La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Action plan 2013.pdf
FOOD ALLERGY ACTION PLAN
Student’s Name: _____________________________ D.O.B.___________________
ALLERGY TO: _______________________________________________________ Child’s
A special table for lunch/snacks is requested. ALLERGIC REACTION TREATMENT for ALLERGIC REACTION Any of these symptoms can represent an allergic reaction: 1. Injectable Epinephrine (check one) Mouth: itching and swelling of the lips, tongue or mouth Skin: hives, swelling of the face or extremities
❑ Twinject™ 0.3mg ❑ Twinject™ 0.15mg
Gut: nausea, abdominal pain, cramps, vomiting, diarrhea 2. Antihistamine Throat: tightening of throat, hoarsess, hacking cough Lungs: shortness of breath, repetitive cough, wheezing Heart: weak or thready pulse,low blood pressure, fainting, 3. Other ___________________________ 4. Call 911. State that an allergic reaction has Other: _____________________________________________
occured and epinephrine has been given. 5. Call Emergency Contacts (see below) SUSPICIOUS ALLERGIC REACTION TREATMENT for SUSPICIOUS REACTION 1. Antihistamine Symptoms: itchy rash or a few hives
❑ Benadryl ______________❑ Other _________________
2. Call Emergency Contacts (see below) Emergency Contacts: 1. Name/Relationship Phone Number(s) Phone Number(s)
a. _______________________________________ ________________________ _______________________b. _______________________________________ ________________________ _______________________c. _______________________________________ ________________________ _______________________
Even if parent/guardian cannot be reached, do not hesitate to medicate or call 911. 2. _________________________________________________________________________________________________
❑ The school may post this form in a visible location.
❑ If the patient presents to the emergency department, please monitor the patient for a biphasic reaction for at least ______ hours.
❑ Two doses of Epinephrine should be kept at school in case a repeat dose is needed.
❑ The student is capable and has been instructed in the proper method of self administering the medications named above and
may carry the medicines during school hours.
______________________________ ________________________________ ______________________________
Physician/Provider Signature Parent Signature Principal Signature
TRAINED STAFF MEMBERS 1. _______________________________________________________________________________ Room _______ 2. _______________________________________________________________________________ Room _______ 3. _______________________________________________________________________________ Room _______
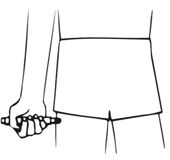
Twinject® 0.3 mg and Twinject® 0.15 mg Directions
Hold black tip near outer thigh (always apply to thigh).
Remove caps labeled “1” and “2.”
Place rounded tip against outer thigh, press down hard until needle penetrates. Hold for 10 seconds, then remove.
to 10. Remove the EpiPen® unit and massage the injection area for 10
syringe from barrel by holding blue collar at needle base.
Put needle into thigh through skin, push plunger down all the way, and remove.
Once EpiPen® or Twinject® is used, call the Rescue Squad. Take the used unit with you to the Emergency Room. Plan to stay for observation at the Emergency Room for at least 4 hours.
SIERRA COLLEGE ADMINISTRATIVE PROCEDURE No. AP 4255 Drug Policy - Nursing Program Drug Testing upon Admission to the Clinical Component Students are admitted to the nursing program pending a negative drug test. Admission will be withdrawn for a student testing positive. Procedure for Drug Testing Students Students admitted to the nursing program will be notified of the
Bioconjugate Chem. 2002, 13, 518−524 Methotrexate Conjugate with Branched Polypeptide Influences Leishmania donovani Infection in Vitro and in Experimental Animals† Gyo¨rgy Ko´cza´n,‡ Asoke C. Ghose,§ Ananda Mookerjee,§ and Ferenc Hudecz*,‡Research Group of Peptide Chemistry, Hungarian Academy of Sciences, Eo¨tvo¨s L. University,Budapest 112, POB 32, Hungary, H-1518 a

 TRAINED STAFF MEMBERS
TRAINED STAFF MEMBERS