La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Wellselling.at
Originalarbeit · Original Article
Forsch Komplementärmed Klass Naturheilkd 2001;8:373–382
Combined Herbal Preparation for Topical Treatment of Herpes labialis
a Departement für Innere Medizin, Naturheilkunde, Universitätsspital Zürichb Phytocon GmbH, Trogenc Churd brunner und hess software AG, Zürich
Key Words Schlüsselwörter
Rhubarb · Rheum sp. · Sage · Salvia officinalis ·
Rhabarber · Rheum sp. · Salvia officinalis · Salbei ·
Aciclovir · Herpes labialis · Clinical trial
Aciclovir · Herpes labialis · Klinische Studie
Zusammenfassung Background: The efficacy of many preparations for topical use Hintergrund: Die Wirksamkeit vieler bei Herpes-Infektionen lo-
in herpes infections have remained rather disappointing. The
kal angewendeter Präparate ist eher enttäuschend. Die Entwick-
development of new antiviral drugs, especially herbal prepara-
lung neuer antiviral wirksamer Medikamente und speziell auch
tions, thus remains desirable. In a screening study with plant
pflanzlicher Präparate ist deshalb nach wie vor wünschenswert.
extracts, a rhubarb root extract and a sage extract showed a
Ziel: Die Wirksamkeit eines topischen Kombinationspräparats
promising activity. Objective: The efficacy of a combined topi-
mit Rhabarber- und Salbeiextrakt, eines Monopräparates mit
cal preparation with rhubarb and sage extracts, of a single-
Salbeiextrakt sowie eines Referenzpräparats wurde mittels ei-
agent preparation with sage extract and of a reference treat-
ner komparativen randomisierten Doppelblindstudie unter-
ment was investigated in a double-blind, comparative, ran-
sucht. Patienten und Methoden: Insgesamt nahmen 149 Patien-
domised trial. Patients and Methods: A total of 149 patients
ten an der Studie teil. Die Daten von 145 Patienten (111 weibli-
participated, and 145 patients (111 female, 34 male) of whom
che und 34 männliche) konnten in die «Intention-to-treat»-Ana-
64 received the rhubarb-sage cream, 40 the sage cream and 41
lyse miteinbezogen werden. Davon erhielten 64 die Rhabarber-
Zovirax cream could be evaluated by intention-to-treat analy-
Salbeicreme, 40 die Salbeicreme und 41 die Zovirax-Creme.
sis. The dried rhubarb extract (23 mg/g) is a standardised aque-
Beim Rhabarber-Trockenextrakt (23 mg/g) handelt es sich um
ous-ethanolic extract according to the German Pharmacopoeia
einen eingestellten wässrig-ethanolischen Extrakt nach DAB
(DAB) with 4.0–6.0% hydroxyanthracene derivatives. The dried
mit 4,0–6,0% Hydroxyanthracen-Derivaten. Beim Salbei-Tro-
sage extract (23 mg/g) is an aqueous extract. The reference
ckenextrakt (23 mg/g) handelt es sich um einen wässrigen
product was Zovirax cream (Zovirax Creme) with the active in-
Extrakt. Als Referenzpräparat diente Zovirax® Creme mit dem
gredient aciclovir (50 mg/g). Results: The mean time to healing
Wirkstoff Aciclovir (50 mg/g). Ergebnisse: Die Heilungszeit aller
in all cured patients was 7.6 days with the sage cream, 6.7 days
geheilten Patienten betrug bei der Salbeicreme durchschnitt-
with the rhubarb-sage cream and 6.5 days with Zovirax cream.
lich 7,6 Tage, bei der Rhabarber-Salbeicreme 6,7 Tage und bei
There were statistically significant differences in the course of
der Zovirax-Creme 6,5 Tage. Im Verlauf der Symptome zeigten
the symptoms. For the parameter ‘swelling’, at the 1st follow-
sich statistisch signifikante Unterschiede. Für den Parameter
up visit there was a significant advantage for Zovirax cream
«Schwellungen» zeigte sich bei der 1. Kontrollvisite ein signifi-
compared to sage cream, and for the parameter ‘pain’, at the
kanter Vorteil für die Zovirax-Creme im Vergleich zur Salbeicre-
2nd follow-up visit there was a significant difference in favour
me. Bei der 2. Kontrollvisite zeigte sich ein signifikanter Unter-
of the rhubarb-sage cream compared to the sage cream. Con-
schied zugunsten der Rhabarber-Salbeicreme gegenüber der
clusion:
The combined topical sage-rhubarb preparation
Salbeicreme bezüglich dem Parameter «Schmerzen». Schluss-
proved to be as effective as topical aciclovir cream and tended
folgerung: Es konnte gezeigt werden, dass das topische Kombi-
to be more active than the sage cream.
nationspräparat ebenso wirksam wie die Zovirax-Creme und
tendenziell besser als die Salbeicreme ist.
