La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
043098 early pregnancy termination with mifepristone
C o py r ig h t , 1 9 9 8 , by t h e Ma s s a c h u s e t t s Me d i c a l S o c i e t y
V O L U M E 3 3 8 N U M B E R 1 8 EARLY PREGNANCY TERMINATION WITH MIFEPRISTONE AND MISOPROSTOL IN THE UNITED STATES
IRVING M. SPITZ, M.D., D.SC., C. WAYNE BARDIN, M.D., LAURI BENTON, M.D., AND ANN ROBBINS, PH.D. ABSTRACT Background
causes abortion by competitively blocking
have been used successfully to terminate pregnancy
progesterone receptors.1-3 For maximal ef-
in Europe and China. We report the results of a large
fectiveness, a prostaglandin should be giv-
U.S. study of mifepristone and misoprostol in wom-
en 48 hours after mifepristone.1,3,4 The rates of
en with pregnancies of up to nine weeks’ duration.
termination of pregnancies 49 days old or less are
Methods
similar, ranging from 96 to 99 percent, whether
and then 400 mg of misoprostol two days later to
mifepristone is used with gemeprost or misoprostol,
2121 women seeking termination of their pregnan-
both prostaglandin E compounds.1,3,5-7 Gemeprost
cies at 17 centers. The women were observed for
is expensive, requires refrigeration, and is not widely
four hours after the administration of misoprostol
available, but misoprostol is inexpensive, stable at
and returned on day 15 for final assessment. Results
room temperature, and obtainable in many coun-
the final assessment. Among them, pregnancy was
terminated in 762 of the 827 women pregnant for
Many American women do not have access to
р49 days (92 percent), 563 of the 678 women preg-
abortion,8 and in developing countries up to 200,000
nant for 50 to 56 days (83 percent), and 395 of the
women die annually of complications after illegal
510 women pregnant for 57 to 63 days (77 percent)
abortions.9 The availability of medical abortion in
(PϽ0.001). Termination occurred within 4 hours after
the United States and elsewhere could lead to great-
the administration of misoprostol in 49 percent of
er access to safer abortion services. We conducted a
the women and within 24 hours in 75 percent. Fail-
multicenter trial of mifepristone and misoprostol to
ures, defined as cases requiring surgical intervention
determine whether this combination could be used
for medical reasons or because the patient request-
to terminate pregnancies of up to 63 days’ duration.
ed it, the abortion was incomplete, or the pregnancywas ongoing, increased with increasing duration of
pregnancy. The largest increase was in failures rep-resenting ongoing pregnancy, which increased from
Participating Centers
1 percent in the р49-days group to 9 percent in the
From September 1994 to September 1995, we enrolled 2121
57-to-63-days group (PϽ0.001). Abdominal pain, nau-
women, each with a documented pregnancy of 63 days’ duration
sea, vomiting, diarrhea, and vaginal bleeding also in-
or less, requesting termination of pregnancy. Women with liver,
creased with advancing gestational age. Two percent
respiratory, renal, adrenal, or cardiovascular disease, thromboem-
of the women in the р49-days group, as compared
bolism, hypertension, anemia, insulin-dependent diabetes melli-
with 4 percent in each of the other two groups, were
tus, coagulopathy, or known allergy to prostaglandins were ex-
hospitalized, underwent surgical intervention, and
cluded, as were women less than 18 years of age or those morethan 35 years of age who smoked more than 10 cigarettes per day
received intravenous fluids (Pϭ0.008).
and had another cardiovascular risk factor. Women were also ex-
Conclusions
cluded if they had in situ intrauterine devices, were breast-feed-
men is effective in terminating pregnancies, espe-cially in women with pregnancies of 49 days’ dura-tion or less. (N Engl J Med 1998;338:1241-7.)1998, Massachusetts Medical Society.
From the Center for Biomedical Research, Population Council, 1230
York Ave., New York, NY 10021, where reprint requests should be ad-dressed to Dr. Robbins.
