La t√©tracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l‚ÄôARNt sur la sous-unit√© 30S ribosomale, interrompant l‚Äô√©longation de la cha√ģne prot√©ique bact√©rienne. Ce m√©canisme conf√®re une activit√© sur un spectre large, incluant bact√©ries Gram positives, Gram n√©gatives, rickettsies et spiroch√®tes. Sa biodisponibilit√© digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magn√©sium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et g√©nito-urinaires. L‚Äô√©limination se fait par voie r√©nale et biliaire. Les effets ind√©sirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d‚Äôadministration pr√©coce. Les guides th√©rapeutiques mentionnent sumycin prix , en soulignant la n√©cessit√© de restreindre son utilisation afin de limiter les r√©sistances acquises.
Audiolab.usal.es
Inferred basilar-membrane response functions for listeners
Christopher J. Placka) and Vit Drga
Department of Psychology, University of Essex, Wivenhoe Park, Colchester, CO4 3SQ, England
Enrique A. Lopez-Poveda
Instituto de Neurociencias de Castilla y Leo¬īn, Universidad de Salamanca, Avda. Alfonso X ‚Äė‚ÄėEl Sabio‚Äô‚Äô s/n,37007 Salamanca, Spain
ÕĎReceived 3 September 2003; revised 5 January 2004; accepted 17 January 2004Õí
Psychophysical estimates of cochlear function suggest that normal-hearing listeners exhibit acompressive basilar-membrane ÕĎBMÕí response. Listeners with moderate to severe sensorineuralhearing loss may exhibit a linearized BM response along with reduced gain, suggesting the loss ofan active cochlear mechanism. This study investigated how the BM response changes withincreasing hearing loss by comparing psychophysical measures of BM compression and gain fornormal-hearing listeners with those for listeners who have mild to moderate sensorineural hearingloss. Data were collected from 16 normal-hearing listeners and 12 ears from 9 hearing-impairedlisteners. The forward masker level required to mask a fixed low-level, 4000-Hz signal wasmeasured as a function of the masker‚Äďsignal interval using a masker frequency of either 2200 or4000 Hz. These plots are known as temporal masking curves ÕĎTMCsÕí. BM response functionsderived from the TMCs showed a systematic reduction in gain with degree of hearing loss. Contraryto current thinking, however, no clear relationship was found between maximum compression andabsolute threshold.
2004 Acoustical Society of America. ÕďDOI: 10.1121/1.1675812ÕĒ
PACS numbers: 43.66.Dc, 43.66.Mk, 43.66.Sr ÕďNFVÕĒ
I. INTRODUCTION
erence to derive the BM response to a tone at CF. Oxenhamand Plack ÕĎ1997Õí measured the forward masker level re-
Cochlear hearing loss is associated with an increase in
quired to mask a brief signal as a function of the level of the
absolute threshold, an abnormally rapid growth in loudness
signal ÕĎreferred to here as the growth of masking, or GOM,
with level, and a loss of frequency selectivity ÕĎsee Moore,
techniqueÕí. When the masker was an octave below the signal
1995 for a reviewÕí. These characteristics may result from
frequency of 2000 or 6000 Hz, a given change in signal level
dysfunction of the outer hair cells ÕĎOHCsÕí in the organ of
required a much smaller change in masker level for the sig-
Corti. The OHCs are thought to be involved in an ‚Äė‚Äėactive‚Äô‚Äô
nal to remain at threshold. This is thought to be because the
mechanism that effectively applies gain to stimulation at fre-
response to the signal is compressive and the response to the
quencies close to the characteristic frequency ÕĎCFÕí of each
masker is linear. Indeed, the shallow off-frequency masking
place on the basilar membrane ÕĎBMÕí ÕĎsee Yates, 1995 for a
function ÕĎmasker level plotted against signal levelÕí is an es-
reviewÕí. The gain is greatest at low stimulation levels, and
timate of the BM response function to a tone at CF.
decreases with increasing level. This frequency- and level-
A different technique was developed by Nelson
et al.
dependent gain sharpens BM tuning at low to moderate lev-
ÕĎ2001Õí. The signal was fixed at a level just above absolute
els, and also results in a highly
compressive BM response to
threshold. The masker level required to mask the signal was
mid- and possibly high-level tones close to CF ÕĎRobles
et al. ,
measured as a function of the masker‚Äďsignal interval to pro-
1986; Ruggero
et al. , 1997Õí. Measurements of BM vibration
duce a
temporal masking curve ÕĎTMCÕí. For an
off -frequency
in nonhuman mammals have confirmed that interfering with
masker, the TMC is assumed to reflect the decay with time of
the function of the OHCs, for example by furosemide injec-
the internal effect of the masker: As the masker‚Äďsignal inter-
tion ÕĎRuggero and Rich, 1991Õí, results in a steeper, more
val is increased, the masker level has to increase to compen-
sate for the decay. For an
on -frequency masker, the TMC
Psychophysical techniques based on forward masking
reflects the decay of masking,
and the compression applied
have been used to estimate the growth of response of the
to the masker: If the response is compressive, a larger change
human BM. Forward masking is used to avoid simultaneous
in physical masker level will be required to produce a given
interactions on the BM ÕĎe.g., suppressionÕí that complicate
change in BM excitation. It follows that an on-frequency
the interpretation of the results ÕĎOxenham and Plack, 1997Õí.
TMC that is steep compared to the off-frequency TMC is
Most of these techniques have involved comparisons of the
indicative of compression. It is also possible to derive re-
effects of maskers at and below the signal frequency. Since
sponse functions from TMC data. It is assumed that, for a
the BM response to a masker well below CF is linear, the
given masker‚Äďsignal interval, the BM excitation level at the
off-frequency masking function can be used as a linear ref-
signal place in response to the masker is a constant at thresh-old, regardless of the masker frequency. For a given masker‚Äď
signal interval, the level of the off-frequency masker re-
J. Acoust. Soc. Am.
115 (4), April 2004
quired is an estimate of the BM excitation required at the
35 dB. However, the results may have been compromised by
signal place ÕĎgive or take an additive constant on a dB scaleÕí.
the fact that Moore
et al. did not use high-pass noise to mask
Therefore, a plot of the on-frequency masker level ÕĎinput
spread of excitation ÕĎsee aboveÕí. The compression exponents
levelÕí against the off-frequency masker level ÕĎoutput levelÕí is
estimated by Moore
et al. for normal-hearing listeners were
an estimate of the BM response function for the on-
at least twice as great as those from GOM studies that in-
cluded the high-pass noise ÕĎNelson
et al. , 2001; Oxenham
The results from the GOM and TMC studies for normal-
and Plack, 1997Õí. Hicks and Bacon ÕĎ1999aÕí, again using the
hearing listeners at high frequencies are broadly consistent
GOM technique without high-pass noise, found that mild
with the rate of growth of BM velocity at high CFs, as mea-
temporary hearing loss induced by aspirin was associated
sured in other mammals ÕĎLopez-Poveda
et al. , 2003; Nelson
with a change in slope, consistent with a reduction in com-
et al. , 2001; Oxenham and Plack, 1997; Plack and Drga,
pression. Two listeners with mild permanent sensorineural
2003Õí. Most GOM and TMC studies report compression ex-
hearing loss showed similar effects. In a recent study mea-
ponents ÕĎthe slopes of the response functions on dB/dB co-
suring GOM for
simultaneous notched-noise maskers, Baker
ordinatesÕí in the range 0.15‚Äď0.3. This corresponds to com-
and Rosen ÕĎ2002Õí reported a reduction in gain and compres-
pression ratios ÕĎthe inverses of the compression exponentsÕí
sion for a listener with a hearing loss of only 20 dB. How-
of between 6.7:1 and 3.3:1. Furthermore, the shapes of the
ever, compression estimates were generally quite low in this
estimated response functions, with linear low-level regions
study, possibly because of suppressive interactions between
and compressive midlevel regions, are also consistent with
the physiology, suggesting that both behavioral techniques
In the present study, the TMC technique was used to
measure cochlear processes. However, there are two good
estimate the BM response to a tone at CF for listeners with a
reasons for favoring the TMC technique. As signal level is
range of impairments, from no impairment to mild to mod-
increased in the GOM technique, the peak of the traveling
erate. The aim was to determine how the shape of the re-
wave produced by a high-frequency signal will shift basally
sponse function changes with severity of hearing loss, and to
on the BM ÕĎMcFadden, 1986Õí. This means that the GOM
test the hypothesis that mild hearing loss is associated with a
technique is probably not measuring the response of a single
place on the BM, but rather the growth of the peak of thetraveling wave with level. In addition, as signal level is in-
II. METHOD
creased excitation will spread to higher CFs. To prevent lis-teners using information from the high-frequency side of the
A. Listeners
excitation pattern ÕĎwhere the response growth is much more
Sixteen normal-hearing listeners and nine listeners with
linear than at the peakÕí, a high-pass noise needs to be added
mild to moderate hearing impairment participated in the
to the stimulus ÕĎOxenham and Plack, 1997Õí. Nelson
et al.
study. Normal-hearing listeners ÕĎten females and six males,
ÕĎ2001Õí demonstrated that GOM curves in the absence of a
aged 19‚Äď37 years oldÕí were mostly students from the Uni-
high-pass noise exhibit about half the compression of GOM
versity of Essex. All had normal audiogram thresholds
curves in the presence of the noise. This finding is consistent
ÕĎwithin 15 dB ANSI, 1996Õí in octave steps from 250‚Äď8000
with the greater compression exponents measured in GOM
studies that did not include high-pass noise ÕĎHicks and Ba-
Hearing-impaired listeners ÕĎfive females and four
con, 1999b; Moore
et al. , 1999; Plack and Oxenham, 2000Õí.
malesÕí, were aged 54 ‚Äď 68 years old, except for listener RD,
Selection of the appropriate noise level is problematic, espe-
who was 42 years old. Hearing-impaired listeners reported
cially for impaired listeners. The TMC technique avoids both
the onset of hearing difficulties between 2 and 15 years ago
these complications. In the TMC technique the signal is fixed
and had mild-to-moderate amounts of hearing loss. This was
at a low level, and hence presumably causes excitation above
most likely sensorineural hearing loss since it came on
detection threshold over a fixed, relatively small, region of
gradually and was unrelated to any acute trauma or known
the BM. The region of the BM measured does not change
disease. It was most likely age related, except for listeners
with masker level, and since the spread of excitation is lim-
PJ, SG, and RD, who reported repeated exposure to noisy
ited there is no need for a high-pass noise.
environments when younger. RD also had a family history of
Both the GOM and TMC techniques have been used to
hearing loss. On average, audiogram levels for the hearing-
estimate the BM response for listeners with cochlear hearing
impaired group were higher than laboratory norms for nor-
loss. The results suggest that a hearing loss of greater than
mal hearing by 20, 30, and 38 dB at 1000, 2000, and 4000
about 50 dB is associated with an almost linear BM response
Hz, respectively. Except for ED, the thresholds at lower fre-
ÕĎNelson
et al. , 2001; Oxenham and Plack, 1997Õí: The slopes
quencies were normal or near normal, suggesting that the
of the GOM functions and TMCs do not vary with masker
impairments did not have a substantial conductive compo-
frequency in these cases ÕĎproviding support for the conten-
nent. Although bone-conduction tests were not performed,
tion that the psychophysical techniques measure cochlear
the close spacing of the on- and off-frequency TMCs for the
processesÕí. For ears with less severe losses, the results are
impaired listeners is also inconsistent with a conductive loss
mixed. Moore
et al. ÕĎ1999Õí used the ratio of the slopes of
ÕĎsee Sec. IV AÕí. RD had borderline normal hearing at 4000
off- and on-frequency GOM functions as an estimate of com-
Hz, but elevated thresholds ÕĎ35‚Äď 42-dB lossÕí at 6000 and
pression. They found that the compression exponent only
8000 Hz. His absolute threshold for the brief 4000-Hz signal
began to increase markedly as hearing loss increased above
in the experiment was 5 dB above the highest absolute
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
TABLE I. Absolute thresholds, stimulus parameters, and estimated BM response parameters for normal-hearing ÕĎupperÕí and hearing-impaired ÕĎlowerÕílisteners, ordered according to the absolute threshold for the signal. Listeners were tested in their right ears unless indicated otherwise. Gain estimates are onlyincluded when the low-level portion of the response function is defined by at least two points. Compression and gain could not be sensibly estimated for RGand ES due to the variability of their data. Values marked with asterisks are from response functions generated by interpolation of the off-frequency TMCs.
threshold for the normal-hearing group. Audiogram thresh-
hearing listeners and from 33‚Äď71-dB SPL for hearing-
olds, and absolute thresholds for the signal used in the ex-
impaired listeners. Masker level was varied trial by trial.
