La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Tgastro.com
Understanding Peptic Ulcers What are peptic ulcers?
An “ulcer” is an open sore. The word “peptic” means that the cause of the problem is due to acid. Most of the time when a gastroenterologist is referring to an “ulcer” the doctor means a peptic ulcer.
The two most common types of peptic ulcer are called “gastric ulcers” and “duodenal ulcers”. These names refer to the location where the ulcer is found. Gastric ulcers are located in the stomach (see Figure 1). Duodenal ulcers are found at the beginning of the small intestine known as the duodenum. A person may have both gastric and duodenal ulcers at the same time.
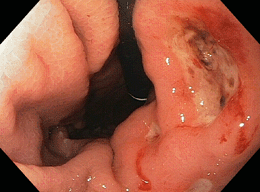
Figure 1. Photograph of a peptic ulcer taken during an upper endoscopy. This ulcer is a “gastric ulcer” because it is located in the stomach. What causes ulcers?
The two most important causes of ulcers are infection with Helicobacter pylori and a group of medications known has NSAIDs.
Helicobacter pylori (also called “H. pylori” or “HP”) is a bacterium that lives in the stomach of infected people. The understanding that H. pylori can cause ulcers was one of the most important medical discoveries of the late 20th century. In fact, Dr. Barry Marshall and Dr. J. Robin Warren were awarded the 2005 Nobel Prize in Medicine for this discovery.
People infected with H. pylori are at increased risk of developing peptic ulcers. When a person is diagnosed with an ulcer, testing for H. pylori is often done. There are a number of tests to diagnose H. pylori. Which test is used depends on the situation.
People with ulcers who are infected with H. pylori should have their infection treated. Treatment usually consists of either three or four drugs. The drug therapy may use acid suppression therapy with a proton pump inhibitor (PPI) along with antibiotic therapy and perhaps a bismuth containing agent such as Pepto-Bismol. H.
pylori can be very difficult to cure; so it is very important that people being treated for this infection take their entire course of antibiotics as prescribed.
NSAIDs (Non-Steroidal Anti-Inflammatory Drugs) are a group of medications typically used to treat pain. There are many drugs in this group. A few of these include: aspirin (Bayer®), ibuprofen (Motrin®, Advil®), naproxen (Aleve®, Naprosyn®), ketorolac (Toradol®) and oxaprozin (Daypro®). NSAIDs are also included in some combination medications, such as Alka-Seltzer®, Goody’s Powder® and BC Powder®.
Acetaminophen (Tylenol®) is NOT an NSAID and is therefore the preferred non-prescription treatment for pain in patients at risk for peptic ulcer disease.
Because NSAIDs are so common, and because many are available over the counter without a prescription, they are a very common cause of peptic ulcers. NSAIDs cause ulcers by interrupting the ability of the stomach and the duodenum to protect themselves from naturally occurring stomach acid. NSAIDs also can interfere with blood clotting. This has obvious importance when ulcers bleed.
People who take NSAIDs for a long time, at high doses or both, have a higher risk of developing ulcers. These people should discuss preventing ulcers with their physician. A PPI can prevent or significantly reduce the risk of an ulcer being caused by NSAIDs.
What does NOT cause ulcers?
There are many myths about peptic ulcers. Ulcers are not caused by emotional “stress” or by worrying. They are not caused by spicy foods or a rich diet. Certain foods might irritate an ulcer that is already there, however, the food is not the cause of the ulcer. People diagnosed with ulcers do not need to follow a specific diet. The days of ulcer patients surviving on a bland diet are a thing of the past.
What symptoms do ulcers cause?
Many people with ulcers have no symptoms at al . And, not all pain in the abdomen is an “ulcer”.
The most important symptoms that ulcers cause are bleeding and pain.
Bleeding from an ulcer can be slow and go unnoticed or can cause life-threatening hemorrhage. Ulcers that bleed slowly might not produce the symptoms until the person becomes anemic. Symptoms of anemia include fatigue, shortness of breath with exercise and pale skin color.
Bleeding that occurs more rapidly might show up as melena – jet black very sticky stool (often compared to “roof tar”) – or even a large amount of dark red or maroon blood in the stool. People with bleeding ulcers may also vomit. This vomit may be red blood or may look like “coffee grounds”. Other symptoms might include “passing out” or feeling lightheaded. Symptoms of rapid bleeding represent a medical emergency. If this occurs, immediate medical attention is needed. People with these symptoms should dial 911 or go to the nearest emergency room.
