La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Microsoft word - psr handout - 01-15-2010.doc
Table of Contents Policy Number and Name
2010 - Maintenance of EMS Personnel Lists:.4 2540 - Paramedic Accreditation:.4 2540B - Skills Verification Form:.6 2541 – Paramedic Infrequently Used Skills:.6 2545 - Endotracheal Intubation – Adult Performance Criteria: .6 2546 – Intraosseous Cannulation Performance Criteria:.7 2547 - Transcutaneous Pacing (TCP) Performance Criteria:.8 2548 – Needle Thoracostomy Performance Criteria:.8 2549 – Needle Cricothyrotomy Performance Criteria: .9 2552 – King Airway Performance Criteria: .10 2553 – Endotracheal Intubation – Pediatric Performance Criteria: .12 2554 – Continuous Positive Airway Pressure (CPAP): .13 2560 – Paramedic Scope of Practice: .14 3410 – ALS Field to Hospital Communications: .15 3411 – ALS Reporting Format:.16 4200 – Management of Controlled Substances:.16 4102 – ALS Medical and Equipment Inventory: .17 4447 – EMS Aircraft Landing Sites:.17 4448 – EMS Aircraft Utilization:.18 4980 – Receiving Hospital Diversion: .19 5102 – Patient Privacy: .19 5103 – Determination of Death in the Field:.20 5105 – Do Not Resuscitate (DNR):.22 5106 – Interaction with Physician or Other Health Care Provider on Scene:.22 5107 – Use of Restraints: .23 5108 – Care of Minors in the Field: .23 5110 – Anatomical Donor Cards:.23 5120 – Triage of Neonates and High Risk Pregnancy: .24 5121 – Neurological Triage Criteria: .24 5122 – Pediatric Trauma Triage Criteria: .24 5130 – ALS Without Base Hospital Contact: .25 5506 – Spinal Immobilization: .25 5561 – BLS Childbirth: .26 5700 – ALS Treatment Policy – Introduction:.26 5701 – Routine ALS Care: .27 5702 – ALS Advanced Airway Management: .27 5707 – ALS Adult Pain Management: .28 5711 – ALS Ventricular Fibrillation/Pulseless Vtach:.29 5712 – ALS Wide Complex Tachycardia with a Pulse:.29 5713 – ALS Narrow Complex Tachycardia: A-Fib/A-Flutter: .30 5714 – ALS Narrow Complex Tachycardia; SVT: .30 5715 – ALS Asystole: .31 5716 – ALS Pulseless Electrical Activity (PEA): .31 5717 – ALS Bradydysrhythmias: .31 5719 – ALS Acute Coronary Syndrome (ACS):.32
5721 – ALS Hypertension:.32 5724 – ALS Ventricular Ectopy:.32 5726 – ALS Return of Spontaneous Circulation (ROSC): .33 5731 – ALS Allergic Reaction/Anaphylaxis:.33 5733 – ALS Poisoning/Overdose:.34 5736 – ALS Hypothermia: .35 5738 – ALS Envenomation: .35 5751 – ALS Altered Level of Consciousness (ALOC):.35 5753 – ALS Seizures:.36 5754 – ALS Acute Stroke: .36 5762 – ALS Vaginal Hemorrhage with Shock: .36 5763 – ALS Severe Pre-Eclampsia/Eclampsia: .37 5764 – ALS Imminent Delivery:.37 5771 – ALS Bronchospasm: .37 5772 – ALS Acute Pulmonary Edema: .37 5774 – ALS Airway Obstruction: .38 5781 – ALS Amputation: .38 5782 – ALS Burn Care:.38 5783 – ALS Major Trauma: .38 5784 – ALS Traumatic Arrest:.39 5800 – Pediatric Routine Medical Care: .39 5810 – Pediatric Pulseless Arrest Asystole/PEA: .39 5811 - Pediatric Pulseless Arrest Ventricular Fibrillation/Ventricular Tachycardia: .40 5812 – Pediatric Bradydysrhythmias: .40 5813 – Pediatric Tachycardia with Pulses: .41 5815 – Pediatric Apparent Life Threatening Event: .42 5817 – Pediatric Airway Obstruction by Foreign Body:.42 5819 – Pediatric Respiratory : Stridor:.43 5820 – Pediatric Respiratory Distress: Bronchospasm: .43 5824 – Pediatric Shock:.44 5826 – Pediatric Allergic Reaction: .44 5828 – Pediatric Seizures: .44 5829 – Pediatric Altered Level of Consciousness:.45 5830 – Pediatric Poisoning/Overdose: .45 5833 – Pediatric Trauma: .46 5837 – Pediatric Burns: .46 5839 – Pediatric Pain Management:.46 5850 – Neonatal Resuscitation:.47 5954 – Monitoring an Intravenous Infusion of Heparin: .47 5995 – Monitoring an Intravenous Infusion of Nitroglycerin:.47 6101 – Sentinel Event Reporting Requirements Policy: .47
The following are excerpts of EMS Policies and are not the complete Policies. Prehospital providers are still responsible for knowing the entire content of each San Joaquin County EMS Policy. While the Policy identification numbers and text cited in this handout are identical to the referenced Policies, the numbers and letters denoting different policy sections do not corresponded with those found within those Policies (e.g. I, A, 1, etc). This handout is designed as a study guide for the Policy examination and is not authorized for field use. 2010 - Maintenance of EMS Personnel Lists:
A. San Joaquin County accredited, authorized and certified EMS personnel shall maintain
up-to-date contact information with the EMS Agency.
B. Authorized advanced life support (ALS) providers shall maintain up-to-date contact
information and a current list of ALS and basic life support (BLS) personnel with the EMS Agency.
C. Individuals shall complete and submit a Personnel Update Form (Appendix A) to the
EMS Agency within thirty (30) days of a change occurring. A change of address may also be submitted online from the EMS Agency website: www.sjgov.org/ems/documents.htm.
D. Authorized ALS providers shall complete and submit a Provider Update Form
(Appendix B) to the EMS Agency within thirty (30) days of a change occurring. This form is intended for use in reporting personnel assignment changes as-well-as changes in provider contact information.
2540 - Paramedic Accreditation:
1. Once a paramedic candidate applies for accreditation and is waiting to attend
orientation, they may begin working as a paramedic using only the basic scope of practice for the State of California and while under the direct supervision of another San Joaquin County accredited paramedic preceptor. Paramedics who have not completed the accreditation process may not function as a paramedic without their assigned paramedic preceptor present.
B. Maintaining Continuous Accreditation:
1. Paramedics shall complete the following to maintain continuous accreditation:
a. Complete the Paramedic Accreditation Application, no later than thirty (30)
days prior to expiration of their accreditation.
b. Provide proof of employment with an approved San Joaquin County ALS
c. Maintain a California Paramedic License. d. Submit copies of the following to the EMS Agency:
identification card (i.e., driver’s license) or valid federal
identification (i.e., Military Identification)
2) Valid California paramedic license; 3) Current certification in cardiopulmonary resuscitation (CPR) for the
Professional Rescuer or Healthcare Provider.
e. Complete a policy and skills review (PSR), within six (6) months of expiration. f.
Successfully pass with a score of 80% or higher with a closed book
examination of the San Joaquin County Policies which will be administered at the end of the PSR. (Refer to the Testing Procedures section of this policy for information on scores of below 80 %).
C. Reinstatement After Lapse in Accreditation:
1. In order for an individual whose accreditation has lapsed to be eligible for renewal,
the following applies: a. For a lapse of less than six (6) months, the paramedic shall: pay the
accreditation fee and meet all requirements listed in Section III (Maintaining Continuous Accreditation).
b. For a lapse of more than six (6) months: complete the initial accreditation
D. Mutual Aid (Out of County): When responding into another local EMS agency’s
jurisdiction during an interfacility transfer, mutual aid response or emergency response, San Joaquin County accredited paramedics shall utilize the San Joaquin County paramedic scope of practice.
E. Testing Procedures: An individual will be allowed to take the Accreditation/Policy
examination a maximum of three (3) times: 1. First Attempt: Scheduled based upon EMS Agency availability; 2. Second Attempt: May be scheduled after a one (1) week waiting period from the
3. Third Attempt: At least four (4) hours of remedial training shall be completed
through the paramedic’s employer relating to the San Joaquin County EMS Policies. The employer shall submit written documentation of such training prior to scheduling a third attempt for testing.
4. For continuous accreditation, the paramedic will be required to attend remedial
training conducted by the SJCEMSA until such time the paramedic passes the examination. If the paramedic’s accreditation lapses during this time, the paramedic must meet the requirements in maintaining continuous accreditation section. Additionally, after three (3) failed attempts the EMS Agency Medical Director may refer the paramedic to the California EMS Authority for further evaluation.
5. For initial accreditation the individual shall reapply for accreditation in order to re-
enter the accreditation process if any of the following occurs: a. Failure to pass the written examination three times; b. Failure to complete the authorization process within forty-five (45) days. Note:
At the discretion of the EMS Agency, this time frame may be extended upon receipt of a written request from the applicant outlining extenuating circumstances.
2540B - Skills Verification Form:
The following is an excerpt of 2540B, which lists the optional skills and medication only:
Pediatric Intubation
Intravenous Heparin infusion Intraosseous infusion Magnesium Sulfate External cardiac pacing
Intravenous Nitroglycerin infusion Nasal Intubation Continuous Positive Airway Pressure Atrovent 12 Lead EKG 2541 – Paramedic Infrequently Used Skills:
A. Demonstration of competency in infrequently utilized skills is to be performed in a
B. Providers are required to develop a process that affords all ALS personnel the
opportunity to demonstrate competency at the required intervals.
C. Providers and ALS personnel shall follow the process specified in EMS Agency Policy
when verifying an infrequently used skill.
D. Providers shall ensure sufficient training resources are available to implement the
E. Providers shall make records available to the EMS Agency, upon request, to
demonstrate compliance with this Policy.
F. The infrequently used skills and intervals at which competency shall be demonstrated
by ALS personnel are as follows: 1. Adult Endotracheal Intubation – Quarterly 2. Pediatric
3. Nasotracheal Intubation – Quarterly 4. Transcutaneous Cardiac Pacing – Annually 5. Intraosseous Infusions – Annually 6. Needle Thoracostomy – Annually 7. Needle Cricothyromoty – Annually
G. Effective July 1, 2010 the frequency for adult endotracheal intubation changes to
H. Effective January 1, 2011 the frequency for adult endotracheal intubation changes to
2545 - Endotracheal Intubation – Adult Performance Criteria:
1. Use universal precautions. 2. States this is a two (2) person procedure 3. Assures an adequate BLS airway. 4. State indications and contraindications. 5. States placement should be completed within 30 seconds 6. Ensure suction and is available and working. 7. Checks light source, ensures a bright, tight, white light. 8. Select appropriate size tube. 9. Check tube cuff for leaks by injecting air into cuff with syringe and deflates cuff.
10. Instruct assistant to preoxyegnate the patient. 11. Position patient in the “ear to sternal notch position”. Understands when to use
bimanual laryngoscopy (optimal external laryngeal manipulation (OELM)) and how it is performed.
12. Prepares to insert tube. 13. Gently inserts laryngoscope blade into mouth and applies upward traction with left
14. The paramedic introduces the ETTI into the patient's mouth and gently advances it
through the glottic opening. The ETTI should rest midline in the trachea and should not be advanced past 23 cm or the black line on the ETTI. Does Not Use Teeth As A Fulcrum.
15. Assistant places ET over ETTI and gently rotates down toward mouth. 16. Paramedic takes over tube and rotates it in a counter clockwise motion, until the
tube is placed in the trachea. If resistance is felt, the tube is rotated 90˚ clockwise and advanced.