Prof. Dr. Reinhard SallerDepartement für Innere Medizin
Naturheilkunde, Universitätsspital Zürich
Tel. +41 1 255-24 60, Fax -43 94E-mail rainhard.saller@dim.usz.ch
Introduction
Herpes simplex viruses are pathogenic to humans and causecommon infections throughout the world. Depending on thesite of infection, we speak of herpes labialis on the lips or her-pes genitalis in the anogenital area. Herpes simplex virusesare neurotropic, which means that after first infection theyspread through the skin or mucosa to the correspondingspinal ganglion and remain inactive there in the latent phase. As a result of various immune stresses they can be re-activat-ed at any time and trigger a characteristic herpes outbreakwith the formation of blisters and inflammation. Trigger ef-fects of this type may be: influenza, menstruation, UV chal-lenge, stress, dental treatment, surgery, excessive alcohol con-sumption, lack of sleep or generally weak immune defences. In Switzerland, antibodies to type I are found in more than90% of the adult population, and, depending on the social andsexual risk of transmission, antibodies to type II are found in20–60% of persons. Transmission is by direct contact with in-fectious material from the skin or mucosae. Primary infec-
Fig. 1. Patients’ flow. Visit 0 = inclusion visit, visit 1 = 1st follow-up visit;
tions with Herpes simplex generally have a troublesome
course, going as far as herpetic gingivostomatitis with type Iand painful ulcerous-oedematous vulvovaginitis with type II. Frequent complications of all herpetic eruptions are super-in-
in the aforementioned screening study. Sage leaves also have
fection with staphylococci, mycotic infection with Candida or
anti-inflammatory activity and, due to their tannin content,
herpetic eczema with neurodermatitis.
may be assumed to have a beneficial action on wound healing.
The early introduction of a systemic therapy with antimetabo-lites such as aciclovir shortly after the appearance of clinicalsymptoms is decisive for a successful therapeutic effect. Long-
Patients and Methods
term oral prophylaxis over months and years (especially
The Declaration of Helsinki and GCP (good clinical practice) rules were
against herpes genitalis) may be performed with low-dose an-
taken into account in the organisation and performance of the study. In
timetabolites. The actions of topical preparations have re-
addition, the approval of the Medical Ethics Committee of the Graubün-
mained rather disappointing. The development of newer an-
tiviral agents and especially those for topical use in herpes in-fections thus remains desirable just as before.
PatientsThe following inclusion and exclusion criteria were applied:
In a screening study with plant extracts, a rhubarb root extract
showed the most promising activity [1]. A prospective, ran-
domised, controlled, double-blind pilot study was therefore
– Diagnosis: recurrent herpes simplex labialis, unequivocally diagnosable
performed to investigate the efficacy and tolerability of a
in the vesicular phase or on appearance of the prodromal signs (itch-
cream with rhubarb extract [2]. A total of 66 patients partici-
ing, smarting, tension, pain) and according to the case history.
– The patients must be informed of the sense and purpose of the study
pated in the study, of whom 45 received rhubarb cream and 21
Zovirax cream (active ingredient aciclovir). The results of the
study showed no statistically significant difference between
– Any topical use of medicines in the affected area within the last 7 days
the two study products. A clear trend to a better action of
Zovirax cream was however seen for the first primary target
– Concomitant topical or systemic use of antiviral or immunomodulating
criterion, i.e. the healing time in all cured patients. The mean
– Known drug allergies or hypersensitivity to one of the active ingredi-
healing time was 6.5 ± 2.5 days (mean ± SD) in the Zovirax
ents (aciclovir, sage leaves, rhubarb root) or one of the excipients
group (n = 21) and 7.4 ± 3.2 days in the rhubarb group (n = 39)
(propylene glycol, lanolin, lauryl sulphate, methyl para-hydroxyben-
[2]. Due to the rather unsatisfactory results of this study, the
zoate (E 218), propyl para-hydroxybenzoate (E 216)).
study with rhubarb cream was interrupted after the first inter-
– Patients expected to show poor compliance. – Patients in whom delayed healing is possible (immune weakness, dia-
im evaluation, and a combined preparation with rhubarb and
sage extracts was developed for study. At the same time, a sin-
The clinical study enrolled 149 patients, and the results for 145 patients
gle-agent preparation with sage leaf extract was included in
(111 female and 34 male) could be evaluated. The patients’ flow is pre-
the study. An extract of this type also showed antiviral action
Forsch Komplementärmed Klass Naturheilkd
Table 1. Demographic distribution Table 2. Distribution of symptoms*
sage
*For statistical testing, the symptoms were re-coded into a new dichotomous variable that indicates whether a symptom is present or absent. 1 Comparison of all medications means all three medications are compared and tested for the two states of the symptom variables, resulting in a 2 × 3
2 Comparison medication 2 versus medication 3 means that two out of three medications are compared and tested for the two states of the symptom
variables, resulting in a 2 × 2 table. Data are only shown if they are significant without corrections for multiple testing. For Bonferroni correctionmultiply the p values by two.
3 Asymptotic 2-sided test. 4 2-sided test. p values without corrections for multiple testing. For Bonferroni correction multiply the p values by two.
Forsch Komplementärmed Klass Naturheilkd
Table 3. Efficacy and safety parameters
1. Time to complete disappearance of lesions (duration of therapy in days)
2. Time to drying and/or to start of crust formation (in days)
3. Clinical course of the symptoms (itching, smarting, tension, pain, swelling, erosion, diameter of largest lesion)
at time of each visit (inclusion, days 4–6, days 10–14)
5. Treatment failure: persistence of lesions at days 10–14
6. Appearance of complications, i.e. extension or scatter of lesions, or superinfection (e.g. impetigo) at days 10–14
*The evaluation was performed by the doctor (D) and the patient (P). The data for the individual symptoms was given in three steps (none, mild and
more severe). The judgement of efficacy and tolerability was given in three steps (good, moderate, unsatisfactory).
The three patient groups were comparable at the start of the study with
centration of 23 mg/g rhubarb extract for the cream is higher by a factor
regard to the following parameters: sex, age, diameter of the largest le-
of 102–103 than the concentrations that have proved to be antivirally ac-
sions, number of lesions, number of hours in the acute stage as well as
tive in vitro. The same concentration was chosen for the sage extract. This
symptoms at the time of the inclusion visit (itching, smarting, tension,
is in the same order of size as in the alcoholic extract that can be used
pain, blister formation, swelling, erosion, crust formation). With the ex-
undiluted, according to the Commission E monograph of 13.3.1990 [3],
ception of one symptom at the time of the inclusion visit, there were no
for painting on affected parts. Among other things, a virustatic and astrin-
significant differences with regard to the distribution of patients in the
three medication groups. The demographic data are presented in table 1.