A low-level notched noise was gated on and off with the
All of the listeners were naive except for EK, IY, PP, and
masker. This was intended as a temporal cue to help reduce
VD. The normal-hearing listeners, except for AC, CN, ES,
possible confusion effects ÕĎNeff, 1986Õí and not as a source of
and RB, had 4 ‚Äď 8 h practice in pilot studies for the current
masking. The noise was white except for a notch at the signal
experiment. AC, CN, ES, and RB, and all of the hearing-
frequency ÕĎfilter cutoffs at 0.883
f s and 1.117
f s , with 90-
impaired listeners received 1‚Äď2 h practice in blocks used to
dB/oct filter slopeÕí. For normal-hearing listeners and listener
determine parameters for them in the main experiment.
RD, the spectrum level in the passband was set 30 dB below
There were no systematic improvements in thresholds in the
the signal level ÕĎi.e., 20 dB below signal absolute thresholdÕí.
experimental sessions. Listeners were paid £5 per hour for
For the remaining hearing-impaired listeners the spectrum
level was set to either 40, 50, or 60 dB below the signal levelso that it fell in the range Ō™5 to 11 dB. For most hearing-impaired listeners, setting the spectrum level to 30 dB below
B. Stimuli and equipment
the signal meant having spectrum levels almost up to 40 dB,
The experiment involved forward masking of tonal sig-
resulting in masking due to the noise. Setting the spectrum
nals by tonal maskers. The signal had a frequency of
f
level to a level between Ō™5 and 11 dB was practical in that
Ō≠4000 Hz and an absolute duration of 8 ms ÕĎ4-ms raised-
hearing-impaired listeners could make use of temporal infor-
cosine ramps, 0-ms steady stateÕí. The masker had a fre-
mation at lower frequencies without the noise contributing to
masking at 4000 Hz. As described above, most of the
ration of 104 ms ÕĎ2-ms raised-cosine ramps, 100-ms steady
hearing-impaired listeners had elevated thresholds at 4000
stateÕí. Silent masker‚Äďsignal intervals ÕĎmasker envelope off-
Hz but normal or near-normal absolute thresholds for fre-
set to signal envelope onsetÕí ranged from 0‚Äď100 ms in steps
quencies below 2000 Hz. Notched-noise levels for each in-
of 5 or 10 ms, with the set of intervals used dependent on
each listener’s performance. The signal level was set to 10
The experiment was run using custom-made software on
dB SL, which ranged from 15‚Äď27-dB SPL for normal-
a PC workstation located outside a double-walled sound-
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
attenuating booth. Stimuli were digitally generated and were
except that signal level was varied using a two-down, one-up
produced using an RME Digi96/8 PAD 24-bit soundcard set
at a clocking rate of 48 000 Hz. The soundcard includes anantialiasing filter. The headphone output of the soundcard
III. RESULTS AND ANALYSES
was fed via a patch panel in the sound-booth wall, withoutfiltering or amplification, to Sennheiser HD 580 circumaural
A. Temporal masking curves
headphones. Each listener sat in the booth and decisions
Individual TMCs are presented in Fig. 1 for normal-
were recorded via a computer keyboard. Listeners viewed a
hearing listeners and in Fig. 2 for hearing-impaired listeners.
computer monitor through a window in the sound booth.
In general, on-frequency TMCs ÕĎtrianglesÕí are steeper, in part
Lights on the monitor display flashed on and off concurrently
or in whole, than the accompanying off-frequency TMCs.
with each stimulus presentation and provided feedback at the
Assuming the BM response to off-frequency maskers is lin-
ear at the signal place, then steeper portions of the on-frequency TMC indicate a compressive response to the on-frequency masker. Such results were found for both the
C. Procedure
normal-hearing and the hearing-impaired groups.
All stimuli were presented monaurally. Normal-hearing
For three impaired ears, RC(
l ), MB, and PJ, it was not
listeners were tested in their right ear. Hearing-impaired lis-
possible to reliably measure on-frequency thresholds at the
teners were tested in their right ear, or in both left and right
longest masker‚Äďsignal interval. In two successive runs, they
ears if their audiogram thresholds at 4000 Hz differed across
consistently detected the signal when the 4000-Hz masker
ears by more than 10 dB. Those tested in both ears wore an
was at 100 dB SPL. The equipment clipped at the next higher
earplug in their contralateral ear to prevent the possibility of
level in the adaptive track ÕĎ102 dB SPLÕí, so the data point
for the longest masker‚Äďsignal interval presented in Fig. 2 for
The experiment used a two-interval, forced-choice adap-
these three listeners was set at 100 dB SPL, and in each case
tive tracking procedure with the interstimulus interval set to
this value was used ÕĎwhen requiredÕí in the analyses de-
500 ms. The signal level was fixed at 10 dB SL and the
scribed below. Limiting the level in this way resulted in
un-
masker level was varied adaptively using a two-up, one-
derestimates of their thresholds and consequently, based on
down rule to obtain the masker level needed to achieve 70.7
linear extrapolation of their off-frequency TMCs, underesti-
percent correct ÕĎLevitt, 1971Õí. The masker frequency and
mates of the amount of compression ÕĎoverestimates of the
masker‚Äďsignal interval were fixed in any given block of tri-
compression exponentsÕí. For several impaired ears, the off-
als. For normal-hearing listeners, the initial masker level was
frequency masker levels at the longer intervals also clipped
set to 0 dB SPL. The step size of the adaptive track was 8 dB
at some stage during the adaptive track on every replication,
for the first four turnpoints and 2 dB for 12 subsequent turn-
and these measurements were aborted Õďsee MB, PJ, DJ(
l ),
points. Data for listeners RD and BH were collected using
and BH in Fig. 2ÕĒ. However, unlike the on-frequency mea-
these settings, but we found it was desirable to slightly
surements for the three ears described above, the signal was
modify the procedure for the rest of the hearing-impaired
only
occasionally detected with the masker at the clipping
listeners, due to limitations in the equipment’s maximum
threshold ÕĎthe adaptive track touched the clipping point be-
output ÕĎ102-dB SPL rmsÕí. The modifications were that the
fore retreatingÕí. It may be assumed that the ‚Äė‚Äėtrue‚Äô‚Äô off-
initial masker level was set to 20‚Äď 40 dB below estimated
frequency masker level for these missing points lies some-
threshold, and the step size was 4 dB for the first four turn-
points and 2 dB for the 12 subsequent turnpoints. For all
A surprising aspect of the data is that the slopes of the
listeners, the mean of the last 12 turnpoints was taken as the
off -frequency TMCs appear to be different for the normal-
threshold estimate for each block of trials. If the standard
hearing and hearing-impaired listeners. Two analyses were
deviation of the turnpoints was greater than 6 dB the esti-
conducted to illustrate and quantify this difference. First, the
mate was discarded and the block was later repeated. Data
slopes of the straight lines connecting consecutive points on
were also discarded and repeated if possible for any blocks in
the off-frequency TMCs were calculated for each listener.
which the masker clipped more than twice at levels above
The slope values for all the listeners were then combined and
ordered by masker‚Äďsignal interval or by masker level. The
Listeners ran blocks of trials lasting 2‚Äď 4 min per block
upper panels of Fig. 3 show running averages of these val-
and spent 15‚Äď 60 min in the sound booth at any one time,
ues, plotted against running averages of masker‚Äďsignal inter-
taking breaks as needed. A replication consisted of a com-
val ÕĎupper leftÕí and masker level ÕĎupper rightÕí. The running
plete run of 10‚Äď20 blocks per listener, depending on the
averages were calculated separately for the normal-hearing
range of the masker‚Äďsignal interval at each
f m , which was
and hearing-impaired groups. The graphs indicate that there
determined during each listener’s practice trials. The order of
are some trends in the data. First, the off-frequency TMC
blocks was randomized across masker‚Äďsignal interval and
f m
slopes for the normal-hearing group show a tendency to de-
until all blocks in a replication had been completed. Unless
crease with increasing masker‚Äďsignal interval. The correla-
otherwise indicated, the mean threshold across four replica-
tion between masker‚Äďsignal interval and slope is significant
tions was taken as the threshold estimate for each combina-
for the normal-hearing group (
r Ō≠Ō™0.231,
n Ō≠106,
p
tion of masker‚Äďsignal interval and
f
0.017). On the other hand, there is little variation in slope
for the signal were measured using the same basic procedure,
with masker‚Äďsignal interval for the hearing-impaired group,
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
FIG. 1. TMCs for normal-hearing listeners, showing mean masker level at threshold as a function of masker‚Äďsignal interval for on-frequency ÕĎ4000-HzÕímaskers ÕĎtrianglesÕí and off-frequency ÕĎ2200-HzÕí maskers ÕĎcirclesÕí.
and the correlation is not significant (
r Ō≠Ō™0.155,
n Ō≠48,
p
absolute threshold and off-frequency TMC slope at a specific
Ō≠0.293). Second, the off-frequency TMC slopes for the
masker‚Äďsignal interval and at a specific masker level.
normal-hearing group show a tendency to decrease with in-
Second-order polynomials were fit to the off-frequency
creasing masker level, and the correlation between level and
TMCs for each listener, and the slopes of the functions cal-
slope is significant (
r Ō≠Ō™0.271,
n Ō≠106,
p Ō≠0.005). The
culated ÕĎanalyticallyÕí at a masker‚Äďsignal interval of 30 ms
correlation between level and slope is not significant for the
and, separately, at a masker level of 85 dB SPL. A slope
hearing-impaired group (
r Ō≠Ō™0.159,
n Ō≠48,
p Ō≠0.282), al-
value was only included when the masker‚Äďsignal interval
though the range of levels for this group is much less than
ÕĎeither 30 ms, or the calculated masker‚Äďsignal interval for an
85-dB SPL maskerÕí fell within the range of intervals tested
A second analysis investigated the relationship between
for that listener. The calculated slopes are shown in the lower
FIG. 2. As Fig. 1, except showing TMCs for hearing-impaired listeners.