17. The paramedic continues to visualize the cords until the tube is placed. 18. Once the tube is in placed, the assistant removes the ETTI while stabilizing tube
19. Inflated cuff with 10 ml of air and detaches syringe. 20. Simultaneously maintains tube position, ventilates patient and confirms tube
placement by: a. Notating capnography readings. PPV at the appropriate CO2 level as well as
b. Observing bilateral rise and fall of chest wall. c. Auscultating bilateral breath sounds with absence of sounds over abdomen. d. Confirm placement with end tidal CO2 device.
21. If initial attempt at intubation fails, reattempt after hyperventilation period of 15-30
22. If air was heard on the right side only, what would you do? (Indicates would deflate
the cuff, pull tube back slightly -1 cm, re-inflate the cuff, and auscultate for bilateral air entry).
23. Note tube markers at front teeth, secures tube, and places oral airway. 24. Provide ventilations at 10 – 12 per minute 25. Successfully intubates in no more than two (2) attempts per patient with
hyperventilation between attempts. If unsuccessful after two (2) attempts, considers Combi-Tube/King Airway
2546 – Intraosseous Cannulation Performance Criteria:
1. Resuscitation 2. Urgent need to administer fluids or medications intravenously with inability to
establish peripheral on two (2) attempts.
1. Fractures of involved bone. 2. Infected burn or area of cellulitis overlying the site of insertion. 3. Congenital deformity or history of osteogenesis imperfecta or osteopetrosis.
C. Potential complications and interventions:
1. Needle becomes obstructed with bone or bone marrow: replace with a second
needle by passing through the same cannulation site, provided no evidence of infiltration is observed, or consider IO cannulation of contralateral tibia.
2. Local infiltration of fluids, medications, or local bleeding: stop infusion and apply
1. Uses universal precautions. 2. States indications, age limit, and contraindications of IO cannulation. 3. Assembles equipment and checks the needle to ensure bevels of the outer needle
and internal stylet are properly aligned.
4. Identifies insertion site at the proximal, anterior tibia, 1-3 cm below tuberosity on
5. After skin prep, places child in supine position and holds leg firmly 6. Directs and inserts needle perpendicular to bone using a boring or screwing motion
until needle “pops” into the bone marrow space (marked by sudden lack of resistance). Needle should stand alone.
7. Attempts aspiration of bone marrow to assist in placement confirmation. 8. Disconnects first syringe and connects second syringe, flushing with at least 3 ml
of normal saline, observing for fluid extravasation
9. After satisfactory flushing, attaches IV tubing and secures needle with sterile 2X2’s
10. Obtains a restraint order prn to prevent inadvertent dislodging of the needle. 11. States potential complications of IO cannulation and interventions.
2547 - Transcutaneous Pacing (TCP) Performance Criteria:
1. Indicated for adult patients with hemodynamically unstable bradycardia. 2. Is authorized as a standing order for paramedics in treating adult patients with
unstable bradycardia. Hemodynamically unstable bradycardia means a patient with a BP < 90, related to a bradycardic rhythm (HR <60) with serious signs and symptoms related to heart rate, (i.e.: chest pain, SOB, ALOC, shock, pulmonary congestion, CHF).
3. TCP should not be delayed for hemodynamically unstable bradycardia patients
while waiting for IV access or for atropine to take effect.
B. Contraindications: TCP is not authorized for use on patients less than 15 years of age.
Not authorized for hypothermic patients because the bradycardia is usually a physiologic response to the body temperature.
2548 – Needle Thoracostomy Performance Criteria:
2. Diminished or absent breath sounds on the affected side. 3. Possible tracheal deviation away from the affected side (late sign). 4. Shock syndrome (weak rapid pulse, hypertensive initially, with hypotension a late
6. Progressively worsening dyspnea/cyanosis.
1. Uses universal precautions. 2. States indications and possible complications of the procedure. 3. Assembles equipment and selects appropriate size needle and cannula. 4. Locates insertion site at the second intercostal space, mid-clavicular line or the
fourth intercostal space at the midaxillary line.
5. Prepare area with Betadine swap. 6. Firmly inserts the needle (attached to syringe) perpendicular to the chest wall, over
the top of the rib until pleura is penetrated as indicated by one or more of the following: a. A “popping sound” is heard, or giving away sensation is felt. b. A “hissing” noise follows evidence of a tension pneumothorax. c. Ability to aspirate free air or blood into the syringe.
7. Advances the catheter and removes needle and syringe. Adds flutter or Heimlich
Valve to prevent re-accumulation of air in the pleural space.
8. Secures needle hub in place with tape over Benzoin tincture or with other approved
9. Reassesses patient lung sounds, respiratory status immediately, and every five (5)
a. The procedure may have to be repeated if the tension is not relieved. b. Air transport: The needle thoracostomy should be done prior to takeoff to allow
for escape of air that may accumulate in the pleural space with atmospheric pressure changes.
2549 – Needle Cricothyrotomy Performance Criteria:
Transtracheal catheter ventilation is a temporary emergency procedure to provide oxygenation when airway obstruction cannot be relieved by other methods. A. Assessment/Treatment Indicators for the unconscious patient :
1. Patient is unconscious and unresponsive. 2. Total airway obstruction following unsuccessful attempts of BLS and ALS
3. Massive facial trauma in a patient who cannot be intubated by either oral or
4. Injury to the trachea/larynx in a patient who cannot adequately ventilated or
intubated by either oral or nasotracheal means.
1. With the high pressure used during ventilation and the possibility of air entrapment,
2. Hemorrhage may occur at the site of the needle insertion, especially if the thyroid is
3. Perforation of the esophagus. 4. Subcutaneous or meditational emphysema. 5. Usually does not allow enough ventilation to adequately eliminate carbon dioxide.
1. Uses universal precautions. 2. States indications and contraindications of procedure. 3. Locates and prepares insertion site at the cricothyroid membrane between the
4. Attaches the IV catheter to the syringe and inserts the needle midline at a 45°
angle with a quick smooth downward motion following the direction of the trachea. Applies negative pressure to the syringe during insertion. Entrance of air into the syringe indicates that the needle is in the trachea.
5. Advances the catheter over the needle, and withdraws the needle and syringe. If
using cricothyrotomy cannula, removes obturator. Attaches oxygen delivery device.
6. Assesses for hemorrhage or subcutaneous emphysema, which may indicate
7. Auscultates lungs while manually holding needle. 8. Secures needle hub in place with tape over Benzoin or with other approved device 9. Monitor end-tidal CO and/or pulse oximetry, and chest expansion
10. Document verification of needle placement 11. Contact Base Hospital if unable to adequately ventilate patient, and transport
immediately to closest hospital for airway management.
2552 – King Airway Performance Criteria:
1. Inability to ventilate in a setting in which endotracheal intubation is not successful
2. Inability of ALS personnel to ventilate or oxygenate the patient. 3. Inability of patient to protect the airway (coma, decreased level of consciousness
4. Cardiac arrest, including traumatic arrest. 5. Agonal or failing respirations, respiratory arrest. 6. Base Hospital Physician Order
1. Patient with GCS > 3 2. Patient has a gag reflex. 3. Patient has a tracheostomy or stoma. 4. Height less than 4 feet
1. Ingestion of caustic substance. 2. Known history of esophageal disease. 3. Inhalation
1. Uses universal precautions. 2. Assures an adequate BLS airway. 3. States indications and contraindications of King Airway. 4. States placement should be completed within 30 seconds. 5. Ensures suction is available and working.
6. Preoxyegnates with BVM for 2-5 minutes with supplemental oxygen when
7. States appropriate size tube based on height.
a. Size 3 – 4 and 5 feet tall b. Size 4 – 5 and 6 feet tall c. Size 5 – Over 6 feet tall
b. Lubricates device with water-soluble lubricant to the beveled distal tip and
posterior aspect of tube, taking care to avoid introduction of lubricant in or near ventilatory openings.
9. States will have a spare esophageal airway available for immediate use. 10. Positions the head. The ideal head position for insertion is the “sniffing position.” A
neutral position can also be used (e.g. spinal injury concerns).
11. Grasps the patient's tongue and jaw with gloved hand and pulls forward. A
laryngoscope may be used. With the King LTS-D rotated laterally at 45-90 degrees such that the blue orientation line is touching the corner of the mouth, introduces tip into mouth and advances it behind base of tongue. Never force the tube into position.
12. As the tube tip passes under tongue, rotates tube back to midline (blue orientation
13. Without exerting excessive force, advances tube until base of connector aligns with
14. Inflates cuff to required volume. States required cuff pressure based on tube size
a. Size 3 – 40 - 55 ml air b. Size 4 – 50 - 70 ml air c. Size 5 – 60 - 80 ml air
15. Connects the King LTS-D to a BVM and ventilates the patient. While ventilating
the patient, gently withdraws the tube until ventilation becomes easy and free flowing (large tidal volume with minimal airway pressure). Adjusts cuff inflation if necessary to obtain a seal of the airway at the peak ventilatory pressure employed.
16. Confirms proper position by auscultation, chest movement, and verification of CO2
by capnography. Do not use esophageal detector device with esophageal airway. The method of confirmation must be documented
17. Secures the tube. Notes depth marking on tube. 18. If placement is unsuccessful, removes tube, ventilate with BVM and repeats
sequence of steps. If unsuccessful on second attempt, BLS airway management shall be resumed.
19. Continues to monitor the patient for proper tube placement throughout prehospital
treatment and transport. Capnography should be done in all cases.
20. Provides ventilations at 10 – 12/minute. 21. Documents airway placement and results of monitoring throughout treatment and
22. The key to insertion is to get the distal tip of the airway around the corner in the
posterior pharynx, under the base of the tongue. It is important that the tip of the device is maintained at the midline. If the tip is placed or deflected laterally, it may enter the piriform fossa and cause the tube to appear to “bounce back” upon full insertion and release.
2553 – Endotracheal Intubation – Pediatric Performance Criteria:
In the absence of a protected airway, attempts to provide adequate lung inflation with a BVM may result in the generation of pharyngeal pressure high enough to cause gastric distention. In addition, gastric insufflation promotes regurgitation with the potential for aspiration of gastric contents into the lungs and may on occasion elevate the diaphragm enough to interfere with lung expansion. Pediatric intubation should only be attempted if an adequate BLS Airway cannot maintained. A. Assessment/Treatment Indicators:
1. Inability of ALS personnel to ventilate or oxygenate the patient. 2. Inability of patient to protect the airway (coma, decreased level of consciousness
3. Cardiac arrest, including traumatic arrest. 4. Agonal or failing respirations, respiratory arrest. 5. Base Hospital Physician Order
B. Contraindications: Intubation may be contraindicated on patients that are known
diabetics or narcotics overdoses, prior to the administration of Dextrose or Narcan.
3. Perforation or laceration of upper esophagus, vocal cords, larynx 4. Laryngospasm or bronchospasm 5. Dental and soft-tissue trauma 6. Aspiration
7. Dysrhythmias 8. Hypertension/Hypotension
1. Use universal precautions. 2. Assure an adequate BLS airway. 3. State indications and contraindications 4. States placement should be completed within 30 seconds. 5. Ensure suction and is available and working. 6. Checks light source, ensures a bright, tight, white light. 7. Select appropriate size tube. 8. Check tube cuff for leaks by injecting air into cuff with syringe and deflates cuff if
9. Position stylet (if used) so that the end is recessed within tube, then lubricates the
10. Instructs assistant to preoxyegnate the patient. 11. Positions the patient with neck slightly extended. Understands bimanual
laryngoscopy and when and how it is used.
12. Perform tube insertion. Gently inserts laryngoscope blade into mouth and applies
upward traction with left hand to visualize the vocal cords. Inserts tube through open cords with right hand when visualized. Does Not Use Teeth As A Fulcrum.
