La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Role of ud testing
Urethral Pressures- A New Role in UD Testing Author: Timothy McKinney, M.D., Ph.D. For: Laborie Quarterly Newsletter, 2006
The goal of urodynamics testing is to provide objective confirmation
of the signs and symptoms of incontinence and voiding dysfunction. While diagnosis and optimal treatment of lower urinary tract dysfunction (LUTD) requires a careful history and objective evaluation, it has been demonstrated that urinary symptoms alone are not specific in predicting the type of dysfunction (15-40% of diagnoses will be wrong without urodynamics testing, and 25-30% of patients will have multiple diagnoses) (1,2,3). The dilemma facing physicians treating urinary dysfunction is that symptoms, patient questionnaires, physical examination findings, voiding diaries, and pad testing do not correlate well with the final diagnosis. Urodynamics testing must be interpreted in combination with other findings as part of an intelligent decision making process.
Naturally, there remains a level of uncertainty about the role of
urodynamics. Some feel that it is not cost effective and only helpful under certain circumstances. Others consider urodynamics essential in assessing urinary incontinence to confirm definitive and objective diagnosis (4,5,6,7) and have advocated its use in all patients prior to surgical intervention (8,9,10,11). Urodynamics can detect detrusor overactivity that may or may not be clinically relevant. It will also detect neurological pathophysiology such as detrusor sphincter dyssynergia and urethral instability, which is a subtle but powerful cause of frequency and urgency syndromes. With new advances in urodynamics technologies, it is hoped that the results will correlate more closely to true clinical findings and further help with clinical outcome prediction and proper choices of therapy. The definition of urethral instability is a variation off the Pura baseline pressure of plus or minus 15 cm H2O. I consistently use a dual pressure sensor, circumferential T-DOC "air-charged" catheter as a technique for diagnosing urethral instabilty. The finding of urethral instability and for that matter, most urethral pathophysiology, has been dificult to see with traditional, point sensor technologies of water, microtip and fiberoptic catheters. Tanago and Ulmsten had taught that you need to measure pressures within the urethra in a circumferential area for accurate pathophysiology, and they had used a fluid filled balloon in some of their
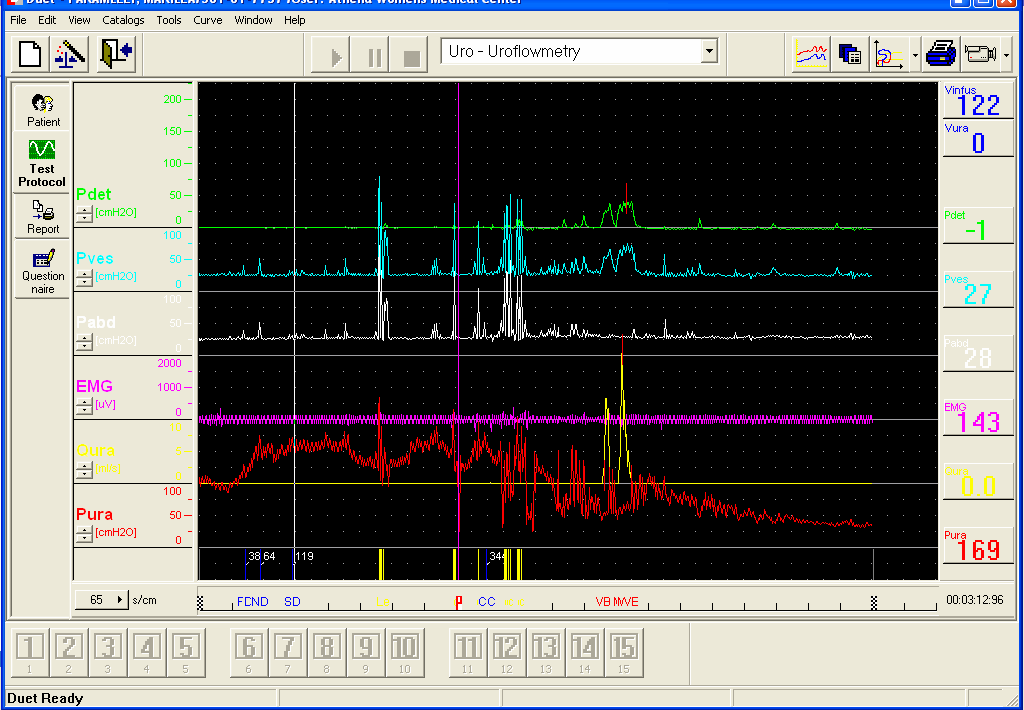
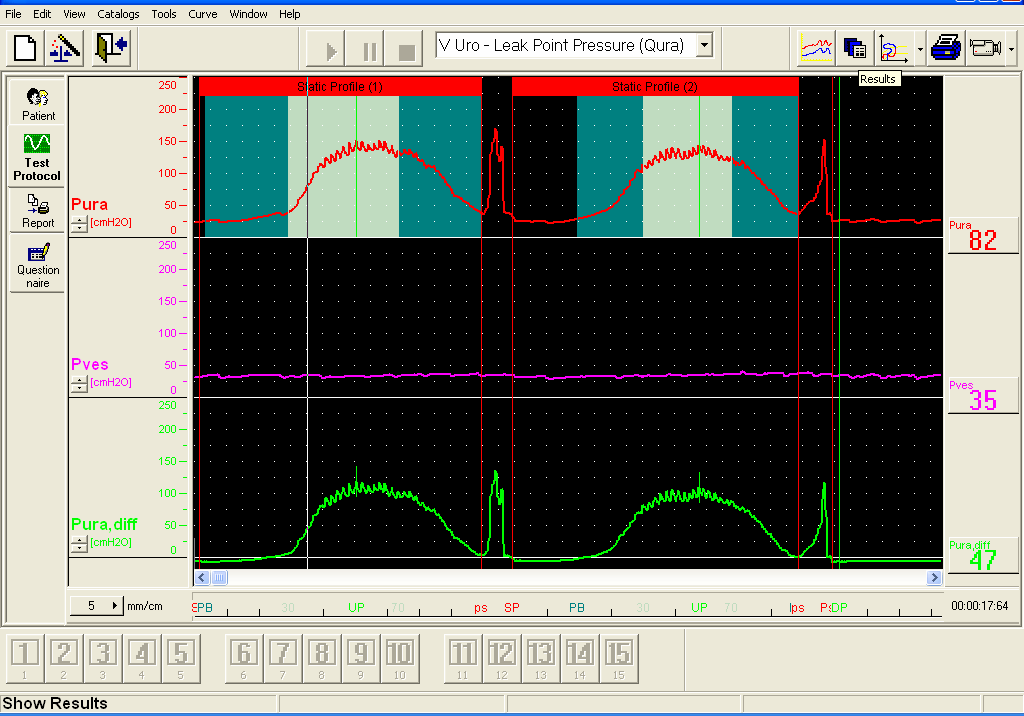