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
FIG. 3. The upper panels show the slopes of the2200-Hz TMCs, collapsed across listeners and plottedas running averages over 20 consecutive points. Theslopes are shown as a function of masker‚Äďsignal inter-val ÕĎupper leftÕí and masker level ÕĎupper rightÕí. Thelower panels show scatterplots of 2200-Hz TMC slopeagainst signal absolute threshold. The slopes were de-rived by fitting second-order polynomials to the TMCdata for each listener. The slopes at a masker‚Äďsignalinterval of 30 ms ÕĎlower leftÕí and at a masker level of85 dB SPL ÕĎlower rightÕí were calculated from the fittedfunctions. The lines show linear regression fits, withequations and
R 2 values displayed on the figure.
two panels of Fig. 3, plotted against the absolute thresholds
signal and the masker at threshold should have been unaf-
for the signal. There is a significant negative correlation be-
fected by the hearing loss,
if there was no additional source
tween absolute threshold and slope at a 30-ms masker‚Äďsignal
of masking for the normal-hearing listeners.
interval (
r Ō≠Ō™0.443,
n Ō≠27,
p Ō≠0.021), but no significant
At a masker‚Äďsignal interval of 10 ms, the mean differ-
correlation between absolute threshold and slope at an 85-dB
ence between signal level and on-frequency masker level is
SPL masker level (
r Ō≠Ō™0.334,
n Ō≠22,
p Ō≠0.129). In sum-
Ō™1.7 dB for the normal-hearing group and 2.0 dB for the
mary, the results show that at short masker‚Äďsignal intervals
hearing-impaired group. At an interval of 20 ms, the values
the off-frequency TMC slopes are shallower for the hearing-
are 6.1 and 5.5 dB, respectively. So, although there is a sug-
impaired listeners than for the normal-hearing listeners.
gestion that the noise may have contributed to masking at the
However, the difference may be related to the fact that the
10-ms gap, there appears to have been no effect at a 20-ms
masker thresholds were at a higher level for the hearing-
gap, for which there is a clear difference in off-frequency
impaired listeners. There appears to be little difference in
slope between the normal-hearing and hearing-impairedgroups when the TMCs are matched for masker level.
B. Response functions
It is conceivable that the results for the shorter masker‚Äď
signal intervals were influenced by the notched noise that
Following the approach of Nelson
et al. ÕĎ2001Õí, TMCs
was presented as a cue to the offset of the masker. The noise
for each listener were converted into BM response functions
level was generally higher relative to the signal level for the
by plotting the off-frequency masker threshold against on-
normal-hearing group compared to the hearing-impaired
frequency masker threshold, paired according to masker‚Äď
group ÕĎsee Table IÕí. Although in all conditions the signal was
signal interval. For several hearing-impaired ears, off-
clearly above threshold in the presence of the noise alone, if
frequency masker levels were not available at all the
the noise had contributed to the masking of the signal at the
masker‚Äďsignal intervals for which on-frequency masker lev-
short masker‚Äďsignal intervals, then the masker level at
els were measured. For these ears, it was assumed that the
threshold may have been artificially lowered for the normal-
slopes of the off-frequency TMCs do not change signifi-
hearing group at the short intervals ÕĎboth on and off fre-
cantly with masker‚Äďsignal interval. Given that there was no
quencyÕí leading to an increase in TMC slope. One way to
significant correlation between masker‚Äďsignal interval and
test this hypothesis is to examine the masker levels at thresh-
slope for the hearing-impaired listeners ÕĎsee Sec. III AÕí, this
old for the on-frequency masker. It is assumed that, for a
was felt to be a reasonable assumption. For those masker‚Äď
given masker‚Äďsignal interval at threshold, the ratio of BM
signal intervals missing a measured off-frequency masker
velocity in response to the signal to BM velocity in response
level, an off-frequency masker level was generated by inter-
to the masker is constant. Furthermore, the BM response to a
polation, using a linear fit to the off-frequency data.
low-level on-frequency masker should have been affected in
The response functions for normal-hearing listeners and
a similar way as the response to the 10-dB SL signal by any
for hearing-impaired listeners are plotted in Figs. 4 and 5,
attenuation ÕĎor loss of gainÕí resulting from the hearing im-
respectively. These show the growth of level with masker‚Äď
pairment: If the hearing impairment resulted in the response
signal interval for the off-frequency masker relative to the
to the signal being attenuated by
x dB, then the response to
growth for the on-frequency masker. Open symbols indicate
the masker should also have been attenuated by
x dB. It fol-
those points that were generated by interpolating the off-
lows that the difference between the
physical levels of the
frequency TMCs. The positive diagonal (
y Ō≠
x ) is included
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
FIG. 4. Estimated response functions for normal-hearing listeners, showing the 2200-Hz masker level at threshold plotted against the 4000-Hz masker levelat threshold, paired according to masker‚Äďsignal interval. The positive diagonal ÕĎstraight lineÕí indicates the expected response of a passive, linear system. Thevertical line indicates signal absolute threshold (
re : the
x axisÕí. The kinked line shows the piecewise linear fit ÕĎsee the text for detailsÕí.
in Figs. 4 and 5 to indicate the expected response of a linear
the response functions with slope less than unity ÕĎcompres-
system with 0-dB gain ÕĎsee belowÕí. Masker‚Äďsignal intervals
over which the on-frequency TMC is parallel to the off-
Most of the normal-hearing listeners show evidence of
frequency TMC translate to portions of the response func-
compression, having shallow portions in their response func-
tions with slope unity, implying a linear BM response.
tions in Fig. 4, although this is not so clear for listeners RG
Masker‚Äďsignal intervals over which the on-frequency TMC
and ES, whose data are variable. Most of the hearing-
is steeper than the off-frequency TMC translate to portions of
impaired listeners also show evidence of compression, as
FIG. 5. As Fig. 4, except for hearing-impaired listeners. Open circles show points on the response functions that were estimated by interpolation of theoff-frequency data, using straight-line fits to the off-frequency TMCs. Left and right ears are indicated by ÕĎ
l Õí and ÕĎ
r Õí, respectively.
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
seen in the shallow portions of their response functions in
maskerÕí are both expressed in dB. The function was fit to the
Fig. 5. Indeed, many of the hearing-impaired response func-
data using the
fminsearch function in MATLAB to satisfy a
tions appear at least as compressive as those seen for normal-
least-squares regression criterion. The slopes of the lower
hearing listeners, although the compression extends over a
and upper sections were fixed at unity ÕĎlinear responseÕí,
smaller range of levels for the former. This suggests that BM
while the slope of the middle section ÕĎ
c Õí and the breakpoints
compression is present even when sensitivity is much re-
(BP1 and BP2) were varied by the fitting procedure. The
duced compared to normal-hearing listeners. Some normal-
only constraint on the fitting procedure was that the compres-
hearing listeners ÕĎVD,PP,IG,NBÕí show evidence of a return
sion exponent
c was not allowed to be negative; otherwise,
to linearity at the highest masker levels, with on-frequency
the parameters were allowed to vary freely. In some cases
TMCs becoming shallow at long masker-signal intervals, and
either the lower breakpoint or the upper breakpoint estimated
hence the response functions becoming steeper at high lev-
by the fitting procedure was beyond the range of the data, so
els. This is not the case in general for hearing-impaired lis-
that effectively the data were fit using a reduced number of
teners. If such a pattern is to be found with hearing-impaired
parameters. The fits were first made to the response function
listeners, it must occur at very high levels ÕĎŌĺ100 dB SPLÕí.
data without any off-frequency interpolation ÕĎjust the filledsymbols in Figs. 4 and 5Õí, and then separately including theinterpolated data ÕĎi.e., filled
and open symbolsÕí. Fits were
C. Estimates of gain and compression
not included when there were less than five points on the
The maximum gain of the active mechanism can be es-
response function Õďi.e., for DJ(
r ), MB, RC(
l ), PJ, and
timated using the horizontal distance between the left-most,
DJ(
l ), without interpolated dataÕĒ. The lines fit to the re-
linear portion of a response function and the positive diago-
sponse functions including the interpolated data are shown in
nal. This is an estimate of the difference between the levels
Figs. 4 and 5. The fits for listeners RG and ES had high rms
of a 4000-Hz masker and a 2200-Hz masker required to pro-
errors ÕĎ9 and 7 dB, respectivelyÕí and are not included in the
duce the same BM response. If it is assumed that no gain is
figures or in subsequent analyses. For the other listeners,
applied to the off-frequency masker ÕĎso that the positive di-
however, the fits generally provide a good description of the
agonal approximates the off-frequency response even at low
input levelsÕí, then this estimate is equivalent to the difference
Scatterplots of maximum gain against signal absolute
in the BM response between a low-level masker at 4000 Hz
threshold and compression against signal absolute threshold
and a low-level masker at 2200 Hz. This measure of gain is
are shown in Fig. 6. Gain and compression estimates were
similar to that used by others, e.g., Ruggero
et al. ÕĎ1997Õí, in
taken from the three-section fits. A gain estimate was in-
that it estimates the difference between the active BM re-
cluded only if there were at least two points on the response
sponse and the maximum passive response at signal place.
function that were below BP1 . The results are shown sepa-
The data of Ruggero
et al. suggest that the off-frequency
rately for fits to the response-function data without interpo-
response to a tone at 0.55ŌęCF is slightly less ÕĎby 2‚Äď 4 dBÕí
lation ÕĎleft-hand panelsÕí and for fits to the data including the
than that of the maximum passive response. Since the pas-
interpolated off-frequency values ÕĎright-hand panelsÕí. The
sive response has broad tuning, it is assumed that any dis-
fits that involved interpolated values are shown as open sym-
crepancy between the off-frequency response and the maxi-
bols. Data from both normal-hearing and hearing-impaired
mum passive response is approximately constant across
listeners are presented together in each graph. A straight-line
individuals. If so, this should not affect any correlation of
fit to the scatterplot data, and the squared correlation coeffi-
gain with absolute threshold in our analyses below.
cient, are also displayed. Individual gain and compression
To help quantify gain and compression, a three-section
fit was applied to each listener’s BM response function
As shown by Fig. 6, the estimated gain of the cochlear
ÕĎLopez-Poveda
et al. , 2003; Yasin and Plack, 2003Õí. The
amplifier decreases systematically with increasing hearing
function comprised a linear low-level region ÕďEq. ÕĎ1ÕíÕĒ, a
loss. The correlation is statistically significant both for the
compressive mid-level region ÕďEq. ÕĎ2ÕíÕĒ, and a linear high-
data without interpolation (
r Ō≠Ō™0.930,
n Ō≠16,
p ŌĹ0.0005;
level region ÕďEq. ÕĎ3ÕíÕĒ. The three sections were joined by two
slopeŌ≠Ō™0.736 dB/dBÕí and for the data with interpolation
breakpoints, a lower breakpoint (BP1) joining sections 1 and
(
r Ō≠Ō™0.951,
n Ō≠22,
p ŌĹ0.0005; slopeŌ≠Ō™0.647 dB/dBÕí.