13. Remove laryngoscope from mouth and removes stylet while stabilizing tube
14. Inflate cuff (if present) with 10 ml of air and detaches syringe.
15. Simultaneously maintains tube position, ventilates patient and confirms tube
placement by: a. Notating capnography readings. b. Observing bilateral rise and fall of chest wall. c. Auscultating bilateral breath sounds with absence of sounds over abdomen. d. Confirm placement with end tidal CO2 device.
16. If initial attempt at intubation fails, reattempt after hyperventilation period of 15-30
17. If air was heard only on the right side, what would you do? (Indicates would deflate
the cuff, if present, pull tube back slightly -1 cm, re-inflate the cuff, and auscultate for bilateral air entry).
18. Note tube markers at front teeth, secures tube, and places oral airway. 19. Provide ventilations at 10 – 12/minute. 20. Successfully intubates in no more than two (2) attempts per patient with
hyperventilation between attempts. If unsuccessful after two (2) attempts, assure an adequate BLS airway.
2554 – Continuous Positive Airway Pressure (CPAP):
The goal of CPAP is to improve ventilation and oxygenation in an effort to avoid intubation in patients who present with severe respiratory distress. A. Assessment/Treatment Indicators: CPAP is authorized for use in patients who are age
8 or older with one of the following: 1. Congestive Heart Failure (CHF) with acute pulmonary edema 2. Near
3. Other causes of severe respiratory distress, excluding trauma
1. Respiratory or cardiac arrest 2. Failing
3. Inability to maintain airway 4. Severely depressed level of consciousness (LOC) 5. Systolic blood pressure < 90mmHg 6. Signs and symptoms of pneumothorax 7. Major trauma, especially head injury or suspected chest injury 8. Facial anomalies or inability to obtain a mask seal
2. Claustrophobia or unable to tolerate mask
1. Use universal precautions. 2. State indications and contraindications. 3. Position the patient in a seated position with legs dependant. 4. Apply cardiac monitor and assess vital signs. 5. Repeat vital signs every five minutes; SpO2 must be used to continuously monitor
6. Treat the patient according to appropriate treatment policy (i.e. pulmonary edema). 7. Set up the CPAP system following manufacturer directions.
8. Explain the procedure to the patient. It is important to reassure the patient
9. Verify that oxygen is flowing to the mask and then apply mask. 10. Do not exceed 10 cm of H20 pressure. 11. Continuously monitor patient for improvement or failure to improve. 12. The patient should improve in the first five minutes with CPAP, evidenced by
decreased heart rate and blood pressure, decreased respiratory rate and an increased SpO2.
13. If the patient does not improve or becomes worse with CPAP, remove the CPAP
device and assist ventilations with BVM as needed.
14. Notify the receiving hospital of the type of CPAP device that is being used 15. Documentation:
a. The use of CPAP must be documented on the patient care record. b. Vital signs to include heart rate, blood pressure, respiratory rate, and SpO2
c. Narrative documentation should include a description of the patient’s response
respond to CPAP and endotracheal intubation is required.
2560 – Paramedic Scope of Practice:
A. As part of the State approved expanded scope of practice, an accredited paramedic, as
part of the organized emergency medical services system in San Joaquin County, while caring for patients in a hospital as part of his/her training or continuing education under direct supervision of a physician, registered nurse, or physician assistant, or while at the scene of a medical emergency or during transport, or during interfacility transfer may perform the following procedures or administer the following medications in accordance with the written policies and procedure of the San Joaquin County EMS Agency: 1. Perform pediatric oral endotracheal intubation. 2. Perform adult naso-tracheal intubation. 3. Perform intraosseuos access. 4. Perform nasogastric intubation and gastric suctioning. 5. Perform transcutaneous cardiac pacing. 6. Monitor and adjust heparin infusion during interfacility transport. 7. Monitor and adjust nitroglycerine infusion during interfacility transport. Administer
using prepackaged products when available the following medications by the routes specified in the ALS treatment protocols: a. Magnesium
3410 – ALS Field to Hospital Communications:
A. ALS Initial Notification/Alert Report: Should be brief and last no longer than 20 to 30
seconds in duration. The purpose of the ALS Initial Notification/Alert Report is to provide the base or receiving hospital with notice to prepare for the patient. 1. ALS personnel should consider the use of this report format in the following
situations: a. Trauma, MCI, disaster, multiple patients, cardiac, or stroke alert activation if
warranted. During a MCI or disaster alert the number of patients should be given and their severity. Categorize the patients by utilizing START terms; “immediate”, “delayed, or “minor”.
life-threatening condition(s) that exist.
c. Patient report or transport or both will be delayed. d. Potential impact on emergency department operations such as the need for
decontamination or multiple patients in spinal precautions or categorized as delayed.
1. This report format is called into the base hospital regardless of patient destination. 2. Prehospital provider administering patient care must call this report to the base
3. If the patient destination is not the base hospital where the patient report was
called, it is the responsibility of the base hospital to provide a patient report to the receiving hospital where the patient is being transported.
4. “ALS Consultation”: When ALS standing orders have been implemented and/or
provider needs further direction/consultation or orders by a MICN or BHP. If no MICN or BHP is available, the paramedic will give an advisory report, and proceed with care under the provision of the ALS without Base Hospital Contact Policy No. 5310.
5. A Patient is refusing treatment (AMA), when in the field care provider’s judgment
the patient needs treatment and transport.
3411 – ALS Reporting Format:
A. Base Hospital Report or Consultation, May Receive Prehospital Report: MICN or Physician
Initial MCI Report Second MCI Report 4200 – Management of Controlled Substances:
1. ALS personnel shall only have access to controlled substances within their scope
of practice. BLS personnel may only have access to controlled substances while under the direct supervision of ALS personnel.
2. All controlled substances stored on the ALS vehicles shall be under double lock.
The keys to access narcotics shall be in the custody of the ALS personnel at all times.
3. Each ALS Provider shall maintain standardized written records of the controlled
substance inventory. These records shall be maintained by the ALS Provider for a minimum period of five years. Once completed, all drug inventory and administration records shall be maintained in accordance with State and Federal Law and Regulation. a. ALS personnel assigned to an ALS unit shall be responsible for maintaining the
correct daily inventory of controlled substances at all times.
b. All controlled substances shall be counted and inspected every time there is a
change in the ALS on-duty staff or at a minimum, once a shift.
c. Both the oncoming ALS personnel and the off-going ALS personnel shall jointly
count, date, time, and sign the standardized controlled substance inventory log.
4. Any discrepancies in the controlled substance count shall be reported to the ALS
Provider supervisor/management and the issuing agent. Discrepancies that cannot be immediately resolved shall be reported to local law enforcement and to the DEA using DEA Form 106 (Appendix A) referring to the theft or loss of controlled substances. A copy of the DEA report shall be submitted to the San Joaquin County EMS Agency along with an unusual occurrence report describing the incident and the ALS Provider’s actions and findings.
5. Controlled substance inventories and logs are subject to inspection by personnel of
the California Board of Pharmacy, Bureau of Narcotic Enforcement Administration, Federal Drug Enforcement Administration, and the San Joaquin County EMS Agency.
4102 – ALS Medical and Equipment Inventory:
A. Each ALS provider is responsible to develop a daily check out sheet, which shall list all
required items listed in this Policy. The provider shall develop an internal Policy that shall require that the attending paramedic complete the check out at the beginning of each shift.
B. The attending paramedic on each unit is responsible to ensure that all drugs and
equipment are present at the beginning of each shift, all equipment is functioning properly, and that all battery-powered devices are charged.
C. All ALS emergency ambulances, non-emergency ambulances, and non-transport units
shall be stocked and equipped as specified in this policy.
D. The quantities specified are minimum quantities except for controlled substances,
which are the maximum quantities allowed.
E. Expiration dates for medications and supplies must be current, as applicable. All
medications, supplies, and equipment shall be stored in accordance with the manufacturer’s recommendation.
F. In addition to the items listed below, all ambulances must meet the minimum
requirements set forth for ambulances in Title XIII of the California Code of Regulations.
4447 – EMS Aircraft Landing Sites:
A. The Incident Commander, or delegated Helispot Manager, should select an emergency
helispot using the following criteria: 1. Approach and departure angle of 6:1 (six feet horizontally for every foot of vertical
obstruction) day; 8:1 night. Ensure that approach, departure and landing area is clear of overhead obstructions such as wires, trees and light poles, etc. Consider prevailing winds.
2. Minimum size of 60 X 60 feet day, to 120 X 120 feet night. 3. The surface must be a firm, relatively flat surface, free of debris. All gravel, sand,
4. At night, a minimum of four flashing or steady burning lights should be used to mark
boundaries of the helispot. No lights should point in the direction of the aircraft.
B. The pilot in Command, after considering these limitations will have final authority to
decide if the helispot is acceptable for safe landing. The "Pilot in Command" of the air ambulance has ultimate authority to refuse to land at any site.
4448 – EMS Aircraft Utilization:
A. Do Not Utilize Ems Aircraft Transport For The Following Patients:
1. Cardiac arrest (in hypothermic arrest consider air transport). 2. Stable patient(s); i.e., fracture ankle, dislocated shoulder, etc. (consideration for air
transport may be given when the ground transport unit is greater than 30 minutes from a receiving facility).
3. Patient(s) contaminated by hazardous materials that cannot be completely
decontaminated prior to transport (e.g., possible nausea/vomiting of Hazardous Materials; eye wash or wound care necessary which has Hazardous Materials contaminant, etc).
4. Patient(s) who are agitated or combative and a potential threat to the crew. 5. Patient(s) located within any city limits. The only exception to this shall be if the
patient must be transported to a specialty care facility (i.e., trauma center, burn center, etc.) outside the city limits.
B. Patient Transport Criteria: Prior to requesting an EMS Aircraft a risk/benefit
1. Does this patient meet the clinical criteria to be transported by air? 2. Does air transport save at least 10 minutes over ground to the closest, most
3. Is air transport in the best interest of the patient? 4. Is air transport the safest way to transport the patient from the scene? 5. Is air transport the most appropriate mode of transportation?
Criteria: EMS Aircraft transport shall only be used when the patient(s) meet
a. Inaccessibility to the scene by ground personnel or equipment. b. Extended
a. Multi-casualty incidents (red or yellow priority patients). b. Critical trauma patients c. Spinal injury with neurological deficit. d. Unstable burn patient. e. Unstable patient from environmental injuries. f.
Vascular compromise in a limb or amputation.
g. Prolonged seizure refractory to medication or seizures involving pregnancy. h. Cardiovascular
Respiratory arrest or severe respiratory comprise.
Complications of childbirth (e.g., abnormal presentations, massive blood loss, etc.)
k. Pediatric Trauma (Refer to Pediatric Trauma Policy). l.
Any other conditions subject to approval of the Base Hospital Physician.
4980 – Receiving Hospital Diversion:
A. The diversion event may last no longer than three hours, at which time the receiving
hospital must go off diversion and remain off for at least twelve hours. A hospital may, with the approval of the EMS Agency Duty Officer, extend their diversion event beyond three (3) hours or request an additional diversion event during the twelve (12) hour period.
B. EMS Agency Duty Officer Initiated Diversion Event:
1. The San Joaquin County EMS Agency Duty Officer or authorized designee may
place a receiving hospital on diversion based one or more of the following:
2. One (1) or more emergency ambulances are waiting to transfer patient care
responsibilities to emergency department staff for more than one (1) hour.
3. Two (2) or more emergency ambulances are waiting to transfer patient care
responsibilities to emergency department staff for more than forty five (45) minutes.
4. Three (3) or more emergency ambulances are waiting to transfer patient care
responsibilities to emergency department staff for more than thirty (30) minutes.