At the start of the study it was determined that the creams should be in-
The symptoms at the time of the inclusion visit are presented in table 2.
vestigated by comparison with an established effective product. Compari-
The evaluation was performed on a dichotomous basis (no symptoms ver-
son with placebo was rejected for ethical reasons. According to the
sus mild and severe symptoms). At this time, blister formation was signifi-
knowledge at the time, Zovirax cream was the best product available.
cantly more marked in the rhubarb-sage group than in the Zovirax group.
The treatment regimen was established as follows: the inclusion visit (day
The study was performed in 8 study centres. These included a dermatolo-
0) should take place within 1 day after the appearance of prodromal signs.
gist, and six general practitioners in their own practices. The eighth study
The study medication should be rubbed in gently every 2–4 h while awake
centre was the Davos Dermatology and Allergy Clinic.
until the visit on day 10–14 or until the lesions were judged to be healed
In order to determine adverse effects, the investigating doctors ques-
by the doctor or the patient. The 1st follow-up visit took place between
tioned the patients during the two follow-up visits.
the 4th and 6th day and the 2nd follow-up visit between the 10th and 14th
The study medication was allocated to the patients according to a ran-
day. The symptoms were evaluated by questionnaires during the initial
domisation scheme developed by the statistician. Randomisation was un-
visit and during the two follow-up visits. In addition, the symptoms and
dertaken in a 1:1:1 ratio (Zovirax:sage:rhubarb-sage) in blocks of 6. After
the use of the medication were recorded in a patient diary.
an interim analysis, a new randomisation list was created with a 1:1:2 ratio
When dispensed, the study medications could not be distinguished one
(Zovirax:sage:rhubarb-sage) in blocks of 8.
from the other (labelled tubes with safety closure). Only after openingthe tube distinction was possible on the basis of colour. Since the patients
did not know which ‘chemical’ product served as the reference, even after
The dried rhubarb extract is a standardised aqueous-ethanolic extract ac-
opening their tube it was not possible for them to determine whether they
cording to the German Pharmacopoeia (DAB) with 4.0–6.0% hydroxyan-
had a ‘chemical’ or a ‘herbal’ preparation. Since the tubes were opened
thracene derivatives, calculated as rhein by reference to the dried extract.
only after the visit, it may be assumed that the investigating doctor also
This is obtained from the roots of Rheum palmatum L. and Rheum offici-
could not readily identify the study product.
nale BAILL. The dried sage extract is an aqueous extract obtained fromthe leaves of Salvia officinalis L. Rosemaric acid, an important con-
stituent of the labiate tannins, serves as the lead substance.
The aim of the study was to document the efficacy and tolerability of a
The study medicines were rhubarb-sage cream (23 mg/g rhubarb extract
cream based on rhubarb extract plus sage extract and of a cream based on
and 23 mg/g sage extract), sage cream (23 mg/g sage extract) and Zovirax
sage extract only in patients with labial herpes. This was a prospective,
cream (Zovirax® Creme, Glaxo Wellcome AG, Schönbühl, Switzerland;
multi-centre, randomised, double-blind trial that ran from 1996 to 1999.
50 mg/g aciclovir). The latter was purchased from a pharmaceutical
At least 80 cases with the most effective herbal cream and at least 40 cas-
es with Zovirax cream were planned. Since neither of the two herbal
The rhubarb extract concentration was chosen on the basis of the rhubarb
creams showed a clear advantage over the other at the time of the interim
extract concentration in Pyralvex (NORGINE Pharmazeutische Prä-
evaluation after 59 patients (sage cream 19, rhubarb-sage cream 21, Zovi-
parate GmbH, Marburg, Germany), a solution used for conditions of the
rax 19 patients), it was decided to enlarge the study as follows: sage and
oral mucosa and gingiva, as well as aphthae. Pyralvex contains 10 mg/ml
Zovirax cream at least an additional 20 patients, rhubarb-sage cream at
salicylic acid, and the rhubarb extract has an anthraquinone glycoside
least an additional 40 patients. The interim evaluation and the possibility
content corresponding 3 mg/ml. This concentration led to excessive
of an alteration of the randomisation were foreseen in the study protocol.
colouration of the cream and was therefore reduced. The selected con-
The efficacy and safety parameters are presented in table 3.
Forsch Komplementärmed Klass Naturheilkd
The parameters adopted are suitable for determining the course of labialherpes. They correspond to the symptoms usually recorded in clinicalstudies [e.g. 4–9]. In some studies [e.g. 4, 9] the virus load of the lesionswas also determined. This parameter was not adopted in this study sincethe criteria selected adequately describe the course of a relapse. External monitoring was performed to ensure the quality of the data. Inaddition, an investigators’ meeting was organised to train the participat-ing investigators at the start of the study. The study sponsor was ParsennProdukte AG, CH-7240 Küblis. Statistical MethodsAll data analyses were performed using SPSS for Windows 95/NT, re-lease 6.3 and 9.0 (SPSS Inc., Chicago, IL, USA). Continuous variables were presented by means of summary statistics. This refers to the number of patients with valid data (n), mean, median,minimum, maximum, SD. Categorical data were presented using absolute and relative frequenciesper category. To detect possible differences in the baseline characteristics between the
Fig. 2. Time to resolution of crusts.
treatment groups, data such as age, gender, symptoms, lesions and dura-tion of the infection were subjected to confirmatory statistics (chi-squaretest, analysis of variance (ANOVA), multinomial logistic regression). Todetect possible effects by centres, the parameters for time necessary up tothe point where the patient is cured, were additionally tested with anANOVA model with treatment, centre and their interactions as factors. In order to have centre sizes with 13–19 patients per centre, centres withlow number of patients were pooled for this purpose. An intention-to-treat (ITT) analysis was performed. All patients knownto have at least one application of the trial medication were included inthe ITT analysis.