2, and an upper breakpoint (BP2) joining sections 2 and 3.
Figure 6 also shows that, although there is a range of com-
The equations for the three sections are given by
pression values for both normal-hearing listeners ÕĎleft half ofthe dataÕí and hearing-impaired listeners ÕĎright half of the
dataÕí, there is little correlation between compression and ab-solute threshold. The correlations are not significant either
for the data without interpolation (
r Ō≠0.101,
n Ō≠21,
p
Ō≠0.662) or for the data with interpolation (
r Ō≠0.284,
n
Ō≠26,
p Ō≠0.159). For some of the more impaired ears the
compressive region is defined by only a couple of points
where
G is the gain ÕĎdBÕí,
c is the slope of the compressive
ÕĎoften interpolatedÕí. However, the ears with milder impair-
region ÕĎdB/dBÕí or the compression exponent,
k Ō≠
ments ÕďRD, JC, ED(
l ), SG, DJ(
r ), RC(
r ), and ED(
r )] have
BP2(
c Ō™1)Ō©
k 1 .
L in input level, level of 4000-Hz
well-defined shallow sections in their response functions and
compression exponents within the normal range ÕĎ0.29, 0.26,
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
FIG. 6. Scatterplots of maximum gain against signalabsolute threshold ÕĎupper panelsÕí, and response-function slope against signal absolute threshold ÕĎlowerpanelsÕí, at 4000 Hz. The left-hand panels show the re-sults for response functions generated without interpo-lation. The right-hand panels include the results for re-sponse functions that were generated using interpolatedoff-frequency masker levels ÕĎindicated by the opensymbolsÕí. Gain estimates are only included when thelow-level portion of the response function is defined byat least two points ÕĎsee Table IÕí.
0.15, 0.29, 0.21, 0.28, and 0.37, respectively, for the interpo-
ponent, should all be unaffected by the hearing loss, and
lated dataÕí. The mean compression exponent for the interpo-
hence independent of the degree of hearing loss. For an ear
lated data is 0.20 for the normal-hearing listeners and 0.26
with purely OHC dysfunction, however, the maximum gain
should be strongly related to the absolute threshold. Specifi-
There is an issue regarding whether the three-section
cally, a plot of gain ÕĎin dBÕí against absolute threshold ÕĎin dBÕí
straight-line fits provide an accurate characterization of the
should be a straight line with a slope of Ō™1. Turning down
response functions. Third-order polynomials have been used
the gain by 10 dB should result in an increase in absolute
previously to fit response functions ÕĎNelson
et al. , 2001;
Plack and Drga, 2003Õí. Such fits were attempted on the
If the hearing loss experienced by our listeners were
present data but gave very inconsistent results, with negative
simply a matter of non-frequency-specific attenuation
prior
slopes in some cases. It was felt that the three-section fits,
to the BM, as might result from conductive hearing loss, then
although not ideal, do capture the main features of the re-
both on- and off-frequency TMCs would increase by the
sponse functions for the normal-hearing and hearing-
same amount and, consequently, the estimated maximum
impaired listeners: The reduction in gain with hearing loss
gain would remain unchanged as a function of hearing loss.
ÕĎalso reflected in the vertical spacing between the on- and
Similarly, pure IHC loss ÕĎpost-BM attenuationÕí should result
off-frequency TMCsÕí, and the preservation of a shallow
in no change in the estimated maximum gain ÕĎalthough it is
slope in the response function ÕĎcompressionÕí, even for ears
only possible to measure the lower breakpoint on the re-
sponse function if it is above absolute thresholdÕí. These pre-dictions do not seem to describe the present data. The strong
IV. DISCUSSION
relation between maximum gain and absolute threshold ÕĎFig.
6Õí suggests that the hearing loss in the impaired listeners
A. Consequences of inner and outer hair cell
tested here was mainly the result of OHC dysfunction. Off-
dysfunction
frequency TMCs were somewhat higher in level for the
An elevation in absolute threshold may result from a
hearing-impaired compared to the normal-hearing group, but
dysfunction of the inner hair cells ÕĎIHCsÕí or of the OHCs
it was the general increase in level for the on-frequency
ÕĎsee Moore, 1995Õí. IHC dysfunction reduces the efficiency of
TMCs relative to the off-frequency TMCs that characterized
transduction of BM vibration ÕĎhence reducing sensitivityÕí but
the impaired group, again consistent with OHC damage. In-
is not thought to affect the mechanical properties of the BM
cluding the interpolated data, the plot of gain against abso-
itself ÕĎLiberman
et al. , 1986Õí. OHC dysfunction affects the
lute threshold has a slope of Ō™0.65, which suggests that most
response of the BM, but not the transduction process
per se .
of the threshold elevation can be attributed to a reduction in
Now, imagine a situation in which a cochlea has damage to
gain. The fact that the slope was not Ō™1 suggests that there
the IHCs only. For a given input level, the response proper-
may have been some IHC dysfunction among the listeners
ties of the BM should be
identical to that for a healthy ear.
ÕĎcontributing to perhaps 35% of the threshold elevation for
According to the measures described earlier, the maximum
those ears for which the gain was measurableÕí. Indeed, from
gain of the active mechanism, the input level at the first
the results of other studies examining the relative proportions
breakpoint in the response function, and the compression ex-
of IHC and OHC hearing loss, it would be surprising if there
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
FIG. 7. BM response functions for normal-hearing andhearing-impaired listeners. The normal response func-tion is an average function generated from the presentdata ÕĎsee the text for detailsÕí. In panels ÕĎAÕí to ÕĎCÕí theresponse functions for the hearing-impaired listenersare hypothetical. In panel ÕĎAÕí, the gain for hearing-impaired listeners is reduced equally at all input levelsup to the passive response. In panel ÕĎBÕí, the reductionin gain is greatest at low input levels, with a diminish-ing reduction as level is increased. In panel ÕĎCÕí, thegain is reduced at low input levels, but unaffected athigh input levels. Panel ÕĎDÕí shows average responsefunctions,
impaired listeners, generated from the present data ÕĎseethe text for detailsÕí. In panel ÕĎDÕí, the thin vertical linesshow the average absolute thresholds for the signal, andthe thin horizontal lines the associated response levels,for the normal-hearing and hearing-impaired listenersused to generate the response functions.
were not some evidence of IHC dysfunction ÕĎLopez-Poveda
associated with a reduction in the gain at the
lower input
et al. , 2004; Moore and Glasberg, 1997; Moore
et al. , 1999Õí.
levels only , and not across the whole range of input levels
IHC dysfunction will raise the output level on the BM re-
that are affected by the active mechanism. This is why the
sponse function that corresponds to absolute threshold, and
slope of the compressive part of the response function did
may explain why the low-level linear segment on the re-
not vary significantly with absolute threshold ÕĎsee Fig. 6Õí.
sponse function is generally shorter for the hearing-impaired
In this respect, the present data do not appear to be con-
listeners than for the normal-hearing listeners ÕĎsee Figs. 4
sistent with some physiological models of hearing loss. The
and 5, and Sec. IV BÕí. However, given that OHC dysfunction
BM response function of a chinchilla injected 40 min previ-
was probably the main cause of the reduction in sensitivity,
ously with furosemide showed a reduction in gain at all lev-
what do the present results tell us about the effects of OHC
els ÕĎRuggero and Rich, 1991Õí, more similar to option ÕĎAÕí in
Fig. 7. As with the present data, however, BM compressionwas relatively unaffected by this mild hearing loss. Muru-
B. Effects of outer hair cell dysfunction on the BM
gasu and Russell ÕĎ1995Õí report guinea pig displacement mea-
response
surements during salicylate perfusion. Some of their re-sponse functions show a reduction in gain at all levels, but
To aid the discussion of the effects of OHC dysfunction
some show an effect only at low levels, similar to the func-
on the shape of the BM response function, three different
tions reported here. Recent auditory-nerve recordings from
hypothetical scenarios are illustrated in Fig. 7. Each panel of
cats with noise-induced hearing loss also seem consistent
the figure shows the normal response function ÕĎcontinuous
with the present data ÕĎHeinz
et al. , in pressÕí. For mild hear-
black line, generated from the present data as described be-
ing loss, a measure of the total auditory-nerve activity
lowÕí, the passive response function with no active mecha-
showed a reduction in response at low levels but not at high
nism ÕĎthin dotted lineÕí, and a hypothetical response for a
levels, consistent with a reduction in gain at low levels only.
listener with mild hearing loss ÕĎalternate dashes and dotsÕí. In
The thin vertical and horizontal lines in panel ÕĎDÕí of Fig.
the upper left panel ÕĎAÕí the gain is reduced equally at all
7 show the average absolute threshold for the signal, and the
input levels up to the passive response. In the upper right
associated response level, for those normal-hearing and
panel ÕĎBÕí the reduction in gain is greatest at low input levels,
hearing-impaired listeners used to generate the average re-
with a diminishing reduction as level is increased. In the
sponse functions. Notice that the BM response level at
lower-left panel ÕĎCÕí the gain is reduced at low input levels,
threshold is higher for the hearing-impaired group. This may
but unaffected at high input levels. The lower-right panel ÕĎDÕí
be interpreted as a reduction in sensitivity resulting from
shows average response functions generated from the present
IHC dysfunction. These lines also illustrate the point made in
data. These functions were obtained by averaging the
x and
y
Sec. IV A that the linear segment of the response function
values of the lower breakpoints and the compression expo-
measurable in the experiment ÕĎthreshold to first breakpointÕí
nents derived from the fitting procedure, across the normal-
is shorter for the hearing-impaired listeners.
hearing listeners and across the hearing-impaired listeners.
Upper breakpoints were omitted because they often could
C. Off-frequency temporal masking curves
not be specified ÕĎthe values from the fitting procedure wereabove the highest points on the response functionsÕí, and ÕĎas
A surprising incidental finding of the experiment was
for the gain estimatesÕí the results for ears with less than two
that the slopes of the off-frequency TMCs were
shallower for
points on the response function below the lower breakpoint
hearing-impaired listeners than for normal-hearing listeners
were also omitted. For those ears that remained, it seems
when compared at short masker‚Äďsignal intervals. Recently,
clear that the data are best summarized by option C. Al-
Rosengard
et al. ÕĎ2003Õí have also reported shallow off-
though there are individual differences in the response func-
frequency TMCs in hearing-impaired listeners compared to
tions, overall it appears that mild cochlear hearing loss is
normals. The analysis described in Sec. III A suggests that
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
the difference may be related to the higher off-frequency
ACKNOWLEDGMENTS
masker levels for the hearing-impaired listeners. When the
The authors thank the Associate Editor and two anony-
off-frequency TMC slopes were compared at the same
mous reviewers for very helpful comments on an earlier draft
masker level ÕĎor at long masker‚Äďsignal intervalsÕí there was
of the manuscript, and especially for spotting that the off-
little difference between the groups.
frequency TMC slopes decrease at high levels. The authors
According to the interpretation of TMCs outlined in the
also thank Andrew Oxenham for comments on an earlier
Introduction, the shape of the off-frequency TMC should de-
draft of the manuscript, and Ray Meddis for valuable discus-
pend only on the internal decay of forward masking, a mea-
sions regarding the interpretation of the data. The research
sure of temporal resolution. There is little evidence to sug-
was supported by EPSRC Grant GR/N07219. Author EALP
gest that hearing-impaired listeners in general have a deficit
was supported by FIS PI020343 and G03/203.
in temporal resolution, at least as measured by tasks such asgap detection with sinusoidal markers ÕĎMoore and Glasberg,1988Õí and modulation detection ÕĎBacon and Gleitman, 1992;
Bacon, S. P., and Gleitman, R. M. ÕĎ
1992 Õí. ‚Äė‚ÄėModulation detection in subjects
with relatively flat hearing losses,’’ J. Speech Hear. Res.