5. Ambulance gurneys are being used by the emergency department to treat patients
6. EMS Duty Officer determines that such action is necessary to mitigate the capture
7. The three-hour diversion limitation may be exceeded if the EMS Agency Duty
Officer determines that such action is necessary to mitigate the capture of emergency ambulance services.
5102 – Patient Privacy:
A. “Imaging device” means any device capable of capturing and storing still or moving
images such as digital or other cameras, video cameras, cellular phones with picture taking or video recording capability, or any other devices with picture taking or video recording capability.
B. “Protected Health Information” (PHI) means any information related to the past,
present, or future physical or mental health or condition of an individual; the provision of health care to an individual; or the past, present, or future payment for the provision of health care to an individual. PHI includes information that may be oral or recorded and in any form or medium that is created or received by prehospital care personnel or an EMS provider. Protected health information (PHI) includes any individually identifiable health information. Identifiable refers not only to data that is explicitly linked to a particular individual (that's identified information). It also includes health information with data items, which reasonably could be expected to allow individual identification.
C. “Protected Personal Information” (PPI) shall include but not be limited to PHI, pictures
or other forms of voice or image recording, patient address, telephone numbers, social security number, date of birth, age, or any other information which could be used to uniquely identify the patient or that could result in identity theft if released for unauthorized purposes or to unauthorized personnel.
1. Patient privacy and confidentiality are fundamental expectations within the San
2. EMS personnel shall at all times protect the privacy and confidentiality of the
3. Possessing, releasing, or distributing protected personal information, including
protected health information other than for authorized purposes as part of an EMS organization’s permitted record keeping activities or uses is prohibited and may be a violation of the Health Insurance Portability and Accountability Act (HIPAA).
4. Permitted uses of PPI by EMS personnel and organizations include:
b. Continuous Quality Improvement (CQI) program activities; c. Patient
e. EMS Agency approved education, training, or research. f.
Prohibited activities and uses of PPI by EMS personnel and organizations include but are not limited to: 1) Any form of communication of PPI other than as permitted in Section IV of
this policy, including but not limited to: a) Verbal
b) PPI contained in email or other forms of written communication; c) Sharing of PPI on any website, blog, or other form of public
d) With the exception of permitted uses described in Section IV above,
the use of any imaging device while engaged in patient care, while at the scene of a medical emergency or hospital, or at anytime when such use could reasonably be expected to result in the capture of PPI.
5103 – Determination of Death in the Field:
A. Determining death prior to initiation of resuscitative measures:
1. If a patient meets criteria for obvious death upon an initial assessment EMS
personnel shall not initiate resuscitative measures including cardiopulmonary resuscitation (CPR) on the patient.
2. Obvious death is defined as a patient exhibiting apnea and pulselessness
accompanied by one or more of the following conditions: a. Decomposition of tissue; b. Decapitation; c. Rigor mortis and post mortem lividity characterized by rigidity or stiffening of
muscular tissues and joints in the body usually appearing in the head, face and neck muscles and the pooling of venous blood in dependent body parts;
e. Massive crush injury and/or penetrating injury with evisceration or total
destruction of the heart, lung, and/or brain;
B. EMS personnel are not required to use a cardiac monitor (i.e. “run a strip”) to confirm
C. Determining death after the initiation of resuscitative measures:
assessment does not reveal obvious death, EMS personnel
shall initiate treatment or resuscitative measures in accordance with applicable treatment protocols.
2. EMS personnel shall initiate rapid transport and continue resuscitation when the
following factors are present: a. The patient has a return of spontaneous circulation. b. Cardiac arrest occurred while under the care of EMS personnel. c. Bystanders used an automatic external defibrillator (AED) on the patient and
delivered a shock prior to arrival of EMS personnel.
d. Bystanders witnessed patient’s cardiac arrest and immediately started CPR
and continued to perform CPR until arrival of EMS personnel.
e. Traumatic cardiac arrest when the time from arrest to arrival at the closest
D. In the absence of factors requiring rapid transport, as identified in the paragraph above,
EMS personnel shall remain on scene and provide resuscitation to cardiac arrest patients.
E. If the patient remains pulseless and apneic following fifteen (15) minutes and five (5)
rounds of resuscitative measures ALS personnel shall contact the base hospital and request permission to discontinue resuscitative measures from the on-duty Base Hospital Physician (BHP). 1. ALS personnel shall confirm and document the patient’s cardiac rhythm in two (2)
electrocardiographic leads and provide evidence that the cardiac monitor is functioning properly (e.g. induced artifact due to manual compressions or pre-cordial thump.)
2. The attending paramedic shall attach a code summary from the electrocardiograph
3. The attending paramedic shall document the name of the BHP authorizing the
request for determination of death on the PCR.
F. Actions following a determination of death:
1. EMS personnel shall notify the law enforcement agency with jurisdiction following a
2. EMS personnel may not move or disturb a dead body until disposition has been
made by law enforcement or coroner representative.
3. EMS personnel shall leave in place all invasive therapeutic modalities initiated
during the resuscitation for the coroner’s review. These modalities may include but are not limited to advanced and basic airways, intravenous catheters, cardiac electrodes, etc.
4. EMS personnel shall not transport dead bodies by ambulance except in the
extremely rare occurrence that a patient is determined to be dead during transport. In such situations, EMS personnel shall deliver the body to the intended hospital.
5. If family or significant other request resuscitative efforts for a patient with obvious
death ALS and BLS personnel shall decline the request to initiate resuscitation and provide an explanation, reassurance and support to the family or significant other.
G. EMS personnel shall utilize S.T.A.R.T. guidelines in determining death at the scene of
multi-casualty incidents. As EMS resources become available patients initial determined to be dead per S.T.A.R.T may be re-assessed.
5105 – Do Not Resuscitate (DNR):
A. All patients whose initial assessment does not reveal “obvious death” as defined in
EMS Policy No. 5103 Determination of Death, shall be treated in accordance with applicable treatment protocols, unless the prehospital emergency medical care personnel are presented with a valid DNR order evidenced by one of the following: 1. A written and signed physician’s order in the patient’s medical record stating DNR; 2. A completed State of California Prehospital DNR Request Form; 3. A Medic Alert® bracelet inscribed “Do Not Resuscitate EMS”.
B. In the absence of a DNR order, if family members of an unconscious patient request
that resuscitative measures are not to be undertaken, prehospital emergency medical care personnel are to initiate appropriate basic life support treatment while contacting the Base Hospital for assistance and direction.
5106 – Interaction with Physician or Other Health Care Provider on Scene:
1. In the event that an unknown physician offers assistance on scene, ask the person
his/her name and request to see his/her State of California physician or surgeon’s license. If doubt about the person’s license request to see proof of identity, i.e. state driver’s license or identity card.
2. Pre-hospital personnel have the following responsibilities in the event that a
physician is on scene: a. Remain tactful, calm, and courteous. b. Provide the physician with a California Medical Association – EMS Authority
physician involvement on scene card (Appendix A) describing his/her options. EMS personnel should keep these cards readily available.
c. The identity of a physician shall be confirmed prior to EMS personnel
relinquishing responsibility for patient care.
d. Offer assistance to the physician on scene. The EMS provider cannot perform
orders given outside normal scope of practice as defined in the San Joaquin County EMS Treatment Protocols.
e. Maintain control of medications and equipment from the unit, and inform the
physician of drug and equipment availability.
Make initial contact with the base hospital physician (BHP), and communicate newly implemented plan for scene management.
B. An off-duty paramedic not accredited in San Joaquin County or not an employee of the
on scene ALS provider which provides proof of current paramedic licensure in California may at the discretion of the attending paramedic, and while under direct supervision provide assistance not to exceed the State’s basic paramedic scope of practice.
5107 – Use of Restraints:
A. The following forms of restraint shall NOT be used by prehospital personnel:
1. Hard plastic ties or any restraint device requiring a key to remove. 2. Sandwiching patients between backboards, scoop-stretchers, or flat, as a restraint. 3. Restraining a patient’s hands and feet behind the patient, i.e. hog-tying. 4. Methods or other materials applied in a manner that could cause respiratory,
vascular, or neurological compromise, including prone restraints.
B. Restrained extremities should be evaluated for pulse quality, capillary refill, color,
nerve, and motor function every 15 minutes. It is recognized that the evaluation of nerve and motor status requires patient cooperation, and thus may be difficult or impossible to monitor.
5108 – Care of Minors in the Field:
A. Parental consent is not required before initiating care or transport when:
1. The minor is emancipated. 2. The parent has given written authorization to procure medical care to any adult
over 18 years of age taking care of the minor.
3. A minor, 12 years or older, consents to the furnishing of hospital, medical and
surgical care related to treatment or diagnosis of infectious, contagious or communicable diseases.
4. A minor, living separate and apart from parent (for any period of time), managing
own economic affairs, regardless of source of income and regardless of whether parent(s), consented to separation. Parents are not liable for care provided pursuant to this section.
5. A minor, 12 years or older, is an alleged rape victim. 6. A minor, is a victim of a sexual assault (applies to both boys and girls and has no
7. A minor, seeks pregnancy prevention or treatment of pregnancy (does not include
8. A minor, 12 years or older, seeks medical or hospital care or counseling relating to
diagnosis and treatment of drug and alcohol related problem.
5110 – Anatomical Donor Cards:
A. “Imminent Death”: means for the purpose of this policy any situation in which illness in
the adult unconscious patient (18 years of age or older) are so severe that death is likely to occur prior to or shortly after the patient arrives at the hospital.
B. “Reasonable Search”: means for the purpose of this policy a brief, rapid search by law
enforcement, coroner, hospital, ambulance, or emergency medical personnel of an individual and his/her wallet/purse with the intention of locating an anatomical donor card attached to that individual’s driver’s license or state issued identification card.
C. If the patient is declared dead by law enforcement personnel or determined to be
obviously dead in accordance with EMS Policy No. 5103, ambulance or emergency medical personnel shall defer any search to coroner personnel.
5120 – Triage of Neonates and High Risk Pregnancy:
A. Pregnant patients with the following presentations are to be transported to designated
acute care hospital that meets additional criteria as specializing in the care of neonates and high risk pregnancies: 1. Pregnant patients who present with signs and symptoms of active labor and/or
vaginal bleeding and meet one or more of the following conditions: a. No history of prenatal care b. Gestational age from 20 to 33 weeks
2. Pregnant patients who are between 20-33 weeks pregnant and are suspected to
3. Any newborn who meets one or more of the following conditions:
a. Significant anoxia either prior to or during transport. b. Gestational age less than 33 weeks.
B. The following hospital(s) are designated as Neonatal Intensive Care Centers in San
Joaquin County: 1. San Joaquin General Hospital.
5121 – Neurological Triage Criteria:
A. Prehospital personnel shall assess all trauma patients using the following criteria and
are directed to transport patients meeting criteria to a designated neurological trauma receiving facility: 1. Glasgow Coma Scale Motor Score of 4 or less (not localizing to noxious stimuli). 2. Signs and symptoms of spinal cord injury (paraplegic/quadriplegic). 3. Major compound and/or penetrating head injury.
B. The following hospitals and trauma centers are designated or recognized as a
neurological trauma receiving center for San Joaquin County: 1. San Joaquin General Hospital; 2. University of California Davis Medical Center (level I trauma center); 3. Doctors Medical Center, Modesto (level II trauma center); 4. Memorial medical Center, Modesto (level II trauma center); 5. St. Joseph’s Medical Center, as an alternate destination when transport to San
Joaquin General Hospital or a trauma center is not feasible.