The course of the study and the patient numbers are present-ed in figure 1. The data for 130 patients were available for theevaluation of time to healing. Data for 123 cases were avail-able for the evaluation of time to crust formation. The datafor 22 patients could not be used in this case since either therewas no crust formation or the diary was missing or not com-pleted by the patients. The mean time to crust formation was 7.8 days with the sagecream, 7.2 days with the rhubarb-sage cream and 6.3 days
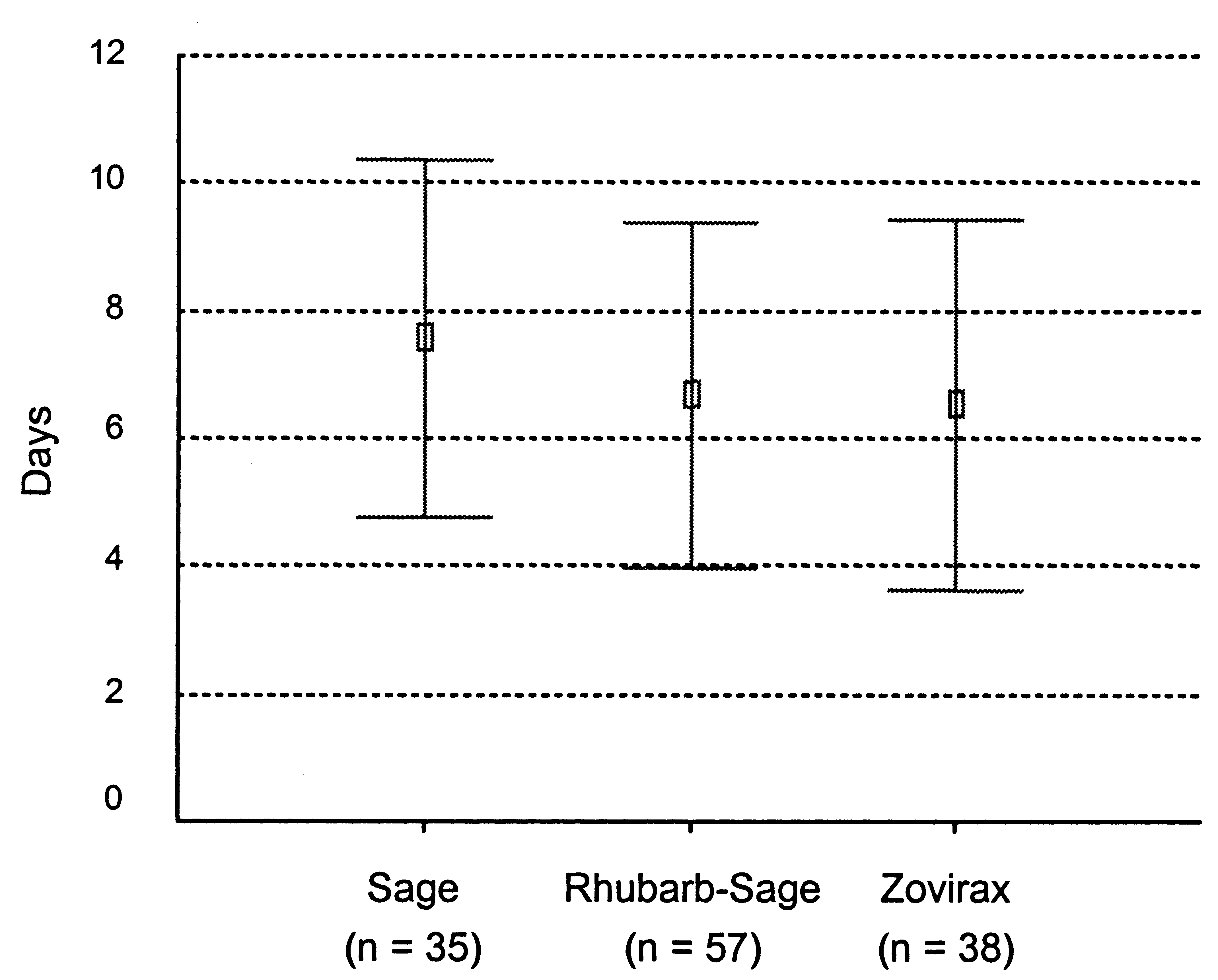
Fig. 3. Time to cure of patient
with Zovirax cream (fig. 2). The mean time to healing was 7.6days with the sage cream, 6.7 days with the rhubarb-sagecream and 6.5 days with Zovirax cream (fig. 3). Neither thetime to crust formation nor the time to healing differed signif-
Table 4. Statistical data for crust formation and healing
icantly between the treatment groups. The ANOVA- and
Bonferroni-corrected multiple test results are presented intable 4.
For comparison of the healing time, a Kaplan-Meier survival
analysis, including also those patients with missing data, was
performed, resulting in non-significant differences betweenthe three types of treatments (log rank statistic 2.02, p = 0.36).
If the non-inferiority margin for healing, the acceptable inferi-
ority between the plant extracts and aciclovir (Zovirax), is set
to 1.5 days, one would conclude non-inferiority for both
rhubarb-sage to aciclovir (Zovirax) and sage to aciclovir
(Zovirax). Similarly, with the non-inferiority margin for crust
Forsch Komplementärmed Klass Naturheilkd
formation set to 1.5 days, non-inferiority can be concluded for
significantly between the groups at the time of the 1st and 2nd
both plant extracts to acciclovir (Zovirax).
follow-up visits (tables 5 and 6). With the dichotomous com-
With one exception each time, the symptoms did not differ
parison of symptoms (no symptom versus mild to severe
Table 5. Course of symptoms: 1 st follow-up visit*
sage
*For statistical testing, the symptoms were re-coded into a new dichotomous variable that indicates whether either a symptoms is present or absent.