35 , 642‚Äď 653.
Moore
et al. , 1992Õí. However, it is the case that the hearing-
Baker, R. J., and Rosen, S. ÕĎ
2002 Õí. ‚Äė‚ÄėAuditory filter nonlinearity in mild/
impaired listeners in the present study were older and re-
moderate hearing impairment,’’ J. Acoust. Soc. Am.
111 , 1330‚Äď1339.
ceived less training than the normal-hearing listeners, and
Furukawa, T., and Matsuura, S. ÕĎ
1978 Õí. ‚Äė‚ÄėAdaptive rundown of excitatory
this may have influenced temporal processing. If the effects
post-synaptic potentials at synapses between hair cells and eighth-nerve
fibers in the goldfish,‚Äô‚Äô J. Physiol. ÕĎLondonÕí
276 , 193‚Äď209.
of hearing impairment on the off-frequency TMCs were
not a
Heinz, M. G., Scepanovic, D., Sachs, M. B., and Young, E. D. ÕĎ
in press Õí.
consequence of a general temporal resolution deficit, two
‚Äė‚ÄėNormal and impaired level encoding: Effects of noise-induced hearing
possibilities remain. The first is that the aspect of temporal
loss,’’ in
Auditory Signal Processing: Physiology, Psychoacoustics, and
resolution measured by forward masking is unconnected
Models , edited by D. Pressnitzer, A. de Cheveigne¬ī, S. McAdams, and L.
Collet ÕĎSpringer, New YorkÕí.
with the aspect ÕĎor aspectsÕí measured in other tasks, and that
Hicks, M. L., and Bacon, S. P. ÕĎ
1999a Õí. ‚Äė‚ÄėEffects of aspirin on psychophysi-
hearing-impaired listeners have a specific deficit in forward
cal measures of frequency selectivity, two-tone suppression, and growth of
masking. This might be possible if forward masking is a
masking,’’ J. Acoust. Soc. Am.
106 , 1436 ‚Äď1451.
Hicks, M. L., and Bacon, S. P. ÕĎ
1999b Õí. ‚Äė‚ÄėPsychophysical measures of au-
consequence of adaptation at the IHC/auditory nerve synapseÕĎ
ditory nonlinearities as a function of frequency in individuals with normal
Furukawa and Matsuura, 1978; but see Oxenham, 2001;
hearing,’’ J. Acoust. Soc. Am.
105 , 326 ‚Äď338.
Smith, 1979Õí, and that IHC dysfunction affects this in some
Levitt, H. ÕĎ
1971 Õí. ‚Äė‚ÄėTransformed up-down methods in psychoacoustics,‚Äô‚Äô J.
way. The second possibility is that the auditory system re-
Acoust. Soc. Am.
49 , 467‚Äď 477.
Liberman, M. C., Dodds, L. W., and Learson, D. A. ÕĎ
1986 Õí. ‚Äė‚ÄėStructure‚Äď
sponds nonlinearly to an off-frequency masker, either at the
function correlation in noise-damaged ears: A light and electron-
level of the BM or more centrally. To account for the differ-
microscopic study,’’ in
Basic and Applied Aspects of Noise-Induced Hear-
ence between the normal and impaired ears, the off-
ing Loss , edited by R. J. Salvi, D. Henderson, R. P. Hamernik, and V.
frequency compression exponent may be invariant with level
Lopez-Poveda, E. A., Plack, C. J., and Meddis, R. ÕĎ
2003 Õí. ‚Äė‚ÄėCochlear non-
but increased in impaired ears ÕĎleading to a shallow TMC
linearity between 500 and 8000 Hz in listeners with normal hearing,’’ J.
slope in impaired earsÕí, or the compression exponent may be
Acoust. Soc. Am.
113 , 951‚Äď960.
increased at high levels ÕĎleading to a shallow TMC slope at
Lopez-Poveda, E. A., Plack, C. J., Meddis, R., and Blanco, J. L. ÕĎ
2004 Õí.
high levelsÕí. The finding that the TMC slopes were similar
‚Äė‚ÄėCochlear nonlinearity between 500 and 8000 Hz in listeners with mod-erate cochlear hearing loss,‚Äô‚Äô Abstracts of the Twenty-Seventh Annual
for normal and impaired ears at long masker‚Äďsignal intervals
Midwinter Meeting of the Ass. Res. Otolaryngol., Daytona Beach, FL.
McFadden, D. ÕĎ
1986 Õí. ‚Äė‚ÄėThe curious half octave shift: Evidence for a basal-
ward migration of the travelling-wave envelope with increasing intensity,’’in
Basic and Applied Aspects of Noise-Induced Hearing Loss , edited by R.
J. Salvi, D. Henderson, R. P. Hamernik, and V. Colletti ÕĎPlenum, New
V. CONCLUSIONS
Moore, B. C. J. ÕĎ
1995 Õí.
Perceptual Consequences of Cochlear Damage
BM response functions derived from on- and off-
ÕĎOxford University Press, OxfordÕí.
frequency TMCs generally show a linear low-level
Moore, B. C. J., and Glasberg, B. R. ÕĎ
1988 Õí. ‚Äė‚ÄėGap detection with sinusoids
region and a compressive midlevel region. With hear-
and noise in normal, impaired and electrically stimulated ears,’’ J. Acoust.
ing loss the low-level region shifts to the right, re-
Soc. Am.
83 , 1093‚Äď1101.
Moore, B. C. J., and Glasberg, B. R. ÕĎ
1997 Õí. ‚Äė‚ÄėA model of loudness percep-
flecting the reduction in sensitivity, but there is little
tion applied to cochlear hearing loss,’’ Aud. Neurosci.
3 , 289‚Äď311.
evidence for a change in the slope of the compressive
Moore, B. C. J., Shailer, M. J., and Schooneveldt, G. P. ÕĎ
1992 Õí. ‚Äė‚ÄėTemporal
region with losses up to 50 dB or so.
modulation transfer functions for bandlimited noise in subjects with co-
The results suggest that mild to moderate sensorineu-
chlear hearing loss,’’ Br. J. Audiol.
26 , 229‚Äď237.
Moore, B. C. J., Vickers, D. A., Plack, C. J., and Oxenham, A. J. ÕĎ
1999 Õí.
ral hearing loss is associated with a reduction in the
‚Äė‚ÄėInter-relationship between different psychoacoustic measures assumed to
gain for low-level CF tones, but little change in the
be related to the cochlear active mechanism,’’ J. Acoust. Soc. Am.
106 ,
gain for higher-level tones, and consequently little
Murugasu, E., and Russell, I. J. ÕĎ
1995 Õí. ‚Äė‚ÄėSalicylate ototoxicity: The effects
on basilar membrane displacement, cochlear microphonics, and neural re-
sponses in the basal turn of the guinea pig cochlea,’’ Aud. Neurosci.
1 ,
frequency TMCs than normal-hearing listeners when
measured at short time intervals. However, there is
Neff, D. L. ÕĎ
1986 Õí. ‚Äė‚ÄėConfusion effects with sinusoidal and narrow-band-
little effect of impairment on TMC slope at long time
noise forward maskers,’’ J. Acoust. Soc. Am.
79 , 1519‚Äď1529.
Nelson, D. A., Schroder, A. C., and Wojtczak, M. ÕĎ
2001 Õí. ‚Äė‚ÄėA new procedure
intervals, or if the TMCs are matched for off-
for measuring peripheral compression in normal-hearing and hearing-
impaired listeners,’’ J. Acoust. Soc. Am.
110 , 2045‚Äď2064.
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
Oxenham, A. J. ÕĎ
2001 Õí. ‚Äė‚ÄėForward masking: Adaptation or integration?‚Äô‚Äô J.
from growth-of-masking functions and temporal masking curves,’’ Ab-
Acoust. Soc. Am.
109 , 732‚Äď741.
stracts of the Twenty-Sixth Annual Midwinter Research Meeting of the
Oxenham, A. J., and Plack, C. J. ÕĎ
1997 Õí. ‚Äė‚ÄėA behavioral measure of basilar-
Ass. Res. Otolaryngol., Daytona Beach, FL.
membrane nonlinearity in listeners with normal and impaired hearing,’’ J.
Ruggero, M. A., and Rich, N. C. ÕĎ
1991 Õí. ‚Äė‚ÄėFurosemide alters organ of Corti
Acoust. Soc. Am.
101 , 3666 ‚Äď3675.
mechanics: Evidence for feedback of outer hair cells upon the basilar
Plack, C. J., and Drga, V. ÕĎ
2003 Õí. ‚Äė‚ÄėPsychophysical evidence for auditory
membrane,’’ J. Neurosci.
11 , 1057‚Äď1067.
compression at low characteristic frequencies,’’ J. Acoust. Soc. Am.
113 ,
Ruggero, M. A., Rich, N. C., Recio, A., Narayan, S. S., and Robles, L.
ÕĎ
1997 Õí. ‚Äė‚ÄėBasilar-membrane responses to tones at the base of the chinchilla
Plack, C. J., and Oxenham, A. J. ÕĎ
2000 Õí. ‚Äė‚ÄėBasilar-membrane nonlinearity
cochlea,’’ J. Acoust. Soc. Am.
101 , 2151‚Äď2163.
estimated by pulsation threshold,’’ J. Acoust. Soc. Am.
107 , 501‚Äď507.
Smith, R. L. ÕĎ
1979 Õí. ‚Äė‚ÄėAdaptation, saturation, and physiological masking in
Robles, L., Ruggero, M. A., and Rich, N. C. ÕĎ
1986 Õí. ‚Äė‚ÄėBasilar membrane
single auditory-nerve fibers,’’ J. Acoust. Soc. Am.
65 , 166 ‚Äď178.
mechanics at the base of the chinchilla cochlea. I. Input‚Äďoutput functions,
Yasin, I., and Plack, C. J. ÕĎ
2003 Õí. ‚Äė‚ÄėThe effects of a high-frequency suppres-
tuning curves, and phase responses,’’ J. Acoust. Soc. Am.
80 , 1364 ‚Äď
sor on tuning curves and derived basilar-membrane response functions,’’ J.
Acoust. Soc. Am.
114 , 322‚Äď332.