The principal investigators and centers participating in the study are list-
Downloaded from www.nejm.org at WELCH MEDICAL LIBRARY-JHU on April 17, 2005 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
ing, were receiving anticoagulation or long-term glucocorticoid
with respect to age (mean, 27 years; range, 18 to
therapy, had adnexal masses, had ectopic pregnancies, or had
45), gravidity, parity, number of spontaneous or
signs or symptoms suggesting they might abort spontaneously.
previous elective abortions, and ethnic or racial dis-
All the women agreed to undergo surgical termination of preg-nancy if the medical method failed. Among the 2121 women,
tribution (white, 71 percent; black, 15 percent; His-
915 were enrolled at eight Planned Parenthood clinics, 538 at
panic, 9 percent; Asian, 5 percent). Seventy-three
four university-hospital clinics, and 668 at five free-standing abor-
percent of the women had had previous pregnancies,
tion clinics. The protocol was approved by the human investiga-
51 percent elective abortions, and 15 percent spon-
tional review board at each participating institution, and all thewomen gave informed consent. Study Design Efficacy
Pregnancy was measured from the first day of the last menstrual
Among the 2015 women who returned for the
period according to menstrual history, pelvic examination, and
third visit, the rates of pregnancy termination were
vaginal ultrasonography. On the basis of the investigator’s final
92 percent in the р49-days group, 83 percent in the
assessment of these three measures, the women were assigned tothe following arbitrarily defined gestational-age groups: the р49-
50-to-56-days group, and 77 percent in the 57-to-
days group (859 women); the 50-to-56-days group (722); and
63-days group (PϽ0.001) (Table 1). Of the 59 wom-
en who did not receive misoprostol, 56 had termi-
Three clinic visits were scheduled. At visit 1 (day 1), the wom-
nation of their pregnancies after mifepristone alone.
en were assessed clinically and took 600 mg of mifepristone oral-
In the remaining three women, it subsequently be-
ly. At visit 2 (day 3), they took 400 mg of misoprostol orally un-less a complete abortion had already occurred. After taking
came apparent that their pregnancies had not been
misoprostol, the women were monitored for four hours for ad-
terminated after mifepristone and they should have
verse events, such as nausea, vomiting, diarrhea, and abdominal
been given misoprostol; they later underwent surgi-
pain. These events were rated by the women and recorded as mild
cal termination. The rate of termination after mife-
(felt but easily tolerated), moderate (uncomfortable enough tointerfere with usual activity), or severe (incapacitating, preventing
pristone alone also decreased significantly with in-
usual activity). Vaginal bleeding was recorded on a diary card and
creasing gestational age, from 5 percent to 0.8 percent
rated by each woman on days 1 through 15 of the study as spot-
ting (less than normal menstrual bleeding), normal (similar to
The rates of incomplete abortion were 8 percent
normal menstrual bleeding), or heavy (more than normal men-
in the 50-to-56-days group and 7 percent in the 57-
strual flow). During this period, the women were also monitoredfor expulsion of the conceptus. At visit 3 (day 15), the treatment
to-63-days group, as compared with 5 percent in the
р49-days group (Table 1). The failures for all other
Efficacy was defined as the termination of pregnancy with com-
reasons were significantly higher in both the 50-to-
plete expulsion of the conceptus without the need for a surgical
56- and 57-to-63-days groups than in the р49-days
procedure. The need for a surgical procedure (either vacuum as-piration or dilation and curettage) constituted a failure, and such
group. The largest increase was in failures represent-
a procedure was performed at any time if the investigator believed
ing ongoing pregnancy, which rose from 1 percent
there was a threat to a woman’s health (medically indicated), at a
in the р49-days group to 9 percent in the 57-to-63-
woman’s request, or at the end of the study for an ongoing preg-
days group. Ninety percent of the surgical termina-
nancy or incomplete abortion. Follow-up was extended beyond
tions performed for medical reasons were for vaginal
visit 3 if there was uncertainty about the completeness of theabortion or if bleeding persisted.
bleeding. A patient’s request was the reason least of-
A total of 106 women were excluded from the efficacy analysis
because they did not return for visit 3. Evidence suggesting a suc-
Although the study design called for analysis ac-
cessful outcome was available for 92 of these women, and evi-
cording to the three discrete gestational-age groups,
dence of failure for 1. The remaining 13 women were lost to fol-low up; 5 had continuing pregnancies when last seen at visit 2.