5122 – Pediatric Trauma Triage Criteria:
A. Patients with any one or more of the following, who are 14 years of age or less may be
transported to a designated Pediatric Trauma Center using the most expeditious method available: 1. Criteria for direct transport of pediatric trauma patients to a Pediatric Trauma
1) Initial systolic blood pressure (SBP) <90 (<80 if under 6 years of age) or
2) Requires advanced or continuous airway support; 3) Glasgow Coma Score (MOTOR) <5 (not localizing noxious stimuli).
1) Penetrating injuries to the head, neck, chest or torso, or penetrating injuries
proximal to the elbow and knee with vascular compromise;
2) Rib fractures causing flail chest; 3) Limb amputation or near amputation proximal to wrist/ankle. Burns - 20%
or more of the body surface area (15% or more if < age 10);
Injury: Crushing injury to head or torso (e.g., run over by a
2. Patients that meet the following criteria shall be transported to the closest
paramedic receiving facility: a. Pulseless and non breathing following trauma; b. Unstable or unmanageable airway.
3. Patients with any one or more of the following, who are 14 years of age or less,
after consultation with the base hospital physician, may be transported to a designated Pediatric Trauma Center using the most expeditious method available: a. Two or more proximal long bones (humerus, femur) fractures; b. Crush, degloved, or mangled extremity; c. High speed vehicular crashes with significant passenger space intrusion; d. Ejection from a moving vehicle (automobile, motorcycle, etc.); e. Vehicular crashes requiring extrication time of >20 minutes; f. Death in the same passenger compartment; g. Vehicular rollovers; h. Falls > 3 times the height of the child; i. Auto/pedestrian or auto/bicycle injury with >5 mph impact speed.
5130 – ALS Without Base Hospital Contact:
A. Upon completion of the call requiring ALS without base hospital contact ALS personnel
shall: 1. Determine the cause of the communications failure and report or replace faulty
2. Complete the ALS without Base Hospital Contact Report and submit the report to
their provider’s quality improvement coordinator before close of shift but no later than 24 hours after the occurrence.
3. The Provider’s quality improvement coordinator shall complete a review and submit
the ALS without Base Hospital Contact Report with their findings and a copy of the patient care report (PCR) to EMS Agency CQI Coordinator within 72 hours of the occurrence.
5506 – Spinal Immobilization:
Additionally, paramedics may discontinue or clear spinal immobilization initiated by BLS personnel, if in the opinion of the paramedic spinal immobilization is not warranted or may compromise patient care. Paramedics are required to document on the patient care record each instance of discontinuing spinal immobilization and the findings of their exam clearing the patient.
5561 – BLS Childbirth:
1. Assist mother with delivery, clean, preferably sterile technique 2. Control and guide delivery of neonate’s head and body 3. Check for cord around neck, gently slide over head if possible, if tight clamp and
cut to unwind and deliver neonate as quickly as possible
4. Suction neonates mouth and nose with bulb syringe 5. Clamp and cut umbilical cord 6. Dry and wrap neonate for warmth (especially the head); if possible place with
7. Note time of delivery and assess respirations, pulse rate and strength of crying 8. Perform neonatal resuscitation if needed. 9. Evaluate mother post delivery for evidence of shock due to excessive bleeding 10. Deliver placenta 11. Perform fundal message to help stop postpartum bleeding
1. Place mother in shock position, elevate hips with pillows, if possible place mother
2. If cord is present, assess cord for palpable pulse 3. If strong regular pulse is absent, gently insert gloved hand into vagina to relieve
4. Cover exposed cord with saline soaked dressing 5. Ensure ALS transport
5700 – ALS Treatment Policy – Introduction:
Base Hospital Physicians may order any medication or procedure within the paramedic scope of practice for any patient condition regardless of the treatment protocols. These orders are known as "Base Physician Orders" and physicians must issue these orders directly to paramedics via radio or telephone communication. MICNs may not relay a "Base Physician Order." Each "Base Hospital Order" must be documented on a Base Hospital Report Form and be submitted to the San Joaquin County EMS Agency for review. MICNs shall adhere to San Joaquin County EMS Agency Policies and Protocols when offering advice, guidance, and direction to ALS and BLS field personnel.
In order to facilitate the best possible delivery of prehospital emergency medical care attending paramedics have the right to speak directly to a Base Hospital Physician during any call.
5701 – Routine ALS Care:
A. Routine ALS Medical Care shall consist of the following:
1. Standard precautions 2. Provision of appropriate basic life support (BLS) care in accordance with EMS
3. ECG monitoring 4. IV access as indicated (may use saline lock when appropriate) 5. Obtain blood glucose level, as indicated 6. Transport
7. Follow ALS treatment protocols as indicated
5702 – ALS Advanced Airway Management:
A. “Attempt” is defined as the introduction of a laryngoscope blade past the patient’s teeth
B. Intubation in the pediatric patient should only be performed if unable to ventilate and
oxygenate the patient using two-person BVM ventilation. In cardiac arrest, oximetry will not be accurate, so intubation in this case should only occur if the patient cannot be ventilated by BVM.
1. Inability of the patient to protect the airway (coma, decreased level of
consciousness with non-intact gag reflex).
2. Inability of the ALS personnel to adequately ventilate or oxygenate the patient; 3. Cardiac arrest, including traumatic arrest. 4. Failing respirations (irregular and shallow), respiratory arrest.
a) No more than two (2) attempts per patient with preoxygenation and continuous
oximetry monitoring prior to each attempt.
b) An endotracheal tube inducer (ETTI) shall be used on all attempts. c) Each attempt should last no longer than 30 seconds. If during any attempt
patient desaturates below 90%, immediately cease and reventilate to increase saturation.
d) If patient has a Cormack-Lehane grade of 3 or 4 (epiglottis is not or is barely
visible), consider using the King Airway instead of oral endotracheal intubation as a first advanced airway attempt.
Cormack and Lehan Classification (Grades) of Difficult Laryngoscopy
Only posterior portion of glottis can be seen
Only epiglottis may be seen (none of glottis seen)
Neither epiglottis nor glottis can be seen
E. Nasal Intubation: Nasal tracheal intubation may only be performed with a base hospital
physician order. The base hospital physician name shall be documented on the PCR.
F. Advanced Airway Rescue Device (Combi-Tube or King Airway):
1. After two (2) unsuccessful attempts at endotracheal intubation, consider placement
2. The Combi-Tube comes in two sizes while the King Airway comes five (5) sizes.
Only the small adult size is permitted for the Combi-Tube.
3. The Combi-Tube or King Airway is not used in adults < 4 feet tall or children.
G. Paramedics shall reconfirm ET Tube placement prior to transferring patient care. H. Paramedics shall visualize the pharynx and vocal cords with the laryngoscope, if there
is any doubt as to proper placement of the endotracheal tube.
5707 – ALS Adult Pain Management:
A. The use of morphine to manage moderate to severe pain is an advanced life support
procedure that is indicated for patients who are complaining of moderate to severe pain in the presence of adequate vital signs and level of consciousness.
B. Morphine may be used to treat stable patients when extrication, movement, or transport
is required and is anticipated to cause considerable pain to the patient when there are no known contraindications to administering analgesia.
1. Perform routine ALS/BLS medical care as directed in EMS Policy No. 5502,
Routine BLS Care and EMS Policy No. 5701, Routine ALS Care.
2. Monitor patient closely. 3. Establish IV access (IV NS or NS lock as appropriate). 4. Obtain full set of vital signs. 5. Administer Morphine 2-4mg IV every five minutes as needed to relieve pain to a
maximum dose of 20mg. If unable to secure IV access, administer Morphine 5-10mg IM, may repeat one dose in 30 minutes. Document pain scale before and after medication administration.
6. Monitor patient and vital signs carefully; ensure patent airway. Do not administer
morphine sulfate for pain if systolic blood pressure is < 90 or respirations are < 12 without base hospital physician order.
1. Absolute: Allergy or sensitivity to the medication being administered. 2. Relative:
a. Nausea/Vomiting b. Altered level of consciousness c. Hypotension d. Suspected drug and/or alcohol intoxication e. Head
5711 – ALS Ventricular Fibrillation/Pulseless Vtach:
1. If unwitnessed arrest, perform and complete initial CPR sequence (5 cycles/2
2. Defibrillate patient one time using manufacturer recommended dose of energy
(usually 120-200 joules in biphasic defibrillators). If not stated, use 200 joules (biphasic); or 360 joules (monophasic); then resume CPR immediately.
CPR should be administered for complete sequences of 5 cycles/2 minutes,
between each shock. During 5 cycles/2 minutes, establish IV/IO and give Epinephrine during CPR (before or after shock).
4. Intubate and establish IV of normal saline TKO. 5. Administer
a. 1 mg (1:10,000) IV/IO. Repeat every 3-5 minutes b. If unable to establish IV/IO, may be given via ETT, 2 mg (1:1000) diluted in 10
6. Defibrillate 1 x @ 120 - 200 joules (biphasic); or 1 x @ 360 joules (monophasic);
7. Administer Lidocaine 1mg/kg IV (may repeat x 1 in 3-5 minutes). 8. For return of spontaneous circulation, see EMS Policy No.5726, Return of
9. If no return to spontaneous circulation continue CPR and follow appropriate rhythm
renal dialysis patients – Consider IV administration of
500 mg of 10% Calcium Chloride and 1 mEq/kg of Sodium Bicarbonate, consult Base Hospital Physician to discuss further management.
5712 – ALS Wide Complex Tachycardia with a Pulse:
A. Patients with Serious Signs and Symptoms (Chest Pain, BP < 90 systolic, decreased
LOC, shortness of breath, signs of shock): 1. Consult with base hospital physician.
precardioversion sedation with Midazolam 1-2 mg slow IV titrated to
b. Synchronized cardioversion at 100 joules (monophasic energy dose or
c. If no response: repeat synchronized cardioversion at 200 joules (or biphasic
d. If no response: repeat synchronized cardioversion at 300 joules (or biphasic
e. If no response: repeat synchronized cardioversion at 360 joules (or biphasic
If rhythm does not convert with cardioversion, administer Lidocaine 1 mg/kg IV (may repeat x 1 in 3-5 minutes).
2. Consult with base hospital physician for further pharmacotherapy.
B. Patients without Serious Signs and Symptoms:
2. Administer Lidocaine 1 mg/kg IV (may repeat x 1 in 3-5 minutes). 3. Consult with base hospital physician for further electrical or pharmacotherapy
5713 – ALS Narrow Complex Tachycardia: A-Fib/A-Flutter:
A. Patients with Serious Signs and Symptoms: Chest Pain, BP < 90 systolic, decreased
LOC, shortness of breath, signs of shock. 1. Consult base hospital physician.
precardioversion sedation with Midazolam 1-2 mg slow IV titrated to
b. Synchronized cardioversion at 100 joules (monophasic energy dose or
c. If no response: repeat synchronized cardioversion at 200 joules (or biphasic
d. If no response: repeat synchronized cardioversion at 300 joules (or biphasic
e. If no response: repeat synchronized cardioversion at 360 joules (or biphasic
5714 – ALS Narrow Complex Tachycardia; SVT:
A. Patients with Serious Signs and Symptoms (Chest Pain, BP < 90 systolic, decreased
LOC, shortness of breath, signs of shock): 1. Consider reversible causes of tachycardia such as hypoxia and hypovolemia. 2. Consult base hospital physician.
precardioversion sedation with Midazolam 1-2mg slow IV titrated to
b. Synchronized cardioversion at 100 joules monophasic energy dose (or
c. If no response: repeat synchronized cardioversion at 200 joules (or biphasic
d. If no response: repeat synchronized cardioversion at 300 joules (or biphasic
e. If no response: repeat synchronized cardioversion at 360 joules (or biphasic
B. Patients without Serious Signs and Symptoms:
1. Consider reversible causes of tachycardia including hypoxia and hypovolemia and
2. Perform Valsalva’s maneuver. 3. Administer Adenosine 6mg RAPID IV immediately followed by 20 ml of normal
4. If no response after 2 minutes: Administer Adenosine 12mg rapid IV immediately
5. If no response after 2 minutes: Administer Adenosine 12mg rapid IV immediately
6. Consider 12 Lead ECG if available. 7. Consult with base hospital physician.
5715 – ALS Asystole:
A. Consider reversible causes and treat as indicated:
1. Hypovolemia – Start two large bore IV lines and administer rapid 2 liter volume
infusion of NS, then 250 ml boluses until systolic BP is >90 mmHg .