For patients where data was not available, the last observation was carried forward.
1 Comparison of all medications means all three medications are compared and tested for the two states of the symptom variables, resulting in a 2 × 3
2 Comparison medication 1 versus medication 3 means that two out of three medications are compared and tested for the two states of the symptom
variables, resulting in a 2 × 2 table. Data are only shown if they are significant without corrections for multiple testing. For Bonferroni correctionmultiply the p values by two.
3 Asymptotic 2-sided test. 4 2-sided test. p values without corrections for multiple testing. For Bonferroni correction multiply the p values by two. N.A. = Not analysed.
Forsch Komplementärmed Klass Naturheilkd
Table 6. Course of symptoms: 2nd follow-up visit*
sage
* For statistical testing, the symptoms were re-coded into a new dichotomous variable that indicates whether either a symptoms is present or absent.
For patients where data was not available, the last observation was carried forward.
1 Comparison of all medications means all three medications are compared and tested for the two states of the symptom variables, resulting in a 2 × 3
2 Comparison medication 1 versus medication 2 means that two out of three medications are compared and tested for the two states of the symptom
variables, resulting in a 2 × 2 table. Data are only shown if they are significant without corrections for multiple testing. For Bonferroni correctionmultiply the p values by two.
3 Asymptotic 2-sided test. 4 2-sided test. p values without corrections for multiple testing. For Bonferroni correction multiply the p values by two.
symptom), the values of the 1st follow-up visit showed that in
difference for the parameter ‘swelling’ remained significant.
relation to ‘burning’ and ‘burning’, healing was more ad-
At the 2nd follow-up visit there was a significant advantage
vanced in the Zovirax group than in the sage group. After
for the rhubarb-sage group compared to the sage group with
Bonferroni correction for multiple testing, however, only the
Forsch Komplementärmed Klass Naturheilkd
Table 7. Patients not
Not healed at the time of the 2nd follow-up with severe symptoms
Not healed at the time of the 2nd follow-up with mild symptoms
Table 8. Efficacy judgement Table 9. Safety judgement
For the course of symptoms from baseline to the 2nd follow-
between the rhubarb-sage group and the Zovirax group
up visit, the ‘area under the curve’ (AUC) was calculated by
also showed no statistical difference (Fisher’s exact test p =
assigning a score of 0 to the ‘no symptom’ level, a score of 1 to
the ‘mild symptom’ level and a score of 2 to the ‘severe symp-
Two patients had clinical super-infection: both were treated
tom’ level. Comparison of the AUCs for the three medication
with rhubarb-sage, and both presented the super-infection on-
groups revealed no significant differences between the treat-
ly at the 1st follow-up visit. In 1 case the super-infection was
not confirmed. Conclusive statistical analysis with only 2 cases
The results of the supplementary equivalence estimation by
the Mann-Whitney test (results not shown) show that the
With regard to the judgement of efficacy and safety by the
three preparations have comparable efficacy in relation to the
doctors and patients, no significant differences were found. In
any event, it happened that the efficacies of the rhubarb-sage
Judgement of the action of the study medication on the re-
cream and the Zovirax cream were judged to be roughly
lapse rate had to be renounced since a large number of pa-
equal by the doctors and patients and that the sage cream
tients were no longer available for further observation.
tended to be classed as somewhat poorer. With regard to tol-
149 patients were recruited. The 4 drop-outs concerned 2
erability, the patients estimated the rhubarb-sage cream and
protocol violations (no herpes labialis) and 2 patients who did
the Zovirax cream to be rather better than the sage cream.
not attend the follow-up visits (lost to follow-up). The follow-
The corresponding data are presented in the tables 8 and 9.
ing patients could not be taken into account in some respects
A survey of all adverse events observed (a total of 4 cases) is
in the ITT analysis: 4 patients due to withdrawal from the
study (Zovirax group: ‘severe depression’ and ‘insufficient
All adverse events could be classed as mild and transient.
efficacy’; Sage group: ‘infection became worse’ and ‘no
Medical treatment was not necessary, and the patients re-
healing’). In 1 case the withdrawal occurred between the 1st
and 2nd follow-up visits so that this patient could still be in-
Compliance and the degree of patient exposure were checked
cluded in the evaluation of symptoms at the 1st follow-up.
with the aid of the diaries and the consumed tubes of study
Another 11 patients were classed as not healed at the 2nd
medication returned. On average, each patient expressed
follow-up (day 10–14) (table 7). The distribution between the
about 1.2 g of study medication from the tubes and used the
three groups showed no significant differences. Comparison
study medication 4 times daily for 7.7 days.