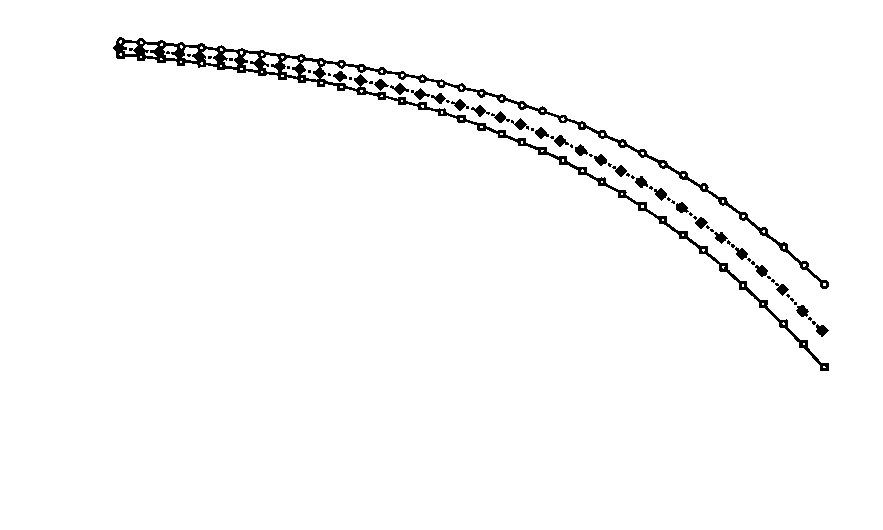
there was in fact a steady decline in the frequency of
The analyses of efficacy therefore included 2015 women.
termination of pregnancy with increasing durationof gestation (Fig. 1). Logistic-regression analysis in-
Statistical Analysis
dicated that the rates decreased with increasing ges-
Statistical analysis was performed with the use of Statistical
tational age, from more than 95 percent before day
Analysis System software (SAS Institute, Cary, N.C.). One-way
40 to less than 90 percent after day 47 and to less
analysis of variance and Kruskal–Wallis tests were used to compare
than 80 percent after day 59. The only other factor
mean values in the gestational-age groups, and Pearson’s chi-square tests were used to compare the distributions of categorical
that was related to outcome was the number of pre-
variables. Fisher’s exact test was used to compare rates in the ges-
vious elective abortions (Fig. 1); the termination
tational-age groups. Stepwise logistic-regression analysis was used
rates were higher for women with no previous abor-
to evaluate the relation between success or failure and various
tions than for those with previous abortions. The
base-line patient characteristics; the significance level required fora variable to stay in the model was 0.10. All statistical tests were
differences in rates were less than 2 percent up to day
35, 2 to 3 percent from days 36 to 42, 3 to 4 percentfrom days 43 to 48, 4 to 6 percent from days 49 to
55, and 6 to 10 percent from days 56 to 63. The
There were 859 women in the р49-days group,
outcomes were unrelated to other base-line charac-
722 in the 50-to-56-days group, and 540 in the 57-
teristics, including age, race, body weight, gravidity,
to-63-days group. The three groups were similar
Downloaded from www.nejm.org at WELCH MEDICAL LIBRARY-JHU on April 17, 2005 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
E A R LY P R E G N A N CY T E R M I N AT I O N W I T H M I F E P R I STO N E A N D M I S O P RO STO L I N T H E U N I T E D STAT E S TABLE 1. RESULTS OF MIFEPRISTONE AND MISOPROSTOL
IN WOMEN SEEKING TERMINATION OF PREGNANCY. PREGNANT PREGNANT PREGNANT
р49 DAYS 50 TO 56 DAYS 57 TO 63 DAYS (N؍827) (N؍678) (N؍510)
number (percent [95% confidence interval])
563 (83 [80–86])* 395 (77 [74–81])*†
*PϽ0.001 for the comparison with the р49-days group. †Pϭ0.02 for the comparison with the 50-to-56-days group. ‡0.001рPϽ0.03 for the comparison with the р49-days group. §PϽ0.001 for the comparison with the 50-to-56-days group.
