La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Microsoft word - patient intake form2.doc
6410 Rockledge Drive, Suite 110, Bethesda, MD, 20817 (O) 301.530.7303 (F) 301.530.7312 2112 F Street, NW, Suite 802A, Washington, DC, 20037 (O) 202.775.7246 (F) 202.775.2345 NAME: ____________________________________________ DATE: ____________
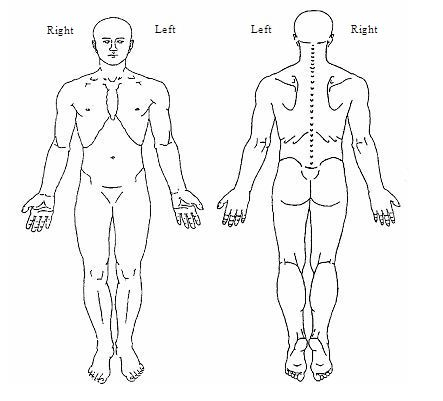
Home Phone: ____________________ Work Phone: _______________________ Cell Phone: ______________________ Who to call in case of emergency: ___________ Name of the doctor who has referred you: _____________________________________ Names of doctors who should get this report: ___________________________________ REASON FOR VISIT: ___________________________________________________ The worst area(s) of pain: __________________________________________________ Please mark the areas of pain Please rate your average daily pain: from 0 (no pain) to 10 (worst possible pain): /10 Length of time that you have had this pain in this area: ________________________ Has something or an event started your pain? YES NO If so what event? ________________________________________________________________________ Circle factors that aggravate your pain? None Standing Exercising Walking Bending Straining Lifting Stress Weather changes Medications Repetitive motions Sitting Head movement Mood swings Light touch Deep breathing Coughing Bearing down Lying down Rolling in bed Other ______________________________________ Circle factors that help your pain: Nothing Resting Walking Standing Sitting Moving Physical therapy Massage Heat/Ice packs Medication Lying down Changing Positions Other__________________________________________________ Circle all characteristics of your pain: Constant Intermittent Burning Sharp Shooting Aching Throbbing Tingling Numbness Other _________________________ Circle prior treatments: Anti-inflammatory medications: (example Ibuprofen), Celebrex, Medrol dose pack Narcotics: Ultram (tramadol), Percocet, Oxycodone, Oxycontin, Vicoden, Hydrocodone, Morphine, Methadone, Dilaudid, Hydromorphone, Duragesic, Actiq Antidepressants: Elavil (Amitriptylline), Pamelor (nortriptylline), Trazodone, Desipramine, Cymbalta Antiseizure medication: Neurontin, Trileptal, Topamax, Gabitril, Lyrica Acupuncture, Magnets, Massage, Chiropractic manipulation, Herbs, Physical therapy Nerve Blocks , Epidural injections, Facet blocks , other ___________________________ ALLERGIES: __________________________________________________________ ALL CURRENT MEDICATIONS YOU ARE TAKING: ______________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ PAST AND PRESENT MEDICAL ISSUES/DISEASES: ______________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ PAST SURGERIES: _____________________________________________________ ________________________________________________________________________ ________________________________________________________________________
FAMILY HISTORY:
SOCIAL HISTORY: Circle all that applies to you. Single Married Divorced Separated Widowed Partnered Do you have children? Yes No How many? ___________________________________ Do you work? Yes No If so, describe please_________________________________ Do you Smoke? Yes No How much? _______________________________________ Do you drink? Yes No How much? _______________________________________ Do you use illicit drugs? Yes No How much? _______________________________ Have you ever been addicted to nicotine, alcohol, or illicit drugs? If so, Please explain ________________________________________________________________________ Are you involved in any unsettled legal issues involving your symptoms? Yes No If so, please explain: ________________________________________________________________________ ________________________________________________________________________ GENERAL HEATH QUESTIONS: Have you had any of the following in the past 2 weeks? (Circle all that applies to you) Fevers Chills Night sweat Unexplained weight loss Eye problems Ear problems Heart problems Lung problems Stomach problems Bladder /kidney problems Skin problems Neurological problems Psychological issues Thyroid problems Diabetes Bleeding problems Please explain any of the above: ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________ ________________________________________________________________________
Sonnenschein Lithium GmbH Industriestrasse 22 D-63654 Büdingen Technical Notice Safety data sheet 1. Identification 1.1 Product Name: 1.2 Company: 1.3 Emergency Telephone Number: 2. Composition/Information on Ingredients R 14/15 Reacts violently with water liberating extremely flammable gases Important Note: The material in this section may only rep
Guillain-Barré Syndrome Support Group After GBS — Pain This series of guides is produced by the Guillain-Barré Syndrome Support Group. We are aregistered charity that supports those affected by the Guillain-Barré syndrome (GBS) and relatedconditions in the United Kingdom and the Republic of Ireland. The related conditions includechronic inflammatory demyelinating polyradiculoneuropath

 6410 Rockledge Drive, Suite 110, Bethesda, MD, 20817 (O) 301.530.7303 (F) 301.530.7312
6410 Rockledge Drive, Suite 110, Bethesda, MD, 20817 (O) 301.530.7303 (F) 301.530.7312