research. Using "air charged" vs. "fluid filled" balloon alleviates the difficulty caused by gravitational effects of air bubbles in the water as well as thermal changes of the water. For best results, I place one sensor into the bladder with the second sensor at the midurethra. Pressures are watched during the filling phase of the complex cystometrogram. To avoid false readings, I place the urethral sensor just to the bladder side of the maximum urethal pressure and use both tape and hand holding of the catheter to prevent the migration of the pressure sensor (fig. 1). If the pressure sensor is too close to either the UVJ or to the urethral meatus, the pathophysiological changes can be missed. This situation was demonstrated in the case report of a 19 yr old patient of mine, who presented with a frequency / urgency syndrome characterized by voiding 50x daily and Q20 minutes at night. She had a prior complex CMG without a urethral pressure recording, that showed normal pressures and EMG without detrusor instability. She had been treated over a 4 year period with anticholinergics as well as biofeedback and other conservative therapies with no success, and was on sedatives and had two suicide attempts. Upon repeating the urodynamics with a urethral pressure sensor, she demonstrated severe urethral instability (fig. 2). She had a negative workup for interstitial cystitis and failed Flomax therapy. I brought her from the psychiatric ward to the OR and placed a sacral nerve stimulator (the Medtronic "InterStim" brand SNS Therapy) with complete reversal of her symptoms. After the InterStim unit placement we repeated her urodynamics, which showed an absence of (correction of) the urethral instability. This is the first documented finding that I know of, showing an objective change demonstated on urodynamics that led to a reversal of a patient's physical symptoms. This phenomona was the impetus to do a retrospective chart review to see if we had similar findings with other patients who had been treated with InterStim SNS therapy. In the retrospective chart review, we saw an interesting coorelation on urodynamics between urethral instability and the success of SNS. Of patients treated with SNS, 26/30 implants (86.66%) were successful. Urethral instability had been urodynamicsally demonstrated in 23/26 of the successful cases (88.4%). Two of the remaining three cases did not have a good CMG with Pura sensor in the right location, therefore, correlation was not possible to interpret but could have existed. One of the failed Sacral Nerve Stimulation had no urethral instability on urodynamics. Furthermore, 11 patients had both a diagnosis of interstitial cystitis (IC) and urethral instability, with severe Quality of Life