Rosengard, P. S., Oxenham, A. J., and Braida, L. D. ÕĎ
2003 Õí. ‚Äė‚ÄėEstimates of
Yates, G. K. ÕĎ
1995 Õí. ‚Äė‚ÄėCochlear structure and function,‚Äô‚Äô in
Hearing , edited
basilar-membrane compression in listeners with normal hearing derived
by B. C. J. Moore ÕĎAcademic, San DiegoÕí, pp. 41‚Äď73.
J. Acoust. Soc. Am., Vol. 115, No. 4, April 2004
Plack et al.: Nonlinearity and hearing loss
Source: http://audiolab.usal.es/Documentos/ArticulosLAB/Plack_etal_JASA2004.pdf
GUIDE POUR LA R√ČDACTION ET LA PR√ČSENTATION DES TH√ąSES A L‚ÄôUSAGE DES DOCTORANTS * Valoriser les th√®ses en privil√©giant l‚Äôinternet ‚Ķ. 3Valoriser dans le respect de la r√©glementation ‚Ķ. 4Comment structurer sa th√®se pour faciliter sa diffusion : √©l√©ments obligatoires . 5Comment pr√©senter sa th√®se pour favoriser sa lisibilit√© . 8 * Le pr√©sent guide concerne les th√
HIGH STRENGTH FINE GRAINED STRUCTURAL STEEL DILLIMAX 890 is a high strength quenched and tempered, fine grained structural steel with a minimum yield strength of 890 N/mm² in its delivered condition (referring to the lowest thickness range), whose mechanical properties are achieved by water quenching followed by tempering. DILLIMAX 890 fulfils the requirements of EN 10 137. It is preferentia
A |
B |
C |
D |
E |
F |
G |
H |
I |
J |
K |
L |
M |
N |
O |
P |
Q |
R |
S |
T |
U |
V |
W |
X |
Y |
Z |
0-9
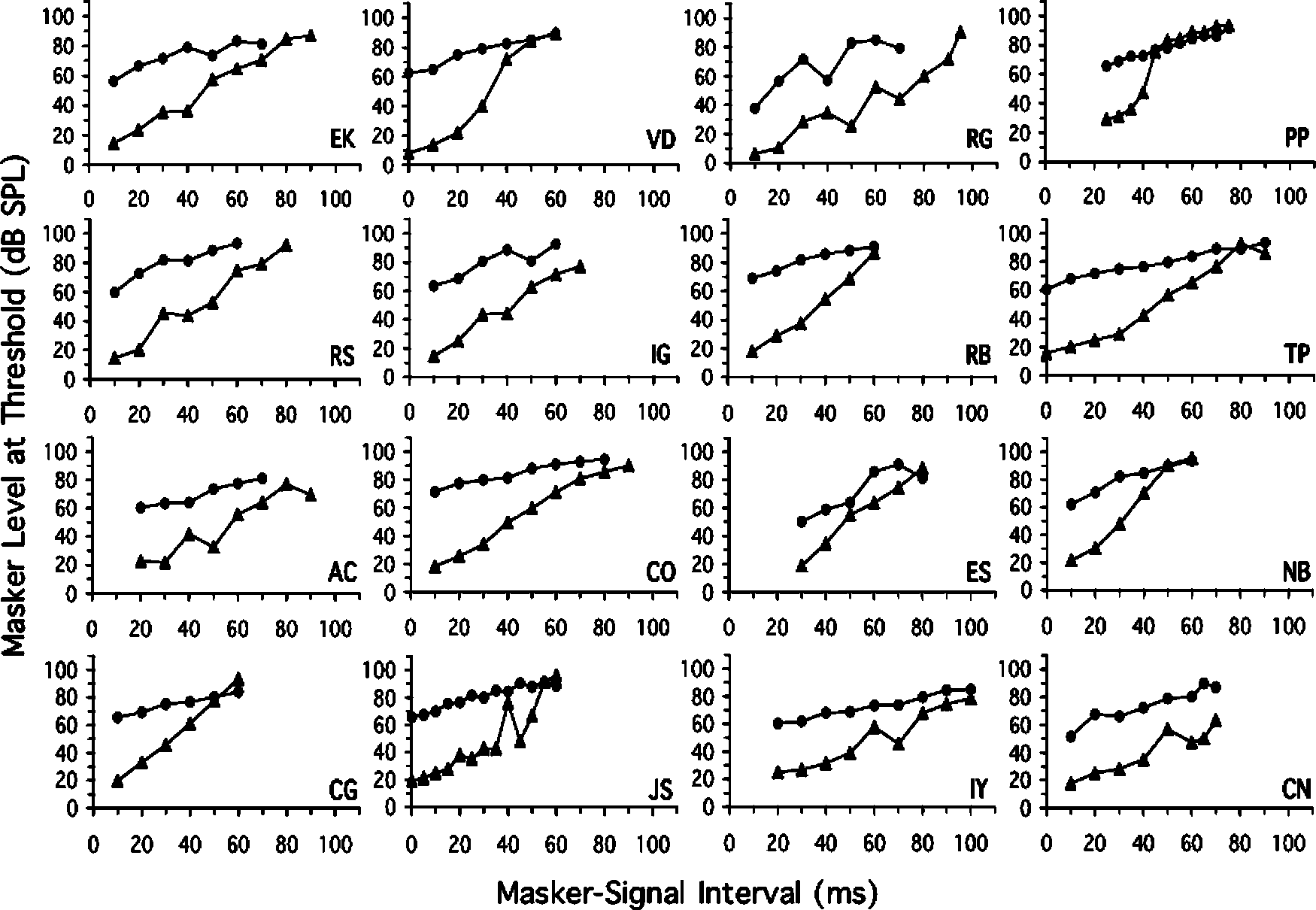
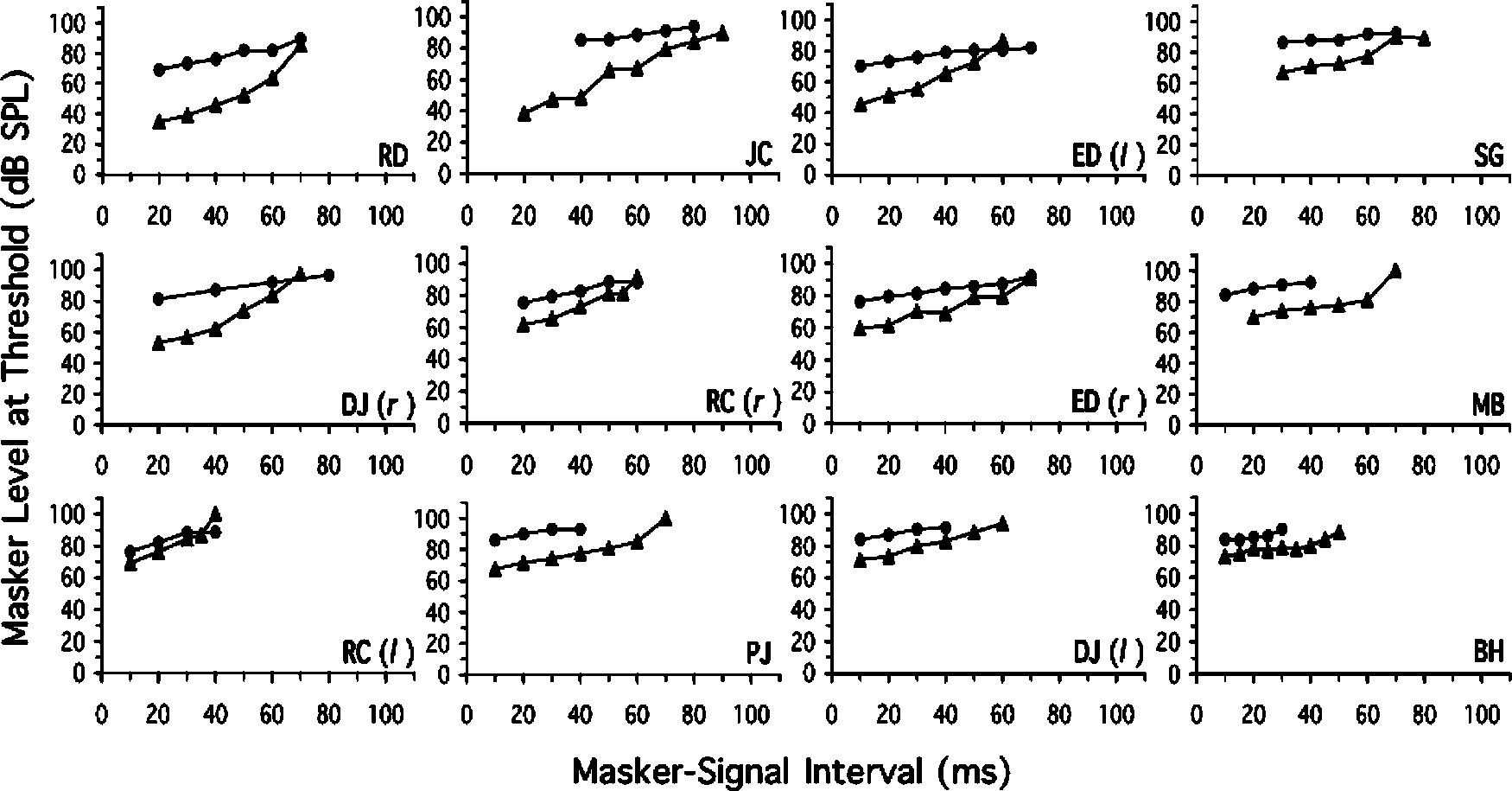 FIG. 1. TMCs for normal-hearing listeners, showing mean masker level at threshold as a function of masker‚Äďsignal interval for on-frequency ÕĎ4000-HzÕímaskers ÕĎtrianglesÕí and off-frequency ÕĎ2200-HzÕí maskers ÕĎcirclesÕí.