2. Hypoxia – Administer 100% oxygen 3. Tension pneumothorax (Policy No. 2548, Needle Thoracostomy Policy). 4. IDDM and Dialysis (Acidosis) – Administer 1 mEq/kg of Sodium Bicarbonate IV 5. Cardiac tamponade – Continue CPR 6. Drug overdoses – Administer reversal agents as indicated. Contact base hospital
7. Hypothermia – Initiate rewarming activities. 8. Renal
(Hyperkalemia) - Administer 500 mg of 10% Calcium
Chloride and 1 mEq/kg of Sodium Bicarbonate IV
B. Administer Atropine 1 mg IV or 2 mg ETT, repeat every 3-5 minutes to a total of 3mg. C. Continue CPR for 5 cycles/2 minutes and recheck pulse/rhythm. D. Contact the Base Hospital for field determination of death if patient remains asystolic
after fifteen (15) minutes of continuous and appropriate advance cardiac life support (ACLS) intervention.
5716 – ALS Pulseless Electrical Activity (PEA):
A. Consider reversible causes and treat as indicated:
1. Hypovolemia – Start two large bore IV lines and administer rapid 2 liter volume
infusion of NS, then 250 ml boluses until systolic BP is >90 mmHg .
2. Hypoxia – Administer 100% oxygen 3. Tension pneumothorax (Policy No. 2548, Needle Thoracostomy). 4. IDDM and Dialysis( Acidosis) – Administer 1 mEq/kg of Sodium Bicarbonate IV 5. Cardiac tamponade – Continue CPR 6. Drug overdoses – Administer reversal agents as indicated. Contact base hospital
7. Hypothermia – Initiate rewarming interventions. 8. Renal
(Hyperkalemia) - Administer 500 mg of 10% Calcium
Chloride and 1 mEq/kg of Sodium Bicarbonate IV
B. Administer Epinephrine 1 mg (1:10,000) IV/IO or ETT 2 mg (1:1000) diluted in 10 ml of
5717 – ALS Bradydysrhythmias:
A. Patients with Serious Signs and Symptoms (systolic BP < 90, signs of shock,
decreased level of consciousness, chest pain, and shortness of breath): 1. May administer Atropine 0.5mg IV while preparing transcutaneous pacer. 2. Consult Base Hospital Physician.
a. Initiate transcutaneous pacing (Policy No. 2547, Transcutaneous Cardiac
Pacing) Repeat dose q 5 min. prn (max 3 mg).
b. Provide sedation with Midazolam 1-2 mg and/or Morphine Sulfate 1-2 mg slow
but patient remains symptomatic, consider fluid
challenges of 250 ml NS. Recheck vital signs every 250ml or more frequently as needed.
d. If inadequate response to Atropine and pacing, consider administering
Dopamine 400 mg/250 cc premix. Start at 10 mcg/kg/min and titrate to systolic blood pressure of 90. (See page 2 for Dopamine dosage chart).
5719 – ALS Acute Coronary Syndrome (ACS):
1. Oxygen 2. If systolic blood pressure is above 100 mmHg, administer nitroglycerin 0.4 mg SL -
may repeat every five (5) minutes if signs/symptoms persist and systolic blood pressure remains above 100 mmHg.
3. If patient is able to swallow, give Aspirin 325mg po. 4. Obtain 12 Lead ECG (Policy No. 2551, 12 Lead ECG) if available. 5. If systolic blood pressure remains above 100 mmHg, administer morphine sulfate
2-4 mg IV - may repeat in 2 mg doses as needed for pain control if systolic blood pressure remains above 100 mmHg.
6. If acute ST Elevation Myocardial infarction (STEMI) is detected on ECG:
Complete Prehospital Thrombolytic Checklist during transport
Consider establishing a second IV Normal Saline TKO during transport.
1. If systolic blood pressure less than 100 mmHg, administer a 250 cc fluid bolus. 2. If systolic blood pressure less than 90 mmHg, see Cardiogenic Shock protocol. 3. Nitroglycerin
NOT be administered to patients of either gender who have
taken Viagra, (sildenafil citrate) or Levitra (vardenafil HCL) within 24 hours or Cialis (tadalafil) within 36 hours.
4. Aspirin should NOT be administered to patients with aspirin allergy or active GI
5721 – ALS Hypertension:
1. Apply oxygen. 2. Obtain 12 Lead ECG if available. 3. Treat significant arrhythmias. 4. Consider IV access. 5. Treat associated syndromes. 6. Consult base hospital physician for patient in hypertensive crisis.
5724 – ALS Ventricular Ectopy:
1. Obtain 12 lead ECG, if available. 2. In the presence of continuous chest pain, administer Lidocaine 1mg/kg IV. 3. Consult Base Hospital if transport time may exceed 20 minutes.
5726 – ALS Return of Spontaneous Circulation (ROSC):
a. Monitor cardiac rhythm and vital signs b. If patient was resuscitated from VF/VT or ventricular ectopy is present consider
consulting base hospital physician for antiarrythmic infusion order.
a. Administer fluid challenge of 500ml IV. b. If pulse is < 60
1) Administer Atropine 0.5mg IV. Repeat every 5 minutes as needed
2) Initiate transcutaneous pacing (Policy No. 2547, Transcutaneous Cardiac
Pacing) if HR and BP not improved with Atropine.
c. Consider Dopamine infusion. Start at 5mcg/kg/min and titrate to systolic BP >
5731 – ALS Allergic Reaction/Anaphylaxis:
1. Remove allergen if possible. 2. Mild reaction (urticaria only):
3. Moderate to severe reaction (Urticaria with one or more of the following: swelling of
mucous membranes, dyspnea, wheezing, chest or throat tightness, abdominal cramps). a. Consider
1:1000, 0.01mg/kg SQ. Maximum dose 0.5mg. (Use with
caution in patients over the age of 35 years and in patients with known coronary artery disease or HTN.)
b. If wheezing, initiate hand held nebulizer dose of Albuterol 5mg in 6 ml NS.
c. Consider IV NS TKO or saline lock. d. Administer diphenhydramine 1mg/kg to maximum dose of 50mg IM or IV.
4. Anaphylaxis (Urticaria and signs of shock with any or all of the following: swelling of
mucous membranes, dyspnea, wheezing, chest or throat tightness, abdominal cramps). a. Administer
1:1000, 0.01mg/kg SQ. Maximum dose 0.5mg. (Use
with caution in patients over the age of 35 years and in patients with known coronary artery disease or HTN.)
b. Establish large bore IV of NS and administer 250ml fluid boluses as indicated. c. If wheezing, initiate hand held nebulizer dose of Albuterol 5mg in 6 ml NS.
d. Administer diphenhydramine 1mg/kg to maximum dose of 50mg IM or IV. e. Consider
If patient is unresponsive with no palpable pulses, administer epinephrine (1:10,000) 0.01mg/kg to max dose of 0.5mg IV.
g. Consult base hospital physician for further orders.
5733 – ALS Poisoning/Overdose:
1. Hydrocarbons (kerosene, gasoline, lighter fluid, turpentine, furniture polish, etc):
a. Do not induce vomiting-transport immediately.
3. Insecticides (organophosphates, carbonates):
a. Skin exposure: decontaminate patient as soon as possible (remove clothes,
c. Assess for SLUDGE (salivation, lacrimation, urination, diaphoresis/diarrhea,
gastric hypermotility, and emesis/eye [small pupils and/or blurry vision]).
d. If indicated, administer Atropine 2.0 mg I.V. slowly. If no tachycardia or pupil
dilation, give second dose of 2.0mg IV. Note: Atropine does not reverse muscle weakness that leads to respiratory failure.
e. Atropine can be toxic and repeat doses above 4 mg should be given by Base
a. IV NS TKO, start immediately. b. Anticipate rapid deterioration of condition. c. In the presence of life-threatening dysrhythmias:
1) Hyperventilate if assisting ventilation or if intubated. 2) Administer
d. For seizures, see EMS Policy, No. 5753, Seizures. e. For signs of shock, see EMS Policy No. 5720, Cardiogenic Shock.
a. IV NS TKO. b. Administer Diphenhydramine 1 mg/kg IV to a maximum of 50 mg. If unable to
a. Consider activated charcoal 1gm/kg PO, not to exceed 50gms given orally (if
within the first 60 minutes of ingestion).
b. Obtain blood glucose level. c. If bradycardic and/or hypotensive, consult base hospital physician for order to
a. Consider activated charcoal 1gm/kg PO, not to exceed 50gms given orally (if
within the first 60 minutes of ingestion).
b. If bradycardic and/or hypotensive, consult base hospital physician for order to
administer Calcium Chloride 500mg slow IV over 5 minutes. May repeat x 1 in ten minutes.
5736 – ALS Hypothermia:
A. Severe hypothermia (stuporous or comatose, dilated pupils, hypotensive or pulseless,
slowed to absent respirations): 1. Prepare to support ventilations using appropriate airway adjuncts. If spontaneous
respirations are present, intubate only if necessary to prevent aspiration or if ventilations are inadequate (4-6/min may be adequate).
2. Ventilate using warm, humidified oxygen if available. Avoid hyperventilating the
3. Observe for organized rhythm and pulses for one minute. If organized rhythm
present, move quickly but gently to warm environment (ambulance) and follow rhythm appropriate treatment protocol.
5738 – ALS Envenomation:
1. Refer to EMS Policy No. 5535, Basic Life Support Envenomation. 2. Insect
a. Scrape away stinger (if appropriate). b. Observe for Allergic Reaction/Anaphylaxis and treat accordingly (EMS Policy
c. Apply cold packs for pain management.
a. Immobilize extremity at or below heart level. b. Circle swelling and note time. c. Apply a light constricting band about 2" above and below the bite. The
purpose of constricting bands is to restrict lymphatic flow, not blood, so they should not be too tight. Check pulses below the bands and readjust the bands as necessary when they tighten due to swelling.
d. Consider pain management. e. Initiate early receiving hospital notification. f. Expedite
a. Apply ice to site. b. Make incisions over bite. c. Apply a tourniquet. d. Delay transport to initiate IV.
5751 – ALS Altered Level of Consciousness (ALOC):
1. Establish IV of normal saline and administer 10ml/kg bolus if signs of shock are
a. If blood sugar < 70 mg/dl, administer Dextrose 50% 25 GM’s IV. b. If unable to establish an IV, after a minimum of two attempts, may administer
c. Glucose paste may be administered if the patient is a known diabetic, can hold
head upright, can self-administer medication, and has an intact gag reflex.
3. If narcotic overdose is suspected, administer Naloxone 0.4mg-2mg IV titrated to
achieve effective respirations (maximum dose 4 mg).
4. If unable to obtain IV access, may administer Naloxone 2 mg IM. 5. Treat rhythm disturbances as appropriate.
5753 – ALS Seizures:
1. If witnessed by prehospital personnel to be seizing for > 2 minutes or patient has
two or more seizures without regaining consciousness; a. Administer Midazolam 2 mg slow IVP.
