurea+Glitazone)
ii. in whom add-on therapy of a drug in the third category is contraindicated or not
iii. they would otherwise be considered for insulin therapy.
Obese patients (BMI≥30kg/m2) who failed triple therapy (metformin+sulphonylurea+Glitazone)
with HbA1c between 8.4 and 10% who would otherwise need insulin therapy.
In these, patients, the addition of Exenatide will necessitate the withdrawal of Glitazone, as the later is not currently licensed with Exenatide
The information contained in this guideline is issued on the understanding that it is accurate based on the resources at the time of issue. For further
information please refer to the most recent Summary of Product Characteristics and British National Formulary.
East & North NHS and West Hertfordshire Health Systems
EXENATIDE (BYETTA®) IN TYPE 2 DIABETES
Professional drivers where insulin therapy may lead to withdrawal of their license.
Patients older than 70 years (trial population); BMI < 30kg/m2; HBA1c < 8.4%.
Severe renal impairment (creatinine clearance<30ml/min)
Diabetic gastropathy with recurrent vomiting
Gastro-intestinal disease with delayed gastric emptying and/or recurrent vomiting.
Post myocardial infarction (insulin preferred) unless insulin therapy declined.
Heart failure, pulmonary hypertension and liver failure (no safety data)
Gall stones or heavy alcohol intake (risk of pancreatitis)
1- Drug intolerance 2- Treatment failure (defined as failure to improve glycaemic control with less than 1%
improvement in HbA1c after 6 months of maximum-dose therapy)
3- Patient’s choice 4- Permanent occurrence of any of the exclusion criteria. 5- Failure to show significant improvement defined as a drop in HbA1c of 1% after 6 months. 6- Need for Insulin therapy or glitazone or gliptin. Exenatide is not licensed to be given with insulin,
Initiation, dosing and treatment monitoring (hospital-based):
Assessment of patient’s eligibility for treatment with Byetta will be undertaken by a consultant diabetologist in line with above criteria.
Treatment should be initiated by a consultant diabetologist in the hospital at a starting dose of 5µg sc twice daily 60 minutes before meals for at least one month in order to improve tolerability.
The dose can be increased to a maximum of dose of 10µg sc twice daily to further improve glycaemic control subject to absence of side effects or intolerance.
Technical aspects of Byetta injection and training will be provided by the Diabetes Specialist Nurses in the secondary care and supervision of care and dose adjustment of Byetta and other concomitant diabetic therapies should be the responsibility of the Diabetes Team in the hospital.
Comprehensive assessment at baseline and follow-up to be undertaken on the enclosed proforma.
Decision to introduce exenatide therapy should be clearly justified and communicated to patient’s GP in line with inclusion criteria.
Progress will be monitored in the specialist diabetes clinic in the hospital every 3 months or more frequently if necessary.
The outcome of each review should be communicated to the GP.
The information contained in this guideline is issued on the understanding that it is accurate based on the resources at the time of issue. For further
information please refer to the most recent Summary of Product Characteristics and British National Formulary.