FIG. 1. TMCs for normal-hearing listeners, showing mean masker level at threshold as a function of masker‚Äďsignal interval for on-frequency ÕĎ4000-HzÕímaskers ÕĎtrianglesÕí and off-frequency ÕĎ2200-HzÕí maskers ÕĎcirclesÕí.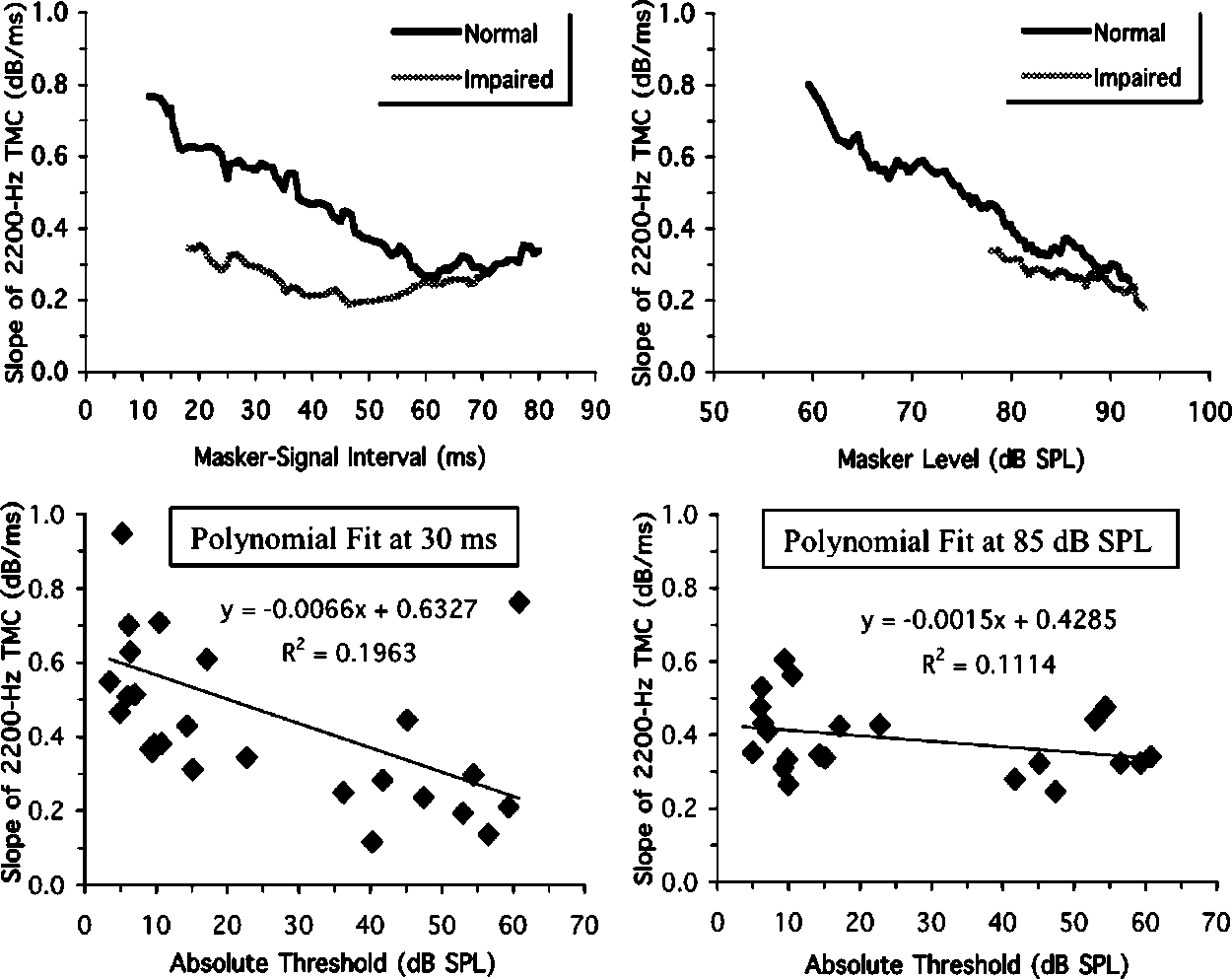 FIG. 3. The upper panels show the slopes of the2200-Hz TMCs, collapsed across listeners and plottedas running averages over 20 consecutive points. Theslopes are shown as a function of masker‚Äďsignal inter-val ÕĎupper leftÕí and masker level ÕĎupper rightÕí. Thelower panels show scatterplots of 2200-Hz TMC slopeagainst signal absolute threshold. The slopes were de-rived by fitting second-order polynomials to the TMCdata for each listener. The slopes at a masker‚Äďsignalinterval of 30 ms ÕĎlower leftÕí and at a masker level of85 dB SPL ÕĎlower rightÕí were calculated from the fittedfunctions. The lines show linear regression fits, withequations and R2 values displayed on the figure.
FIG. 3. The upper panels show the slopes of the2200-Hz TMCs, collapsed across listeners and plottedas running averages over 20 consecutive points. Theslopes are shown as a function of masker‚Äďsignal inter-val ÕĎupper leftÕí and masker level ÕĎupper rightÕí. Thelower panels show scatterplots of 2200-Hz TMC slopeagainst signal absolute threshold. The slopes were de-rived by fitting second-order polynomials to the TMCdata for each listener. The slopes at a masker‚Äďsignalinterval of 30 ms ÕĎlower leftÕí and at a masker level of85 dB SPL ÕĎlower rightÕí were calculated from the fittedfunctions. The lines show linear regression fits, withequations and R2 values displayed on the figure.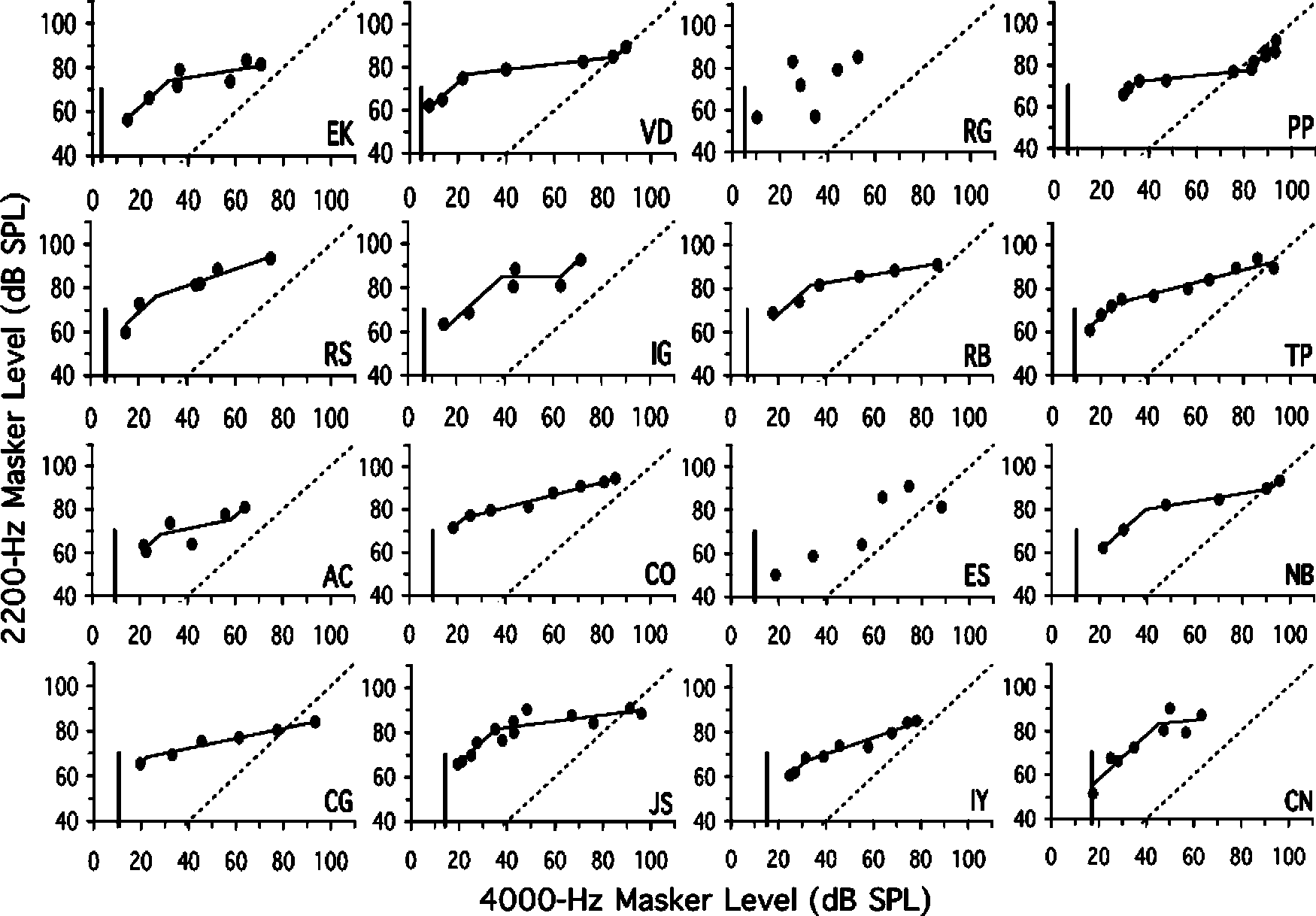
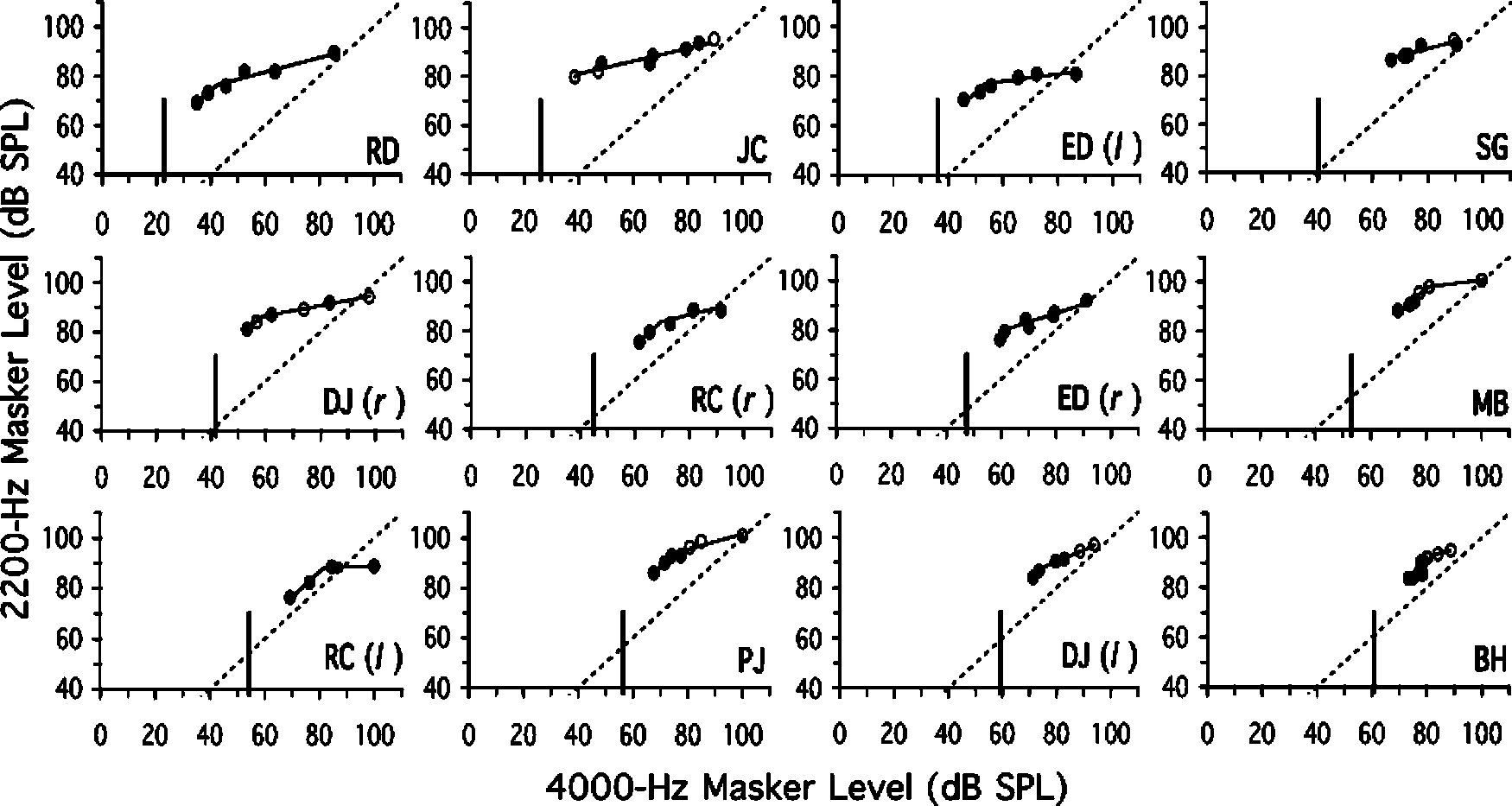 FIG. 4. Estimated response functions for normal-hearing listeners, showing the 2200-Hz masker level at threshold plotted against the 4000-Hz masker levelat threshold, paired according to masker‚Äďsignal interval. The positive diagonal ÕĎstraight lineÕí indicates the expected response of a passive, linear system. Thevertical line indicates signal absolute threshold (re: the x axisÕí. The kinked line shows the piecewise linear fit ÕĎsee the text for detailsÕí.