1) If unable to obtain vascular access, may administer IM. 2) May be repeated if necessary every five (5) minutes (total maximum dose
a. If glucose < 70mg/dl, administer Dextrose 50% 25Gms IV. b. If unable to establish IV, and blood sugar < 70 mg/dl may administer Glucagon
a. Administer Naloxone IV in 0.4 mg increments titrated to achieve effective
b. If unable to establish an IV and narcotic overdose suspected, may administer
4. For pregnant patients, treat as indicated for seizures per this policy and refer to
EMS Policy No. 5763, Severe Pre-Eclampsia/Eclampsia.
5754 – ALS Acute Stroke:
A. Assess patient using the Cincinnati Prehospital Stroke Scale (CPSS) and document
findings. The patient is considered a possible stroke if any of the tested signs/symptoms is positive.
5762 – ALS Vaginal Hemorrhage with Shock:
a. Start a large bore IV. Administer a NS fluid challenge of10 ml/kg. Recheck
b. Consider second large bore IV of NS. c. If post-partum and placenta delivered, perform fundal massage and put infant
5763 – ALS Severe Pre-Eclampsia/Eclampsia:
1. Position patient on left side. 2. Transport quickly with a quiet environment (no siren). 3. Initiate IV of NS at TKO rate (started while enroute to hospital). 4. Treat seizures according to EMS Policy No. 5753, Seizures. 5. Consult base hospital physician to obtain order for Magnesium Sulfate 2Gms slow
5764 – ALS Imminent Delivery:
A. Imminent Delivery: Regular contractions, bloody show, low back pain, feels like bearing
B. Breech Presentation: Presentation of buttocks or both feet. C. Limb Presentation: Presentation of single extremity.
5771 – ALS Bronchospasm:
a. Initiate nebulizer dose of Albuterol 2.5mg in 3 ml NS and Atrovent 0.5mg in 2.5
a. Assist ventilations with 100% oxygen and initiate an inline nebulizer treatment
of Albuterol 2.5 mg in 3 ml NS and Atrovent 0.5mg in 2.5 ml NS
b. Continue Albuterol 2.5 mg nebulizer/bag-valve-mask. c. Epinephrine 1:1000, 0.01 mg/kg SQ. Maximum dose 0.5 mg. (Use with caution
in patients over 35 years of age and in patients with coronary artery disease).
d. Consider CPAP (see EMS Policy No. 2554, Continuous Positive Airway
e. Ensure early receiving hospital notification
3. Breath actuated nebulizer should only be utilized with patient’s who have adequate
spontaneous respirations. Patients that require ventilatory support should have nebulized medications administered via standard nebulizer equipment.
5772 – ALS Acute Pulmonary Edema:
2. Initiate IV access. 3. Nitroglycerin 0.4 mg spray, repeat every 5 minutes if systolic blood pressure
4. Administer Furosemide 40 mg IV. If patient takes Furosemide regularly, give 80
5. If patient is in severe respiratory distress, consider CPAP (Policy No. 5906,
5774 – ALS Airway Obstruction:
A. If patient has signs of severe obstruction and/or is unconscious:
1. Continue abdominal and chest thrusts. 2. Assist ventilation with BVM. 3. Use direct laryngoscopy and Magill forceps to remove foreign body. 4. If unsuccessful, attempt endotracheal intubation. 5. If unsuccessful and unable to ventilate adequately with BVM, consider Needle
5781 – ALS Amputation:
1. When load and transport time is less than 20 minutes:
a. Place the amputated part in a sterile saline gauze wrap.
2. When load and transport time is more than 20 minutes:
a. Place the amputated part in a plastic container. Do not add ice or saline to the
container in which the amputated part has been placed.
b. Place that container in a second plastic container and then place on iced
saline. Ensure that there are two layers of protection between the amputated part and the iced saline.
5782 – ALS Burn Care:
A. Parkland Formula: Amount of IV fluid infused during the first 24 hours = weight in kg X
4 ml X % BSA burned. Administer one-half of the calculated fluid during the first 8 hours. Note: The starting time is considered the time at which the burn occurred and not the time at which medical care is initiated. To obtain an initial hourly infusion rate, use the following formula: (2ml x kg x % BSA)/8.
Example: 120kg male with 20% BSA burn = (2 x 120 x 20) / 8 = 600ml/hr infusion rate
5783 – ALS Major Trauma:
A. Do not delay transport. B. Treatment:
1. Secure airway using the simplest, effective method, while maintaining C-Spine
2. Establish 1-2 large bore IV(s) of normal saline on blood Y tubing.
a. If patient is hypotensive, administer NS wide open until systolic blood pressure
b. If systolic blood pressure remains < 90 after initial bolus, give 250 ml boluses
c. Reassess the patient after each bolus.
3. For pain management, in absence of hypotension and no narcotic allergies,
administer Morphine Sulfate per EMS Policy No. 5707, Adult Pain Management.
5784 – ALS Traumatic Arrest:
1. Secure airway using the simplest, effective method, while maintaining C-Spine
immobilization, if indicated. Consider intubation while en route.
2. Establish two large bore IV(s) of normal saline on blood Y tubing and infuse fluids
3. Monitor and treat dysrhythmias according to ALS treatment guidelines. 4. If blunt trauma arrest and patient is in asystole or pending difficult/prolonged
extrication, consult base hospital physician for determination of death order.
5. All patients that are in traumatic arrest that present with pulseless electrical activity
with an organized rhythm > 30 beats per minute shall be treated and transported without delay as a Major Trauma (EMS Policy No. 5783) patient.
5800 – Pediatric Routine Medical Care:
A. The defined age of a pediatric patient is 14 years old or less, and unless specified
otherwise, pediatric protocols should be used to treat these patients. (Note: An infant is considered to be < 1 year old. A child is considered to be > 1 year old.)
B. A pediatric length-based resuscitation tape will be used to determine drug doses, fluid
volumes, defibrillation settings, and equipment sizes. The tape is designed to estimate a child’s weight based on length (head to heel). The tape also includes information about abnormal vital signs.
5810 – Pediatric Pulseless Arrest Asystole/PEA:
1. Perform immediate, effective CPR. 2. Continue CPR, maintain patent airway with 100% oxygen via BVM. 3. Provide appropriate airway management. 4. Establish IV/IO access. Do not delay transport. If unable to obtain vascular
access, begin transport and continue efforts while en route.
5. Consider reversible causes and treat as indicated. 6. Administer Epinephrine 0.01 mg/kg (1:10,000) IV/IO, max of 1 mg. Repeat every
3-5 minutes. If unable to obtain vascular access, but successful with ETT, administer Epinephrine 0.1mg/kg (1:1000) via ETT followed by a 5ml NS flush.
7. Continue CPR for 5 cycles/2 minutes and recheck pulse/rhythm. 8. For PEA with a rate of 60 or less that is unresponsive to Epinephrine, administer
Atropine 0.02mg/kg IV or IO push. (Minimum dose is 0.1mg with maximum dose of 1mg.) May repeat once in 3-5 minutes if indicated.
9. An order to terminate resuscitation efforts may be given by the base hospital
physician for patients in Asystole that is unresponsive to treatment (See EMS Policy No. 5103, Determination of Death).
10. Note: CPR should be administered for complete sequences of 5 cycles/2 minutes.
During 5 cycles/2 minutes, establish IV/IO and administer medications during CPR to minimize interruptions in chest compressions.
5811 - Pediatric Pulseless Arrest Ventricular Fibrillation/Ventricular Tachycardia:
1. If unwitnessed arrest, perform and complete initial CPR sequence (5 cycles/2
2. Defibrillate patient one time at 2J/kg and then resume CPR immediately for 5
cycles/2 minutes (do not check rhythm or pulse after shock).
3. Check rhythm/pulse. If shockable rhythm, defibrillate 1 x @ 4J/kg and resume
4. Continue CPR for 5 cycles/2 minutes while performing appropriate airway
management. Prepare for and establish IV/IO access with as little interruption as possible in administration of CPR.
5. After 2 minutes of CPR, check pulse and rhythm. If no pulse, resume immediate
CPR and administer Epinephrine via IV/IO. a. 0.01 mg/kg IV/IO. Repeat every 3-5 minutes b. If unable to establish IV/IO, may be given via ETT, 0.1 mg (1:1000) follow with
6. After 2 minutes of CPR, check rhythm and if appropriate defibrillate at 4J/kg. 7. Resume and continue CPR for 5 cycles/2 minutes. 8. Administer Lidocaine 1mg/kg IV/IO (may repeat x 1 in 3-5 minutes). 9. After 2 minutes of CPR, check rhythm and if appropriate defibrillate at 4J/kg. If non
shockable rhythm present, treat according to appropriate protocol.
10. CPR should be administered for complete sequences of 5 cycles/2 minutes,
between each shock. During 5 cycles/2 minutes, establish IV/IO and administer medications during CPR (before or after shock) to minimize interruptions in chest compressions.
5812 – Pediatric Bradydysrhythmias:
1. Assure adequate oxygenation and ventilation. Most bradycardia in children is due
2. Check blood glucose. 3. Check temperature and begin warming if hypothermic. 4. Normal
a. Establish IV access. b. IV NS at TKO rate.
a. Obtain IV access. b. Administer a NS fluid bolus of 20ml/kg. c. Recheck vital signs. d. If patient remains bradycardic despite adequate oxygenation and ventilation,
administer Epinephrine 0.01mg/kg IV/IO (maximum dose of 1mg). If unable to establish IV/IO, administer Epinephrine 0.1mg/kg via ETT followed by a 5ml flush. May repeat epinephrine dose every 3-5 minutes as indicated.
e. If increased vagal tone or primary AV block present, administer Atropine
0.02mg/kg (Minimum dose 0.1mg and maximum dose 1mg). May repeat once.
If bradycardia remains, consult with base hospital physician and consider cardiac pacing.
5813 – Pediatric Tachycardia with Pulses:
1. Consider pediatric normal values for heart rate. Infants may have heart rates as
high as 220/min. and children may have heart rates as high as 180/min. in the presence of fever, anxiety, and/or pain.
2. Manage airway and ventilations as indicated. 3. Obtain vascular access. 4. Treat according to rhythm:
1) Consider and treat underlying cause (fever, pain, trauma, hypovolemia). 2) Consider fluid bolus of NS 20 ml/kg IV/IO. May repeat as indicated. 3) Recheck vital signs after each bolus. 4) If suspected trauma, refer to EMS Policy No. 5833, Pediatric Trauma.
a) Attempt vagal maneuver. b) If unsuccessful, administer Adenosine 0.1mg/kg rapid IV push
(maximum dose of 6 mg) followed by rapid 20ml flush of NS.
c) If unsuccessful, administer Adenosine 0.2mg/kg rapid IV push
(maximum dose of 12 mg) followed by rapid 20ml flush of NS.
b) Administer Adenosine 0.1mg/kg rapid IV push (maximum dose of 6mg)
followed by rapid 20ml flush of NS while setting up to perform cardioversion.
c) Consult base hospital physician for orders:
If responsive, administer Midazolam 0.05 mg/kg (maximum dose of 2mg) prior to cardioversion.
ii. Perform synchronized cardioversion at 1J/kg. iii. If no response, perform synchronized cardioversion at 2J/kg.
1) If no pulse refer to EMS Policy No. 5811, Pulseless Arrest: VFIB/VTACH. 2) Stable:
a) Administer Lidocaine 1mg/kg IV/IO. May repeat once in 3-5 minutes.
b) Administer Lidocaine 1 mg/kg IV/IO while setting up to perform
c) Consult base hospital physician for orders:
If responsive, administer Midazolam 0.05 mg/kg (maximum dose of 2 mg) prior to cardioversion.
Perform synchronized cardioversion at 1J/kg.
If no response, perform synchronized cardioversion at 2J/kg.