How are ulcers diagnosed?
Ulcers are usually diagnosed in one of two ways. The first of these is called an “upper GI series”. An upper GI series involves drinking a white chalky substance called barium, and then taking a number of x-rays to look at the lining of the stomach. Doctors can see the ulcers on the x-rays when they have barium in them.
Another way that ulcers are diagnosed is by an EGD. EGD stands for EsophagoGastroDuodenoscopy. An EGD (also cal ed “upper endoscopy”) is performed by inserting a special lighted camera on a flexible tube into the person’s mouth to look directly into the stomach and the beginning of the small bowel. Ulcers identified during an EGD may be photographed, biopsied and even treated, if bleeding is present.
How are ulcers treated?
The way that ulcers are treated depends on a number of features. Nearly all peptic ulcers will be treated with a proton pump inhibitor (PPI). PPIs are powerful acid blocking drugs that can be taken as a pill or given in an IV. There are five PPIs available in the United States. These are omeprazole (Prilosec®, Zegerid®), lansoprazole (Prevacid®), pantoprazole (Protonix®), rabeprazole (Aciphex®) and esomeprazole (Nexium®). There are very few medical differences between these drugs.
PPIs require a meal to activate them. Patients should eat a meal within 30 minutes to 1 hour after taking this medication for the acid suppression therapy to work most effectively. Waiting later than this time can decrease the positive effect of this medication. This might delay healing or even result in the failure of the ulcer to heal.
Sometimes duodenal ulcers (not gastric ulcers) will be treated with H2 blockers. H2 blockers are another type of acid reducing medication. Common H2 blockers are ranitidine (Zantac®), cimetidine (Tagamet®), famotidine (Pepcid®) and nizatidine (Axid®).
Ulcers are also treated by identifying what caused them. When possible, NSAIDs should be stopped. If the person is infected with H. pylori this infection should be treated.
When someone has an ulcer that has bled significantly treatment might be done at the time of EGD. There are a number of techniques that can be performed during an EGD to control bleeding from ulcer. The gastroenterologist might inject medications or use cautery to burn the ulcer. Not all ulcers need to be treated this way. The doctor doing the EGD will decide if treatment is indicated based on the way the ulcer looks. The doctor will usually treat an ulcer that is actually bleeding when it is seen. He will also often treat other ulcers if they have a certain appearance. These findings are sometimes called “stigmata of recent hemorrhage” or just “stigmata”. Stigmata will usually get treated during the EGD if they are classified as high-risk. Common high-risk findings include a “visible vessel” and an “adherent clot”.
Do ulcers ever go away or get healed?
Most ulcers can be healed. Often, people with ulcers will have to take PPIs for several weeks to heal an ulcer. It is also important to correct what caused the ulcer. When possible, NSAIDs should be stopped. Patients with ulcers caused by NSAIDs should talk to their doctor about other medications that can be used to treat pain.
If the person is infected with Helicobacter pylori, then completing the full dose of antibiotics is very important. Just as important, is making sure that the infection is gone. There are number of ways to do this. Generally, a blood test is not a good way to test if the infection is gone. The doctor who treated the infection can recommend the best way to do the “test of cure”.
People with gastric ulcers (only in the stomach) must have another EGD several weeks after treatment to make sure that the ulcer is gone. This is because a very small number of gastric ulcers might contain cancer. Duodenal ulcers (at the beginning of the smal intestine) usually don’t need to be looked at again.
Deuxièmes Journées Nationales de Cytométrie en Flux (JNCF 2009) Monastir 15, 16 et 17 janvier 2009 Deuxièmes Journées Nationales de Cytométrie en Flux Faculté de Pharmacie de Monastir: 15-17 janvier 2009 Jeudi 15 janvier 2009 (Atelier Pratique) 08h00 – 09h00 : INSCRIPTION 09h00 – 12h30 : COURS 09h00 - 10h30 : Cours 1 (Claude LAMBERT): Principes
Report for Brighton and Hove Health and Wellbeing Board (HWBB) and Clinical Commissioning Group (CCG) 9.8.13 By John Kapp, 22, Saxon Rd Hove BN3 4LE, 01273 417997, johnkapp@btinternet.com CURING THE NHS AND DEPRESSED PATIENTS BY MASS-COMMISSIONING THE MINDFULNESS COURSE The crisis in the NHS is caused by the following factors, which can be solved locally by councillors initiating culture change
 Understanding Peptic Ulcers
Understanding Peptic Ulcers