East & North NHS and West Hertfordshire Health Systems
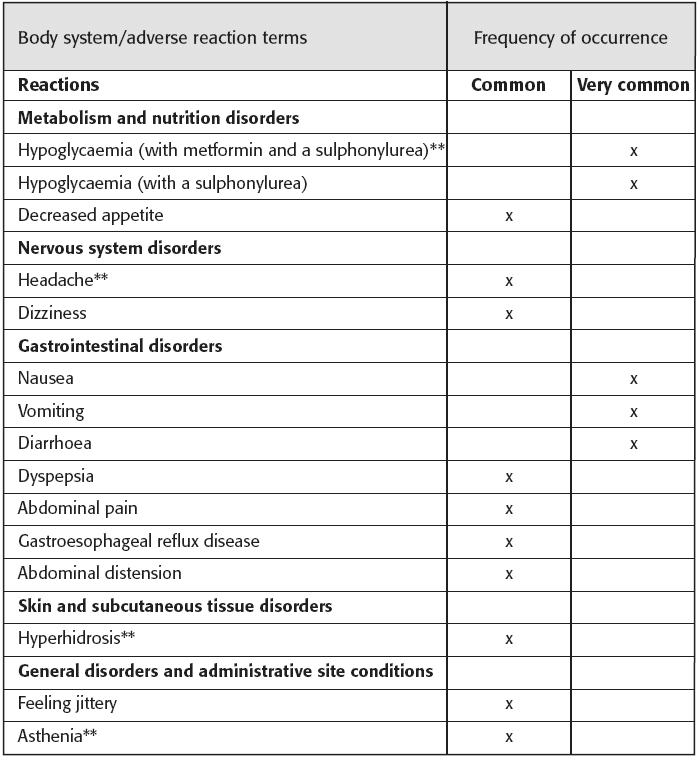
EXENATIDE (BYETTA®) IN TYPE 2 DIABETES Adverse Drug Reactions reported post-marketing Immune system disorders: Anaphylactic reaction, very rarely. Metabolism and nutritional disorders: Dehydration, generally associated with nausea, vomiting and/or diarrhoea, some reports associated with elevation of serum creatinine. Nervous system disorders: Dysgeusia, somnolence. Gastro-intestinal disorders: Eructation, constipation, flatulence. Pancreatitis, cases have been reported. Skin and subcutaneous tissue disorders: Macular rash, papular rash, pruritis, urticaria, angioneurotic oedema.
CONTRAINDICATIONS Hypersensitivity to the active substance or to any of the excipients. Byetta should not be used in patients with type 1 diabetes mellitus or for the treatment of diabetic ketoacidosis and is not recommended for use in patients with end-stage renal disease (creatinine clearance<30ml/min), severe renal impairment or severe gastrointestinal disease. Byetta should not be used in patients with type 2 diabetes who require insulin therapy due to beta-cell failure. Intravenous or intramuscular injection of Byetta is not recommended.5
The information contained in this guideline is issued on the understanding that it is accurate based on the resources at the time of issue. For further
information please refer to the most recent Summary of Product Characteristics and British National Formulary.
East & North NHS and West Hertfordshire Health Systems
EXENATIDE (BYETTA®) IN TYPE 2 DIABETES
Cost and estimated Impact to the NHS Usual daily dose range Approx. annual cost (Drug Tariff Dec 08) Exenatide £887.12
Costs for insulin are calculated on cartridge costs, assuming the patient is using 50 units daily of short acting insulin or 25 units daily of longer acting insulin.
Exenatide is cheaper than adding insulin to glitazones. Compared to insulin alone, exenatide is more expensive, unless dose of insulin exceed about 70 units of analogue insulin (insulin glargine).
CONTACT NUMBERS
East & North Hertfordshire NHS Trust
Dr Colin Johnson Hemel Hampstead hospital
Dr Chantal Kong Hemel Hampstead hospital
Dr Arla Ogilvie Watford general hospital
Dr Michael Clements Watford general hospital
Dr Julia Ostberg Watford general hospital
The information contained in this guideline is issued on the understanding that it is accurate based on the resources at the time of issue. For further
information please refer to the most recent Summary of Product Characteristics and British National Formulary.
APPENDIX A – Media and Solution Preparation Appendix A Regarding the present experimental research, a summary of recommended and standard aseptic techniques should be fol owed throughout every procedure, to ensure axenic conditions. Therefore al material in use should be sterilized by autoclaving (120ºC for 20 min), and al the procedures performed on a sterile bench (disinfected w
Mylène Valiquette-LavigneMarie-Ève Prayal-PratteCatherine LavigueurM.D. psychiatres, Hôpital Honoré-Mercier15 Juin 2010Revoir les indications des antipsychotiques en cas d’agitation, chez le patient en delirium et chez celui souffrant de démenceRéviser la présentation et le traitement du syndrome métabolique chez les patients sous antipsychotiquesRéviser les indications des antipsyc
 East & North NHS and West Hertfordshire Health Systems
East & North NHS and West Hertfordshire Health Systems  East & North NHS and West Hertfordshire Health Systems
East & North NHS and West Hertfordshire Health Systems 
 East & North NHS and West Hertfordshire Health Systems
East & North NHS and West Hertfordshire Health Systems  East & North NHS and West Hertfordshire Health Systems
East & North NHS and West Hertfordshire Health Systems