symptoms of frequency and urgency. These compromised patients had failed conservative therapy for IC and had underwent Sacral Nerve Stimulation implantation with a 10/11 success rate. Interstitial cystitis appears to have a neurological component; at the very least, it may have a subdivision that originates from the overstimulation of the sacral nerves that stimulate the release of mast cells, contributing to the symptoms. Therefore, as part of our algorithm for treatment of IC, we favor SNS if there are urodynamics findings consistent with urethral instability. In our prospective study, patients who presented with urethral instability as the sole finding on urodynamics, were implanted with InterStim therapy. These patients demonstrated a 100% success rate (15/15). This IRB study is still ongoing. It would be of great benefit to run a large prospective study to validate the significance of this urodynamics finding, and to verify that the neurological downregulation of the sacral nerves can lead to a stabilization of urethral pressures. In our experience, patients with the finding of frequency / urgency who demonstrate urethral instability and no DI on urodynamics testing, do not respond well to common anticholonergic/ antimuscarinic therapies for the overactive bladder. These patients appear to be better served using medications geared towards effecting the urethra, which has mainly norepinephrine and serotonergic receptors. Therefore, medications to stabilize the urethra such as alpha agonists (ephedrin, zyrtec D) and antagonists (Flomax, Hytrin) may be more helpful, although we still try the anticholinergic category. A significant number of our patients have benefited from this unusual conservative protocol and have not needed to progress to Sacral Nerve Stimulation. With this in mind we created an algorithm for the workup and treatment of frequency / urgency as shown in figure 3. Conclusions
Urodynamics has a significant role in urology, urogynecology and
female pelvic medicine. It is argued that urodynamics testing is not cost effective, limits access to specialty care, and requires specialized and expensive equipment, special training, and interpretation skills. 12 Urodynamics testing, despite certain limitations, continues to be the gold standard to define the pathophysiology of lower urinary tract dysfunction. It
is proposed that urodynamics is not necessary when straightforward stress urinary incontinence is the clinical diagnosis. Unfortunately, misdiagnosis with the potential for improper treatment is possible. The effects of unnecessary or inappropriate surgery, prolonged ineffective medical treatment, recurrent or persistent incontinence (particularly if a less effective surgery has been done), and post-operative voiding dysfunction, can lead to prolonged patient suffering with potential medico-legal ramifications.