Forsch Komplementärmed Klass Naturheilkd
Table 10. Adverse events
sage rhubarb-sage
Table 11. Placebo-controlled studies with
Zovirax cream
Discussion
Zovirax cream represents a reference product that has provedits worth in various placebo-controlled studies. These studies
The antiviral activity of rhubarb root extract observed during
show that healing is markedly faster with Zovirax cream than
screening was confirmed by the results of various published in
vitro antiviral studies with herpes virus and other coated
Evaluation of these 5 Zovirax studies shows an advantage of
viruses [10, 11]. Anthraquinones could be identified as the ac-
1.2 days in healing time for Zovirax cream compared to place-
tive constituents [11–16]. The somewhat weaker activity of
bo cream. The latest topical herpes remedy is Famvir (No-
sage leaf extract was also confirmed by various publications
vartis, East Hannover, NJ, USA) cream (active ingredient
penciclovir). For this product, a meticulous placebo-con-
The symptoms diminished to roughly the same extent be-
trolled double-blind study with over 2,000 patients showed an
tween the initial visit and the 1st and 2nd follow-up visits.
advantage of 0.7 days (p < 0.01) compared to a placebo cream
However, for the parameter ‘swelling’ there was a significant
advantage for Zovirax cream compared to sage cream at the
The present study is one of the first in which a herbal prepara-
1st follow-up visit (table 5), and for the parameter ‘pain’ there
tion has been investigated by comparison with aciclovir in the
was a significant difference in favour of the rhubarb-sage
indication of labial herpes. Only placebo-controlled studies
cream compared to the sage cream at the 2nd follow-up visit
with a cream containing melissa extract are known. In the lat-
est work [21], this product was investigated in a double-blind
With regard to treatment failures (table 7), it can be estab-
study with 66 patients. The primary target criterion was the
lished that the differences are not statistically significant. It is
comparison of a combined symptom score (pain, blisters, size
also true that the treatment failures presented only mild
of lesion) on the 2nd day of treatment. A barely significant
symptoms in the rhubarb-sage group, whereas all those in the
advantage (p = 0.042) was found for the reference product.
sage group still resulted in severe symptoms. In addition it has
Comparison of the symptom scores over 5 days showed no
to be considered that, in contrast to the sage and Zovirax
further significant differences between the two groups. This
groups, there were no drop-outs in the rhubarb-sage group
confirmed the results of an earlier study with 116 patients
[22], however, this was performed on patients with herpes
Although the significant differences in the courses of individ-
ual symptoms were not clinically relevant, the overall impres-
Current AIDS therapy shows that much better antiviral ac-
sion was that the Zovirax cream and the rhubarb-sage cream
tion can be obtained with combinations of several active sub-
do not differ and that the sage cream is somewhat less effec-
stances than with single substances. In this connection, the fol-
lowing pharmacological studies with herbal combination
Forsch Komplementärmed Klass Naturheilkd
products are of interest: It could be shown that a mixture of
treated with rhubarb cream had a healing time longer by 1.1
alcoholic extracts of Thymus serpyllum L., Viscum album L.,
days than patients treated with Zovirax cream. The present
Salvia officinalis L., Mentha piperita L. and Glycyrrhiza
study shows a healing time 1.2 days longer in the group of pa-
glabra L. markedly suppressed the multiplication of influenza
tients treated with sage cream compared to the aciclovir
viruses in vitro and in ovo, whereas the extracts of the single
(Zovirax) group. The combined rhubarb-sage preparation
drug plants had only moderate (Thymus serpyllum L. and
proved to be as effective as Zovirax cream in this study. The
Salvia officinalis L.) or no activities. Two other combination
difference in mean healing time was only 0.2 days in favour of
preparations showed similar results. The better activity of the
Zovirax cream. The non-significant (trend) superiority of the
combination preparations is attributed to synergistic interac-
rhubarb-sage cream over sage cream suggests that this is a
tion of the individual components [19].
worthwhile combination. Further pharmacological and clini-
In a previous study [2] it was found that a group of patients
cal studies are, however, desirable to quantify this advantage. References
1 Bossart W, Institut für medizinische Virologie der
9 Spruance SL, Rea TL, Thoming C, Tucker R, Saltz-
thraquinone derivates. Planta Med 1990;56:651–
Universität Zürich: Bericht über virologische Un-
man R, Boon R: Penciclovir cream for the treat-
tersuchungen. Interner Bericht. Küblis, Parsenn
ment of herpes simplex labialis. A randomized,
16 Barnard DL, Huffmann JH, Morris JLB, Wood SG,
multicenter, double-blind, placebo-controlled trial.
Hughes BG, Sidwell RW: Evaluation of the antivi-
2 Meyrat R, Büechi S: Studienbericht Rhabarber-
Topical Penciclovir Collaborative Study Group.
ral activity of anthraquinones, anthrones and an-
creme versus Zoviraxcreme. Interner Bericht.
thraquinone derivates against human cytome-
10 Taylor A, McKenna GF, Burlage HM, Stokes DM:
galiovirus. Antiviral Res 1992;17:63–77.
3 Monographie: Salviae folium. Bundesanzeiger 90,
Plant extracts tested against egg cultivated viruses.
17 May G, Willuhn G: Antivirale Wirkung wässriger
Tex Rept Biol Med 1954;12:551–557.
Pflanzenextrakte in Gewebekulturen. Arzneimit-
4 Spruance SL, Schnipper LE, Overall JC Jr, Kern
11 Sydiskis RJ, Owen DG, Lohr JL, Rosler KHA,
ER, Wester B, Modlin J, Wenerstrom G, Burton C,
Blomster RN: Inactivation of enveloped viruses by
18 Kaji-a-Kamb M, Amoros M, Girre L: Search for
Arndt KA, Chiu GL, Crumpacker CS: Treatment
anthraquinones extracted from plants. Antimicrob
new antiviral agents of plant origin. Pharm Acta
of herpes simplex labialis with topical acyclovir in
Agents Chemother 1991;35:2463–2466.
polyethylene glycol. J Infect Dis 1982;146:85–90.
12 Schinazi RF, Chu CK, Babu JR, Oswald BJ, Saal-
19 Serkedjieva J: Inhibition of influenza virus repro-
5 Van Vloten WA, Swart RN, Pot F: Topical acy-
mann V, Cannon DL, Eriksson BFH, Nasr M: An-
duction by combined preparation of medicinal
clovir therapy in patients with recurrent orofacial
thraquinones as a new class of antiviral agents
plants. Antiviral Res 1994;23(suppl 1):136.
herpes simplex infections. J Antimicrob Chemo-
against human immundeficiency virus. Antiviral
20 Kingsley S, Yeo JM, Fiddian AP, Nebout T,
Hantzperg M: Failure of acyclovir cream in treat-
6 Fiddian AP, Yeo JM, Stubbings R, Dean D: Suc-
13 Cohen PA, Hudson JB, Towers GHN: Antiviral ac-
ment of recurrent herpes labialis (letter). BMJ
cessful treatment of herpes labialis with topical
tivities of anthraquinones, bianthrones and hyper-
acyclovir. BMJ (Clin Res Ed) 1983;286:1699–1701.
21 Koytchev R; Alken RG; Dundarov S: Balm mint
7 Shaw M, King M, Best JM, Banatvala JE, Gibson
extract (Lo-701) for topical treatment of recurring
JR, Klaber MR: Failure of acyclovir cream in treat-
14 Andersen DO, Weber ND, Wood SG, Hughes BG,
herpes labialis. Phytomedicine 1999;6:225–230.
ment of recurrent herpes labialis. BMJ (Clin Res
Murray BK, North J-A: In vitro virucidal activity
22 Vogt HJ, Tausch I, Wöbling RH, Kaiser PM: Melis-
of selected anthraquinones and anthraquinone de-
senextrakt bei Herpes simplex. Allgemeinarzt
rivates. Antiviral Res 1991;16:185–196.
Samuels S: Herpes labialis treatment with acyclovir
15 Wood S, Huffman J, Weber N, Andersen D, North
5% modified aqueous cream: A double-blind ran-
J, Murray B, Sidwell R, Hughes B: Antiviral activi-
domized trial. Oral Surg Oral Med Oral Pathol
ty of naturally occurring anthraquinones and an-
Forsch Komplementärmed Klass Naturheilkd
Dear Partner and Friends of the International Chapel of Vienna, We have committed to providing more transparency in what we do as elders and to inform you as partners and friends of the issues that lye before us. One of the ways that we can accomplish this is to provide you with monthly updates. We are hoping that you find these informative as we work together to serve you. We have me
technical post-balance sheet eventsrelevant to Professional Scheme Paper 3.1 Candidates attempting Paper 3.1 should CASE STUDY following issues arising during the final audit find Question 3 relatively straightforward, as By way of a case study, consider Question 3 of have been noted on a schedule of points for its style and standard have barely changed the June 2005 exam. Th

 Originalarbeit · Original Article
Originalarbeit · Original Article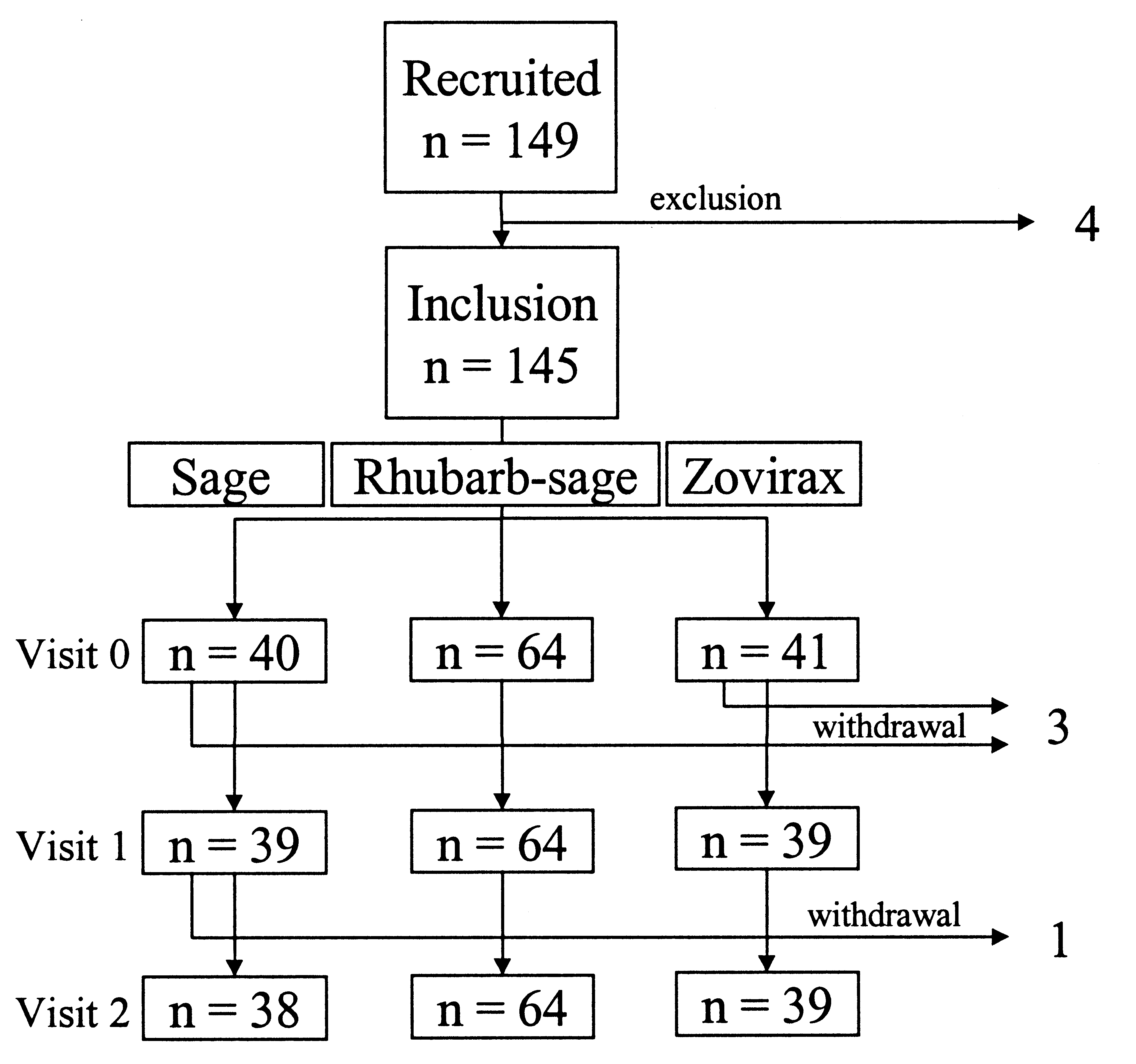 Introduction
Introduction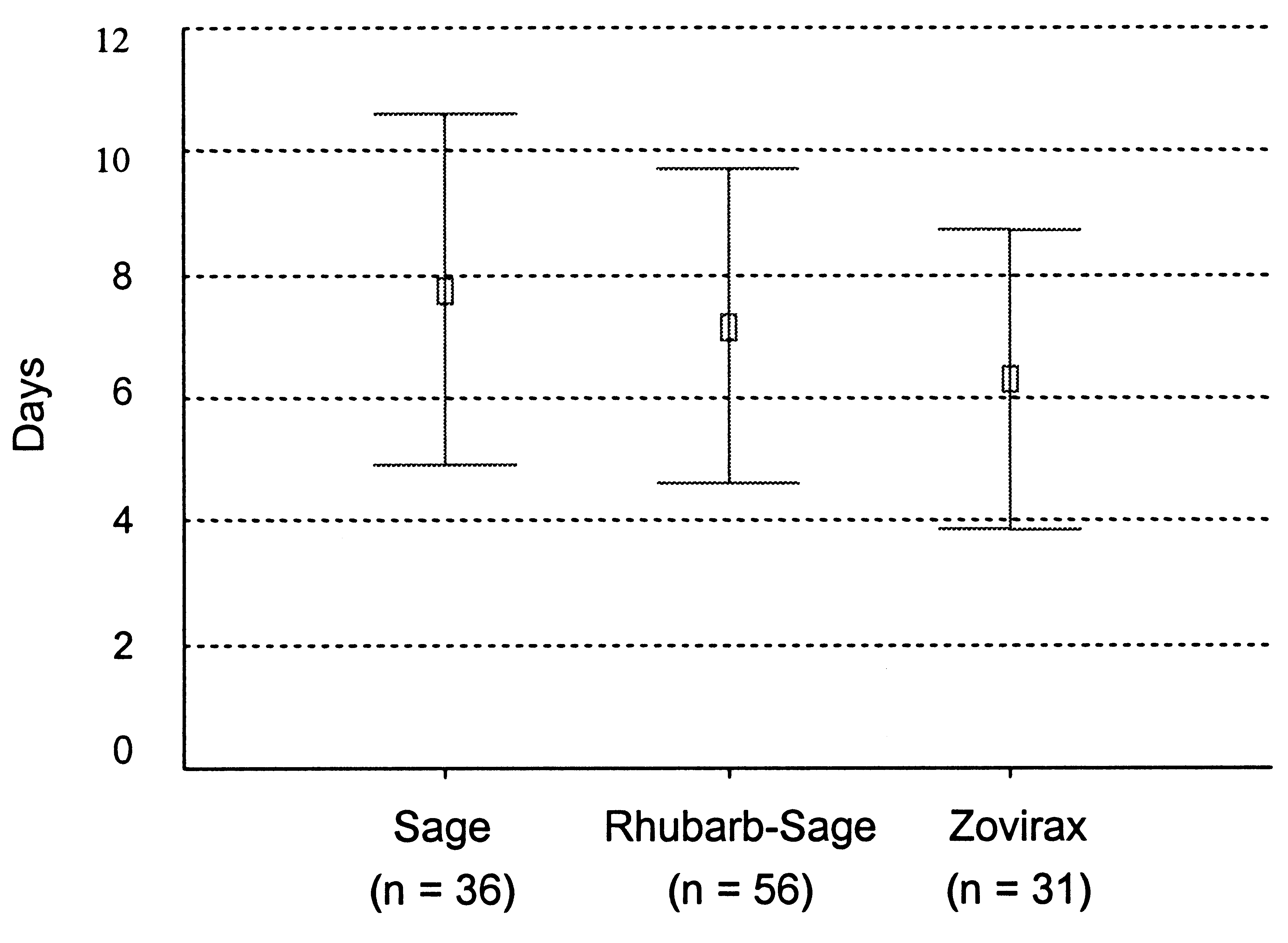
 The parameters adopted are suitable for determining the course of labialherpes. They correspond to the symptoms usually recorded in clinicalstudies [e.g. 4–9]. In some studies [e.g. 4, 9] the virus load of the lesionswas also determined. This parameter was not adopted in this study sincethe criteria selected adequately describe the course of a relapse. External monitoring was performed to ensure the quality of the data. Inaddition, an investigators’ meeting was organised to train the participat-ing investigators at the start of the study. The study sponsor was ParsennProdukte AG, CH-7240 Küblis.
The parameters adopted are suitable for determining the course of labialherpes. They correspond to the symptoms usually recorded in clinicalstudies [e.g. 4–9]. In some studies [e.g. 4, 9] the virus load of the lesionswas also determined. This parameter was not adopted in this study sincethe criteria selected adequately describe the course of a relapse. External monitoring was performed to ensure the quality of the data. Inaddition, an investigators’ meeting was organised to train the participat-ing investigators at the start of the study. The study sponsor was ParsennProdukte AG, CH-7240 Küblis.