If no response, perform synchronized cardioversion at 4J/kg.
d) If cardioversion is successful, consult with base hospital physician for
5815 – Pediatric Apparent Life Threatening Event:
A. “Apparent Life Threatening Event (ALTE)” indicates an episode that is frightening to the
observer (may think the infant has died) and involves some combination of: 1. Apnea (central or obstructive) 2. Color change (cyanosis, pallor, erythema, plethora) 3. Marked change in muscle tone (limpness) 4. Choking or gagging
B. These events usually occur in infants < 12 months old, however, any child less than 2
years old who exhibits the symptoms listed above may be considered an ALTE.
1. Assume the history given is accurate. 2. Determine the severity, nature, and duration of the episode. 3. Obtain a medical history. 4. Perform a complete physical exam that includes the general appearance of the
child, skin color, extent of interaction with environment, and evidence of trauma.
5. If hypoglycemia suspected or ALOC, obtain glucose level. 6. Consider and treat any identifiable causes. 7. Transport patient to the hospital. 8. Note: Most patients will have a normal physical exam when assessed by
responding field personnel. Contact the Base Hospital Physician for consultation if the parent/guardian is refusing medical care and/or transport, prior to completing a Refusal of Care form.
5817 – Pediatric Airway Obstruction by Foreign Body:
1. Attempt to clear the airway using BLS maneuvers.
For infants administer back blows and chest thrusts.
For children > 1 year of age, administer abdominal thrusts.
2. If unable to clear foreign body, visualize the larynx and remove the foreign body
3. Assist ventilation with BVM and 100% oxygen. 4. If patient has a complete airway obstruction and you are unable to clear foreign
body using BLS maneuvers and direct visualization, consider Cricothyrotomy. Refer to EMS Policy No. 2549, Needle Cricothyrotomy for Complete Airway Obstruction.
5819 – Pediatric Respiratory : Stridor:
1. Place patient in position of comfort. 2. If suspected croup, consider saline nebulizer treatment. 3. If suspected epiglottis, do not attempt to visual airway. 4. Administer oxygen, allow parent to administer if appropriate. If patient deteriorates,
or becomes completely obstructed, attempt positive pressure ventilation via BVM.
5. Perform endotracheal intubation only if BVM ventilation is unsuccessful or
5820 – Pediatric Respiratory Distress: Bronchospasm:
A. “Mild Respiratory Distress” indicates mild wheezing, shortness of breath and/or cough.
B. “Moderate Respiratory Distress” indicates spontaneous breathing and adequate tidal
volume with significant wheezing/SOB accompanied by any of the following signs: accessory muscle use, nasal flaring, grunting, and/or inability to speak full sentences.
C. “Severe Respiratory Distress” indicates ineffective ventilations and/or inadequate tidal
volume, which may be accompanied by any of the following signs: accessory muscle use, cyanosis, inability to speak, gasping respirations, and/or decreased level of consciousness.
1. Place patient in position of comfort. 2. Administer oxygen, allow parent to administer if appropriate. 3. Treat according to severity:
1) Monitor heart rate, respiratory rate, and pulse oximetry. 2) Administer Albuterol 2.5mg in 3 ml NS via nebulizer. May repeat as
1) Monitor heart rate, respiratory rate, and pulse oximetry. 2) Administer Albuterol 2.5mg in 3 ml NS by nebulizer with Atrovent 0.5mg in
3) May repeat Albuterol as indicated. 4) Consider
epinephrine 0.01 mg/kg Sub-Q (Maximum dose is 0.3 mg).
1) Assist ventilations with BVM and 100% oxygen. 2) If unable to adequately oxygenate and ventilate patient, perform
3) Administer Albuterol 2.5mg in 3 ml NS and Atrovent 0.5mg in 3 ml NS by
nebulizer/BVM/ETT. May repeat Albuterol as indicated (not to exceed 20mg per hour).
4) Consider epinephrine 0.01 mg/kg Sub-Q (Maximum dose is 0.5mg).
5824 – Pediatric Shock:
A. “Shock” indicates inadequate tissue perfusion. Signs of shock include capillary refill
greater than 2 seconds, pallor, cool/clammy skin, hypotension, and altered level of consciousness.
1. Assure adequate oxygenation and ventilation. 2. Establish vascular access. 3. Administer rapid fluid bolus of NS 20 ml/kg. May repeat as indicated. 4. If suspected Cardiogenic Shock, consult with base hospital physician for Dopamine
5826 – Pediatric Allergic Reaction:
1. Remove allergen if possible. 2. Mild reaction (urticaria only):
a) Consider diphenhydramine 1 mg/kg IM (maximum of 50 mg).
3. Moderate to severe reaction (Urticaria with one or more of the following: swelling of
mucous membranes, dyspnea, wheezing, chest or throat tightness, abdominal cramps). a) Epinephrine
b) Administer diphenhydramine 1 mg/kg IM (maximum of 50 mg).
c) If wheezing, initiate hand held nebulizer dose of Albuterol 2.5mg in 3 ml NS.
4. Anaphylaxis (Urticaria and signs of shock with any or all of the following: swelling of
mucous membranes, dyspnea, wheezing, chest or throat tightness, abdominal cramps).
a) Epinephrine 1:1000, 0.01mg/kg SQ (maximum dose 0.3mg). b) Establish vascular access and administer NS fluid bolus of 20 ml/kg. May
c) If wheezing, administer Albuterol 2.5mg in 3 ml NS. May repeat as needed.
d) If patient is unresponsive with no palpable pulses, administer epinephrine
(1:10,000) 0.01mg/kg to max dose of 0.5mg IV and diphenhydramine 1mg/kg to maximum dose of 50mg IM or IVP.
f) Consult base hospital physician for further orders.
5828 – Pediatric Seizures:
A. Midazolam should not be given unless the patient is actively seizing (2 or more
seizures without regaining consciousness or a seizure that is witnessed by the EMT-P to last for longer than two minutes).
1. Protect from injury, do not restrain. 2. Initiate cooling measures if febrile.
3. If two or more generalized seizures occur without regaining consciousness or the
EMT-P observes seizure activity that lasts for two or more minutes:
a) Establish venous access. b) Evaluate blood glucose level. If blood glucose level is less than 60 refer to
EMS Policy No. 5829, Pediatric Altered Level of Consciousness. 1) If continued seizure activity, administer Midazolam 0.1mg/kg IV (maximum
2) For continued seizure activity not controlled by initial Midazolam dose,
consult base hospital physician for consideration of further Midazolam orders.
5829 – Pediatric Altered Level of Consciousness:
1. Initiate appropriate airway management. 2. Evaluate blood glucose level. If blood glucose level is less than 60, administer
a) Child older than two years of age – Dextrose 50 1ml/kg IV/IO b) Child less than two years of age – Dextrose 25% 2ml/kg IV/IO
c) Neonate – Dextrose 10% 3 ml/kg IV/IO
d) If unable to start IV, consult base hospital for order to administer Glucagon
3. If mental status and respiratory effort are depressed, administer Naloxone 0.4 mg -
2 mg IV/IO. Titrate in small increments to maintain adequate ventilation and airway control to a total initial dose of 2 mg.
4. If positive response to initial dose of Naloxone and strong suspicion of opiate
overdose, may repeat Naloxone dose one time only in five minutes.
5830 – Pediatric Poisoning/Overdose:
1. Insecticides (organophosphates, carbonates):
a) Decontaminate patient as soon as possible (remove clothes, wash skin). b) Avoid contamination of prehospital personnel.
c) Assess for SLUDGE (salivation, lacrimation, urination, diaphoresis/diarrhea,
gastric hypermotility, and emesis/eye [small pupils and/or blurry vision]).
d) If indicated, administer Atropine 0.05 mg/kg IV/IO slowly. May give second
dose of Atropine 0.05 mg/kg in 5 minutes if indicated (Maximum dose of 4mg).
e) If further doses of Atropine are required, consult the base hospital physician.
a) Anticipate rapid deterioration of condition. b) Consider activated charcoal 1gm/kg PO, not to exceed 50gms given orally (if
within the first 60 minutes of ingestion).
c) In the presence of life-threatening dysrhythmias or rapid deterioration:
1) Hyperventilate if assisting ventilation or if intubated. 2) Administer
d) For seizures, see EMS Policy, No. 5828, Pediatric Seizures.
a) Administer Diphenhydramine 1 mg/kg slow IV to a maximum of 50 mg. If
unable to establish IV access, administer IM.
a) Consider activated charcoal 1gm/kg PO, not to exceed 50gms given orally (if
within the first 60 minutes of ingestion).
a) Consider activated charcoal 1gm/kg PO, not to exceed 50gms given orally (if
within the first 60 minutes of ingestion).
b) If bradycardic and/or hypotensive, consult base hospital physician.
5833 – Pediatric Trauma:
1. Secure airway using the simplest, effective method, while maintaining C-Spine
2. Ensure adequate oxygenation and ventilation. 3. Control external bleeding. 4. Establish 1-2 large bore IV(s) of normal saline on blood Y tubing.
a) If patient has signs of shock, administer a fluid bolus of NS 20ml/kg. May
b) Reassess the patient after each bolus.
5. For pain management, in the absence of contraindications, administer Morphine
Sulfate per EMS Policy No. 5839, Pediatric Pain Management.
5837 – Pediatric Burns:
1. Assure adequate oxygenation and ventilation. 2. Administer high flow oxygen if inhalation injury is suspected. 3. Establish vascular access if indicated. 4. Monitor for dysrhythmias and treat as appropriate. 5. For major burns (greater than 10% TBSA), administer fluid bolus of NS 20 ml/kg.
6. For severe pain, refer to EMS Policy No. 5839, Pediatric Pain Management.
5839 – Pediatric Pain Management:
1. Perform routine ALS/BLS medical care as directed in EMS Policy No. 5502,
Routine BLS Care, EMS Policy No. 5701, Routine ALS Care, and EMS Policy No. 5800, Pediatric Routine Medical Care.
2. Monitor patient closely. 3. Establish IV access (IV NS or NS lock as appropriate). 4. Obtain full set of vital signs. 5. Administer Morphine 0.05mg/kg slow IV. May repeat once in five minutes. 6. If unable to secure IV access, administer Morphine 0.1mg/kg IM, may repeat one
5850 – Neonatal Resuscitation:
A. Resuscitation should be initiated on all premature infants who weigh 1 pound and are
1. Position Airway. 2. Suction mouth and nasopharynx with bulb syringe. 3. Dry and keep warm with dry towel or blanket. 4. Stimulate by drying vigorously including head and back. 5. Clamp and cut cord. 6. Evaluate respirations:
a) Mild distress - Administer blow by oxygen. b) Respiratory depression, failure, or gasping respirations – Assist ventilations
PHOTODYNAMIC TREATMENT (BLU LIGHT WITH LEVULAN) A procedure is now available that treats active acne as well as older acne leaving your skin smoother. The procedures are called Photodynamic Acne Treatments using Levulan. The Photodynamic Acne Treatment is a process by which a photosensitizing agent (Levulan) is applied to your skin. The Levulan is then activated with a specific wavelength
FÄRDIGHETSPROVET SOM BERÄTTIGAR TILL SKOGSBRUKETS NATURVÅRDSKORT Det här direktivet fastställer ramarna för hur provet för skogsbrukets naturvårdskort ska ordnas. Direktivets huvudmål är att garantera att proven ordnas på ett enhetligt sätt runtom i landet. Direktivet godkändes på det möte som ledningsgruppen för projektet höll 22.8.2008 och det är i kraft tillsvidare. Priset
 Table of Contents
Table of Contents 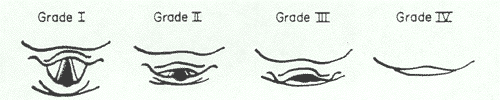 5701 – Routine ALS Care:
5701 – Routine ALS Care: