La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Microsoft word - muscular dystrophy.doc
Muscular dystrophy Introduction
Muscular dystrophy (MD) is a group of inherited muscle diseases in which muscle fibers are unusually susceptible to damage. Muscles, primarily voluntary muscles, become progressively weaker. In the late stages of muscular dystrophy, fat and connective tissue often replace muscle fibers. Some types of muscular dystrophy affect heart muscles, other involuntary muscles and other organs.
The most common types of muscular dystrophy appear to be due to a genetic deficiency of the muscle protein dystrophin.
There's no cure for muscular dystrophy, but medications and therapy can slow the course of the disease.
Signs and symptoms
Signs and symptoms vary according to the type of muscular dystrophy. In general, muscular dystrophy symptoms may include:
• Muscle weakness • Apparent lack of coordination • Progressive crippling, resulting in fixations (contractures) of the muscles around
Many specific signs and symptoms vary from among the different forms of MD. Each type is different in the age of onset, which parts of the body the symptoms primarily affect and how rapidly the disease progresses.
Dystrophinopathies These types of muscular dystrophies are due to a genetic defect of the protein dystrophin. Duchenne's muscular dystrophy is the most severe form of dystrophinopathy. It occurs mostly in young boys and is the most common form of MD that affects children. Signs and symptoms of Duchenne's MD may include:
• Frequent falls • Large calf muscles • Difficulty getting up from a lying or sitting position • Weakness in lower leg muscles, resulting in difficulty running and jumping • Waddling gait • Mild mental retardation, in some cases
Signs and symptoms of Duchenne's usually appear between the ages of 2 and 6. It first affects the muscles of the pelvis, upper arms and upper legs. By late childhood, most children with this form of muscular dystrophy are unable to walk. Most die by their late teens or early 20s, often from pneumonia, respiratory muscle weakness or cardiac complications. Some people with Duchenne's MD may exhibit curvature of their spine (scoliosis).
Becker's muscular dystrophy is a milder form of dystrophinopathy. It generally affects older boys and young men, and progresses more slowly, usually over several decades. Signs and symptoms of Becker's MD are similar to those of Duchenne's. The onset of the signs and symptoms is generally around age 11, but may not occur until the mid-20s or even later. Those affected by Becker's MD usually are able to walk through their teens, and often well into adulthood. Myotonic dystrophy Also known as Steinert's disease, this form of muscular dystrophy produces stiffness of muscles and an inability to relax muscles at will (myotonia), as well as the muscle weakness of the other forms of muscular dystrophy.
Although this form of MD can affect children, it often doesn't affect people until adulthood. It can vary greatly in its severity. Muscles may feel stiff after using them. Progression of this form of MD is slow. Besides myotonia, signs and symptoms of adult-onset myotonic dystrophy may include:
• Weakening of voluntary muscles that control your arms and legs, usually
beginning with the limb muscles farthest from the torso — the muscles of the feet, hands, lower legs and forearms.
• Weakening of head, neck and face muscles, which may result in the face having a
• Weakening of muscles involved in breathing and swallowing. Weaker breathing
muscles may result in less oxygen intake and fatigue. Weaker swallowing muscles increase the risk of choking.
• Fainting or dizziness, which may indicate that the disease is interfering with the
conduction of electrical signals that keep the heart rate normal.
• Weakening of muscles of hollow internal organs such as those in the digestive
tract and the uterus. Depending on which part of the digestive tract is affected, you may experience problems with swallowing as well as constipation and diarrhea. Weakness of the uterine walls may cause problems during childbirth.
• Difficulty sleeping well at night and daytime sleepiness, and inability to
concentrate because of the effect of the disease on the brain.
• Frontal balding in men. • Clouding of the lenses of the eyes (cataracts). • Mild diabetes.
Rarely, infants have this form of muscular dystrophy, in which case it's called congenital myotonic dystrophy. The infant form is more severe, although infants with myotonic dystrophy don't experience myotonia. Signs in infants may include:
• Severe muscle weakness • Difficulty sucking and swallowing • Difficulty breathing • Cognitive impairment
Facioscapulohumeral muscular dystrophy Also known as Landouzy-Dejerine dystrophy, this form involves progressive muscle weakness, usually in this order:
• Face • Shoulders • Abdomen • Feet • Upper arms • Pelvic area • Lower arms
When someone with facioscapulohumeral MD raises his or her arms, the shoulder blades may stick out like wings. Progression of this form is slow, with some spurts of rapidly increasing weakness. Onset usually occurs during the teen to early adult years.
Other major types of muscular dystrophy The other major types of muscular dystrophy include:
• Limb-girdle muscular dystrophy • Congenital muscular dystrophy • Oculopharyngeal muscular dystrophy • Distal muscular dystrophy • Emery-Dreifuss muscular dystrophy
Limb-girdle muscular dystrophy Muscles usually affected first by this form of muscular dystrophy include:
This form then progresses to the arms and legs, though progression is slow. Limb-girdle MD may begin from early childhood to adulthood.
Congenital muscular dystrophy Signs of congenital MD may include:
• General muscle weakness • Joint deformities
This form is apparent at birth and progresses slowly. More severe forms of congenital MDs may involve severe mental and speech problems as well as seizures.
Oculopharyngeal muscular dystrophy The first sign of this type of muscular dystrophy is usually drooping of the eyelids, followed by weakness of the muscles of the eye, face and throat, resulting in difficulty swallowing. Progression is slow. Signs and symptoms first appear in adulthood, usually in a person's 40s or 50s. Distal muscular dystrophy This group involves the muscles farthest away from the center of the body — those of the hands, forearms, feet and lower legs. The severity is generally less than for other forms of MD, and this form tends to progress slowly. Distal MD generally begins in adulthood between the ages of 40 and 60. Emery-Dreifuss muscular dystrophy This form of muscular dystrophy usually begins in the muscles of the:
Cardiac arrhythmias, stiffness of the spine and muscle contractures are other features of Emery-Dreifuss MD. Emery-Dreifuss MD usually begins in the childhood to early teen years and progresses slowly.
Muscular dystrophy is a general term for a group of inherited diseases involving a defective gene. Each form of muscular dystrophy is caused by a genetic mutation that's particular to that type of the disease. The most common types of muscular dystrophy appear to be due to a genetic deficiency of the muscle protein dystrophin.
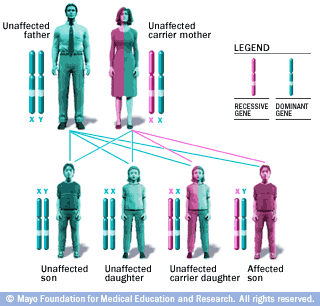
X-linked recessive inheritance pattern with carrier mother
Women can pass down X-linked recessive disorders such as Duchenne muscular dystrophy. A woman who is a carrier of an X-linked recessive disorder has a 25 percent chance of having an unaffected son, a 25 percent chance of having an affected son, a 25 percent chance of having an unaffected daughter and a 25 percent chance of having a daughter who also is a carrier.
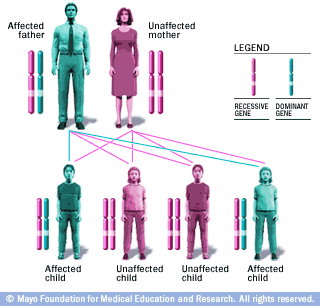
Autosomal dominant inheritance pattern
In an autosomal dominant disorder, the mutated gene is a dominant gene located on one of the nonsex chromosomes (autosomes). You only need one mutated gene to be affected by this type of disorder. A person with an autosomal dominant disorder — in this case, the father — has a 50 percent chance of having an affected child with one mutated gene (dominant gene) and a 50 percent chance of having an unaffected child with two normal genes (recessive genes).
Inheriting Duchenne's or Becker's MD Duchenne's and Becker's muscular dystrophies are passed from mother to son through one of the mother's genes in a pattern called X-linked recessive inheritance. Boys inherit an X chromosome from their mothers and a Y chromosome from their fathers. The X-Y combination makes them male. Girls inherit two X chromosomes, one from their mothers and one from their fathers. The X-X combination determines that they are female.
The defective gene that causes Duchenne's and Becker's muscular dystrophies is located on the X-chromosome. Women who have only one X-chromosome with the defective gene that causes these muscular dystrophies are carriers and sometimes develop heart muscle problems (cardiomyopathy) and mild muscle weakness. The disease can skip a generation until another son inherits the defective gene on the X-chromosome. In some cases of Duchenne's and Becker's muscular dystrophies, the disease arises from a new mutation in a gene rather than from an inherited defective gene.
Patterns differ for other types of MD Myotonic dystrophy is passed along in a pattern called autosomal dominant inheritance. If either parent carries the defective gene for myotonic dystrophy, there's a 50 percent chance the disorder will be passed along to a child.
Some of the less common types of muscular dystrophy are passed along in the same inheritance pattern that marks Duchenne's and Becker's muscular dystrophies. Other types of muscular dystrophy can be passed on from generation to generation and affect males and females equally. Still others require a defective gene from both parents.
When to seek medical advice
Duchenne's muscular dystrophy occurs almost exclusively in boys, although it can occur in girls. Your young child may have difficulty walking, running, rising from the floor or climbing the stairs, or may appear clumsy and fall often. These may be early indications of muscular dystrophy. A child with MD may learn to walk later than other children do and may exhibit signs of muscle weakness between the ages of 2 and 6. By school age, a
child with MD may walk unsteadily and on the toes or balls of the feet. Duchenne's MD usually results in children losing the ability to walk by age 12.
See your doctor if you're concerned about your child's:
• Motor abilities • Clumsiness • Muscle strength • Muscle development
Once muscular dystrophy is diagnosed, medications and physical therapy can help slow its progression.
Because muscular dystrophies are inherited disorders, genetic counseling may be helpful if you're considering having children and to assess the risk of the disease in other family members. Screening and diagnosis
A careful review of your family's history of muscle disease can help your doctor reach a diagnosis. In addition to a medical history review and physical examination, your doctor may rely on the following in diagnosing muscular dystrophy:
• Blood tests. Damaged muscles release enzymes such as creatine kinase (CK) into
your blood. High blood levels of CK suggest a muscle disease such as muscular dystrophy.
• Electromyography. A thin-needle electrode is inserted through your skin into the
muscle to be tested. Electrical activity is measured as you relax and as you gently tighten the muscle. Changes in the pattern of electrical activity can confirm a muscle disease. The distribution of the disease can be determined by testing different muscles.
• Ultrasonography. High-frequency sound waves are used to produce precise
images of tissues and structures within your body. An ultrasound is a noninvasive way of detecting certain muscle abnormalities, even in the early stages of the disease.
• Muscle biopsy. A small piece of muscle is taken for laboratory analysis. The
analysis distinguishes muscular dystrophies from other muscle diseases. Special tests can identify dystrophin and other markers associated with specific forms of muscular dystrophy.
• Genetic testing. Blood samples are examined for mutations in some of the genes
that cause different types of muscular dystrophy. For Duchenne's and Becker's muscular dystrophies, standard tests examine just the portions of the dystrophin gene responsible for most cases of these types of MD. These tests identify deletions or duplications on the dystrophin gene in about two-thirds of people with Duchenne's and Becker's MDs. The genetic defects responsible for Duchenne's and Becker's muscular dystrophies are harder to identify in other cases of those affected, but new tests that examine the entire dystrophin gene are making it possible to pinpoint tiny, less common mutations.
Treatment
There's currently no cure for any form of muscular dystrophy. Research into gene therapy may eventually provide treatment to stop the progression of some types of muscular dystrophy. Current treatment is designed to help prevent or reduce deformities in the joints and the spine and to allow people with MD to remain mobile as long as possible. Treatments may include various types of physical therapy, medications, assistive devices and surgery.
Physical therapy As muscular dystrophy progresses and muscles weaken, fixations (contractures) can develop in joints. Tendons can shorten, restricting the flexibility and mobility of joints. Contractures are uncomfortable and may affect the joints of your hands, feet, elbows, knees and hips.
One goal of physical therapy is to provide regular range-of-motion exercises to keep your joints as flexible as possible, delaying the progression of contractures, and reducing or delaying curvature of your spine. Using hot baths (hydrotherapy) also can help maintain range of motion in joints.
Medications Doctors prescribe medications to treat some forms of muscular dystrophy:
• Myotonic dystrophy. Medications that may be used to help manage the muscle
spasms, stiffness and weakness associated with this condition include mexiletine (Mexitil), phenytoin (Dilantin, Phenytek), baclofen, dantrolene (Dantrium) and carbamazepine (Tegretol, Carbatrol).
• Duchenne's muscular dystrophy. The anti-inflammatory corticosteroid
medication prednisone may help improve muscle strength and delay the progression of Duchenne's MD.
Assistive devices Braces can both provide support for weakened muscles of your hands and lower legs and help keep muscles and tendons stretched and flexible, slowing the progression of contractures. Other devices such as canes, walkers and wheelchairs can help maintain mobility and independence. If respiratory muscles become weakened, using a ventilator may become necessary. Surgery To release the contractures that may develop and that can position joints in painful ways, doctors can perform a tendon release surgery. This may be done to relieve tendons of your hip and knee and on the Achilles tendon at the back of your foot. Surgery may also be needed to correct curvature of the spine. Other treatments Because respiratory infections may become a problem in later stages of muscular
dystrophy, it's important to be vaccinated for pneumonia and to keep up-to-date with influenza shots.
Coping skills
For family members of people with muscular dystrophy, coping with the illness involves a major commitment of physical, emotional and financial effort. The disease presents challenges in the classroom, in the home and in all aspects of life.
In dealing with a disease such as muscular dystrophy, support groups can be a valuable part of a wider network of social support that includes health care professionals, family, friends and a place of religious worship.
Support groups bring together people, family and friends who are coping with the same kind of physical or mental health challenge. Support groups provide a setting in which people can share their common problems and provide ongoing support to one another.
Ask your doctor about self-help groups that may exist in your community. Your local health department, public library, telephone book and the Internet also may be good sources to locate a support group in your area.
By Mayo Clinic Staff, Dec 8, 2007 1998-2008 Mayo Foundation for Medical Education and Research (MFMER).
Source; http://www.mayoclinic.com/print/muscular-dystrophy/DS00200/D.#
March 2007 Trade Marks Registration in Respect of Therapeutic Goods in Australia The importance of selecting trade marks for therapeutic gthat are not likely to cause deception or confusion is illustrated by a number of recent Federal Court decisions. The Court in considering the issue of deception and confusion have looked at the reputation of the marks, any visual or oral similarity
Series Editor: Marie Boltz, PhD, APRN, BC, GNPManaging Editor: Sherry A. Greenberg, MSN, APRN, BC, GNPNew York University College of Nursing Fall Risk Assessment for Older Adults: The Hendrich II Fall Risk Model By: Deanna Gray-Miceli, DNSc, APRN, BC, FAANP, University of Pennsylvania; New Jersey Department of Health and Senior Services WHY : Falls among older adults, unlike other ages te
 X-linked recessive inheritance pattern with carrier mother
X-linked recessive inheritance pattern with carrier mother