FIG. 4. Estimated response functions for normal-hearing listeners, showing the 2200-Hz masker level at threshold plotted against the 4000-Hz masker levelat threshold, paired according to masker‚Äďsignal interval. The positive diagonal ÕĎstraight lineÕí indicates the expected response of a passive, linear system. Thevertical line indicates signal absolute threshold (re: the x axisÕí. The kinked line shows the piecewise linear fit ÕĎsee the text for detailsÕí.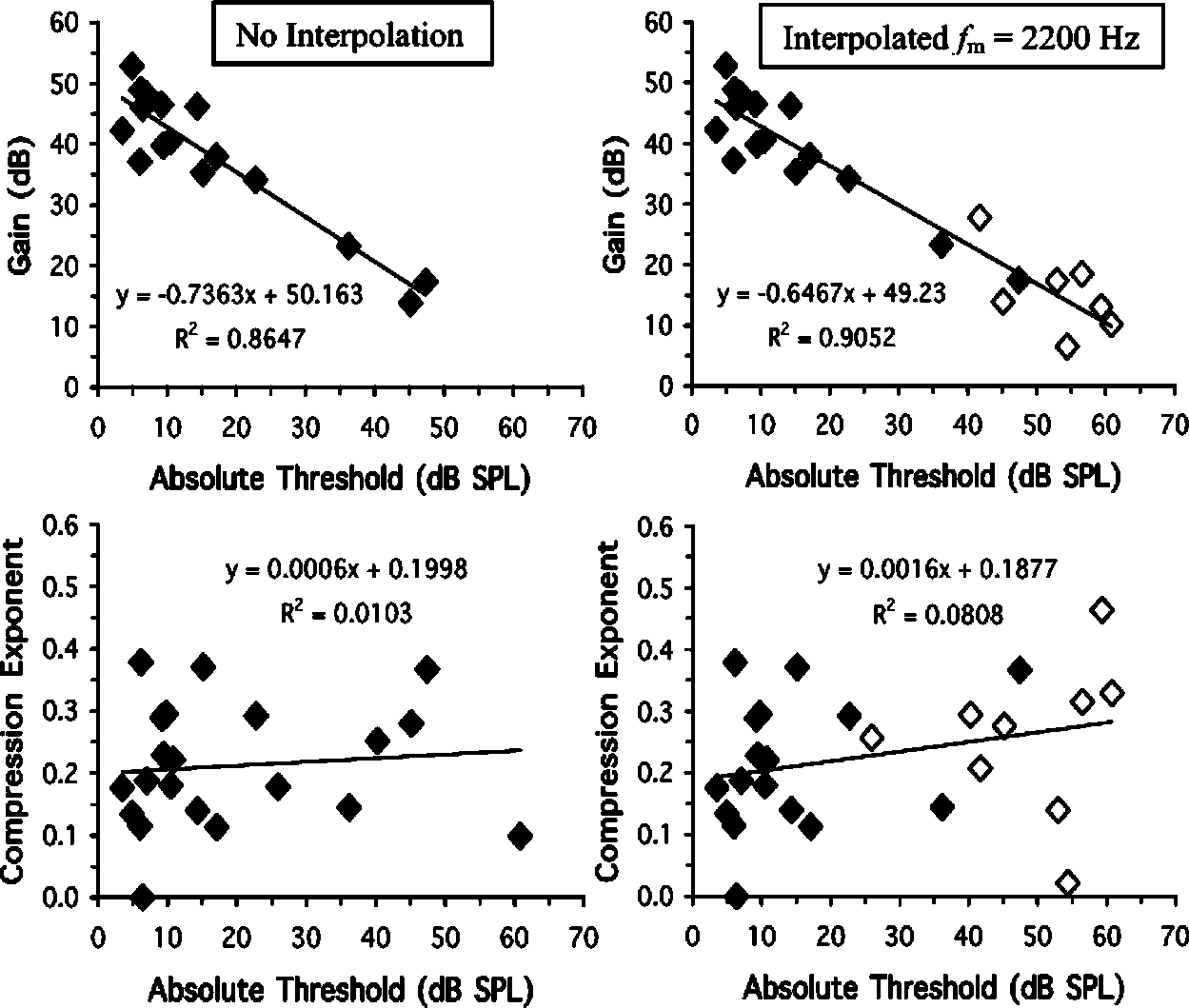 FIG. 6. Scatterplots of maximum gain against signalabsolute threshold ÕĎupper panelsÕí, and response-function slope against signal absolute threshold ÕĎlowerpanelsÕí, at 4000 Hz. The left-hand panels show the re-sults for response functions generated without interpo-lation. The right-hand panels include the results for re-sponse functions that were generated using interpolatedoff-frequency masker levels ÕĎindicated by the opensymbolsÕí. Gain estimates are only included when thelow-level portion of the response function is defined byat least two points ÕĎsee Table IÕí.
FIG. 6. Scatterplots of maximum gain against signalabsolute threshold ÕĎupper panelsÕí, and response-function slope against signal absolute threshold ÕĎlowerpanelsÕí, at 4000 Hz. The left-hand panels show the re-sults for response functions generated without interpo-lation. The right-hand panels include the results for re-sponse functions that were generated using interpolatedoff-frequency masker levels ÕĎindicated by the opensymbolsÕí. Gain estimates are only included when thelow-level portion of the response function is defined byat least two points ÕĎsee Table IÕí.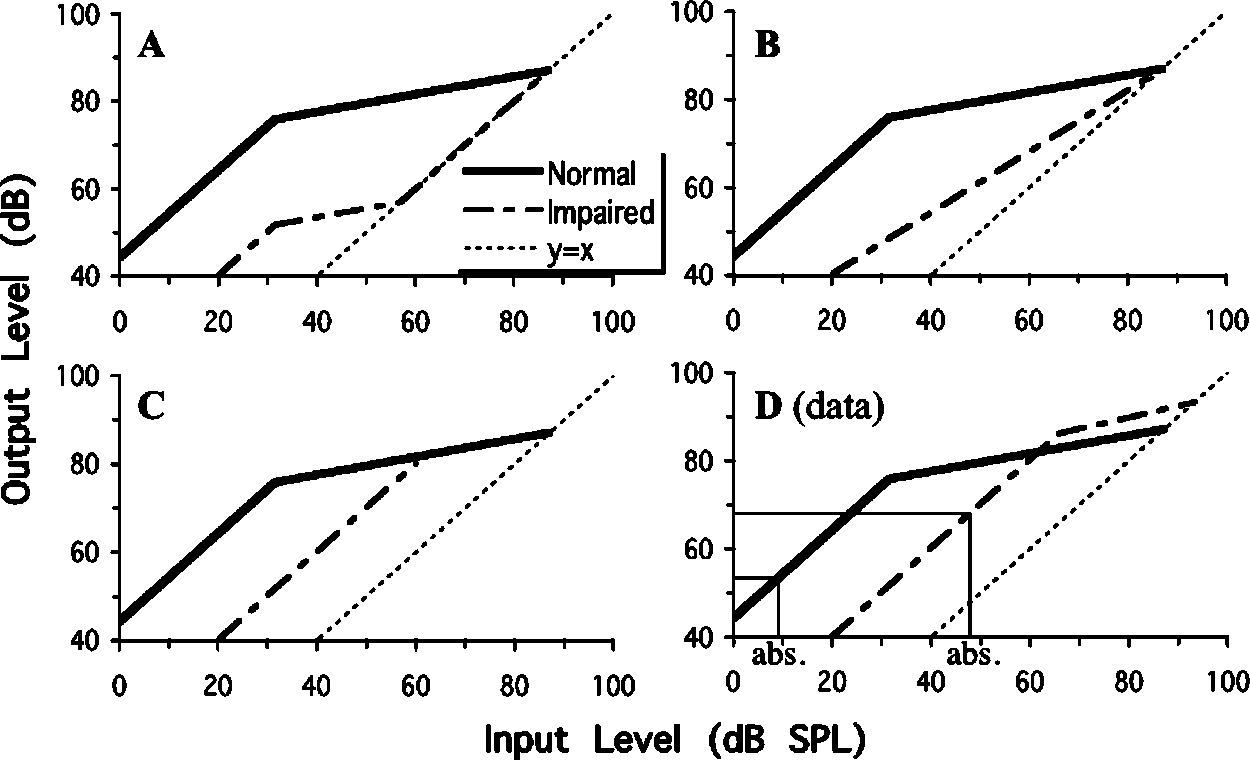 FIG. 7. BM response functions for normal-hearing andhearing-impaired listeners. The normal response func-tion is an average function generated from the presentdata ÕĎsee the text for detailsÕí. In panels ÕĎAÕí to ÕĎCÕí theresponse functions for the hearing-impaired listenersare hypothetical. In panel ÕĎAÕí, the gain for hearing-impaired listeners is reduced equally at all input levelsup to the passive response. In panel ÕĎBÕí, the reductionin gain is greatest at low input levels, with a diminish-ing reduction as level is increased. In panel ÕĎCÕí, thegain is reduced at low input levels, but unaffected athigh input levels. Panel ÕĎDÕí shows average responsefunctions,
impaired listeners, generated from the present data ÕĎseethe text for detailsÕí. In panel ÕĎDÕí, the thin vertical linesshow the average absolute thresholds for the signal, andthe thin horizontal lines the associated response levels,for the normal-hearing and hearing-impaired listenersused to generate the response functions.
FIG. 7. BM response functions for normal-hearing andhearing-impaired listeners. The normal response func-tion is an average function generated from the presentdata ÕĎsee the text for detailsÕí. In panels ÕĎAÕí to ÕĎCÕí theresponse functions for the hearing-impaired listenersare hypothetical. In panel ÕĎAÕí, the gain for hearing-impaired listeners is reduced equally at all input levelsup to the passive response. In panel ÕĎBÕí, the reductionin gain is greatest at low input levels, with a diminish-ing reduction as level is increased. In panel ÕĎCÕí, thegain is reduced at low input levels, but unaffected athigh input levels. Panel ÕĎDÕí shows average responsefunctions,
impaired listeners, generated from the present data ÕĎseethe text for detailsÕí. In panel ÕĎDÕí, the thin vertical linesshow the average absolute thresholds for the signal, andthe thin horizontal lines the associated response levels,for the normal-hearing and hearing-impaired listenersused to generate the response functions.