Symptoms, questionnaires, voiding diaries, physical examination, and
pad testing are not predictive of the final diagnosis and may lead to misdiagnosis. Urodynamics testing is an essential component of the workup of the incontinent and voiding dysfunction patient. Looking at the total picture and all findings, including urethral pressures during filling cystometry, can shed some light on the frequency urgency patient that doesn’t exhibit DI or other neurological findings. 1 Cundiff GW, Harris RL, Coates KW, Bump RC. Clinical predictors of urinary incontinence in women. Am J Obstet Gynecol. 1997 Aug; 177(2):262-7. 2 Drutz HP, Mandel F. Urodynamics analysis of urinary incontinence symptoms in women. Am J Obstet Gynecol 1979;122:789-92. 3 Cardoza LD. Genuine stress incontinence and detrusor instability – a review of 200 patients. Br J Obstet Gynecol 1980;87:184-90. 4 Cantor TJ, Bates CP. A comparative study of symptoms and objective urodynamics findings in 214 incontinent women. Br J Obstet Gynecol. 1980;87:889-892. 5 Wiskind A 6 Digesu GA, Salvatore, Cardozo L, Robinson D, Khulla V. Symptomatic diagnosis of the overactive bladder: is it helpful? Neurourol Urodyn.2000;19:381-2. 7 Homma Y. The clinical significance of the urodynamics investigation in incontinence. BJU Int. 2002;90:489-97. 8 Summitt RL, Stovall T, Bent AE, Ostergard DR. Urinary incontinence: correlation of history and brief office evaluation with multichannel urodynamics testing. Am J Obstet Gynecol 1992;166:1835-44. 9 Sand PK, Hill RC, Ostergard DR. Incontinence history as a predictor of detrusor stability. Obstet Gynecol. 1988;71(2):257-60. 10 Korda A, Drieger M, Hunter P, Parkin G. The value of clinical symptoms in the diagnosis of urinary incontinence in the female. Aust N Z Obstet Gynaecol 1987;27:149-51.
11 McGuire EJ, Lytton B, Pepe V, Kohorn EI. Stress urinary incontinence. Obstet Gynecol. 1976;47:255. 12 Weber AM, Walters MD. Cost-effectiveness of urodynamics testing before surgery for women with pelvic organ prolapse and stress urinary incontinence. Am J Obstet Gynecol. 2000;183:1338-47.
Algorithm of frequency and urgency work up
Anticholinergics Alpha adrenergic antagonist
MAY 2002 Volume 1, Issue 1 AS PRESENTED IN THE DEPARTMENT OF ANESTHESIOLOGY, FACULTY OF MEDICINE UNIVERSITY OF MONTREAL Antiplatelet agents and Committee for Continuing Medical Education perioperative bleeding Department of AnesthesiologyUniversity of MontrealPierre Drolet, MD Chairman and Editor Intravascular thrombosis begins with an endothelial lesion, either spo
Lokaal Centraal informeertWe zijn er nog steeds niet!Het economisch tij zit niet mee! De gevol-gebieden, die groter zijn dan de huidige wij-kindeling. Op deze manier kan de zorg aan-geboden worden in de nabijheid van klantenmaatregelen die de burger direct, maar ookgeschrapt. De tijd voor grote ambities isen kan er efficiënter gewerkt worden. Tochindirect, raken. Het rijk geeft meer
 11 McGuire EJ, Lytton B, Pepe V, Kohorn EI. Stress urinary incontinence. Obstet Gynecol. 1976;47:255. 12 Weber AM, Walters MD. Cost-effectiveness of urodynamics testing before surgery for women with pelvic organ prolapse and stress urinary incontinence. Am J Obstet Gynecol. 2000;183:1338-47.
11 McGuire EJ, Lytton B, Pepe V, Kohorn EI. Stress urinary incontinence. Obstet Gynecol. 1976;47:255. 12 Weber AM, Walters MD. Cost-effectiveness of urodynamics testing before surgery for women with pelvic organ prolapse and stress urinary incontinence. Am J Obstet Gynecol. 2000;183:1338-47.