Complete expulsion of the conceptus occurred
before the administration of misoprostol in 76 wom-en (4 percent). This group included the 56 women
who received only mifepristone and an additional 20women who received misoprostol because their ex-
pulsion status was considered uncertain at the be-ginning of visit 2. It was subsequently determined
that these 20 women had had complete expulsions
before they took misoprostol. During the four hours
of observation after the administration of misopros-tol, 49 percent of the women expelled the concep-
tus, and during the fifth hour an additional 11 per-
cent expelled the conceptus. By 24 hours after
misoprostol administration, 75 percent of the wom-en had expelled the conceptus (Fig. 2). Figure 1. Logistic-Regression Analysis of the Predicted Proba- bility of Successful Pregnancy Termination, According to the Vaginal Bleeding
Duration of Pregnancy for All the Women and for the WomenWho Had and Those Who Had Not Had Previous Elective Abor-
Vaginal bleeding is a natural consequence of the
abortion process, and it occurred in all the womenwhose pregnancies were terminated medically. Themedian duration of bleeding or spotting was 13 daysin the р49-days group and 15 days in the other two
ventions, and intravenous-fluid administration were
groups (PϽ0.001). The proportions of women who
reported for 2 percent of the women in the р49-days
reported heavy bleeding did not differ significantly
group and for 4 percent of those in each of the other
in the three groups, were highest on day 3, and then
groups (Pϭ0.008). Bleeding was managed by the
decreased steadily. By day 15, 77 percent of all re-
administration of uterotonic agents, such as oxyto-
ported bleeding was considered spotting (Fig. 3).
cin, methylergonovine, or vasopressin, in 41 women
Nine percent of the women reported some type of
(5 percent) in the р49-days group, 50 (7 percent) in
bleeding after 30 days, and 1 percent after 60 days.
the 50-to-56-days group, and 55 (10 percent) in the
Excessive bleeding necessitated blood transfusions
in four women and accounted for 25 of 27 hospital-izations (including emergency-room visits), 56 of 59
Other Adverse Events
surgical interventions, and 22 of 49 administrations
Almost all the women (99 percent) reported at
of intravenous fluid. Hospitalizations, surgical inter-
least one adverse event during the study period (Ta-
Downloaded from www.nejm.org at WELCH MEDICAL LIBRARY-JHU on April 17, 2005 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24
Figure 2. Times of Expulsion of the Conceptuses in 1720 Women with Successful Termination of Their Pregnancies.
The women received mifepristone at visit 1 and misoprostol two days later (visit 2). “Uncertain” indicates that expulsion occurredwithin the first 24 hours after misoprostol was given, but the exact time was not known. “Unknown” indicates that expulsion oc-curred more than 24 hours after misoprostol was given, but the exact time was not known.
ble 2). Nearly all had abdominal pain; its overall in-
In the four-hour observation period after the ad-
cidence did not differ among the three groups.
ministration of misoprostol, the number of adverse
However, 53 percent of the women in the 50-to-56-
events and the percentage classified as severe were
days group and 54 percent in the 57-to-63-days
similar to those reported during the entire study pe-
group had abdominal pain reported as severe, as
riod. During these four hours, nausea (PϽ0.001)
compared with 43 percent in the р49-days group
and vomiting (PϽ0.001) were significantly more fre-
(PϽ0.001). Sixty-eight percent of the women re-
quent in the 50-to-56- and 57-to-63-days groups
ceived at least one medication for abdominal pain
than in the р49-days group, and abdominal pain
(usually acetaminophen), and 29 percent also re-
(Pϭ0.009) and diarrhea (Pϭ0.006) were more se-
ceived opiates (usually acetaminophen with hydro-
codone or codeine). The women in the 50-to-56-
The frequency of adverse events declined signifi-
and 57-to-63-days groups received significantly more
cantly with increasing gravidity and parity (Table 2).
analgesia and opiates than the women in the р49-
Nulliparous women received significantly more anal-
days group (PϽ0.001). Abdominal pain resulted in
gesia (PϽ0.001), opiate analgesia (PϽ0.001), and
one hospitalization and was the reason for two med-
medications for nausea (PϽ0.001) and diarrhea (PϽ
ically indicated surgical interventions.
0.001) than parous women. Chronologic age was
As compared with the р49-days group, the 50-to-
not consistently related to the frequency of adverse
56- and 57-to-63-days groups had significantly more
nausea and vomiting, and diarrhea was more fre-
Other adverse events reported included headache
quent in the 57-to-63-days group. The overall per-
(32 percent); dizziness, encompassing light-headed-
centages of events reported as severe were 3 percent
ness and faintness (12 percent); back pain and fatigue
for diarrhea, 10 percent for vomiting, and 20 percent
(9 percent each); fever, vaginitis, and viral infections
for nausea. Medications for these adverse events were
(4 percent each); rigors and dyspepsia (3 percent
taken by 1 percent, 4 percent, and 19 percent of the
each); and asthenia, leg pain, anxiety, insomnia, ane-
women, respectively, with no differences among the
mia, syncope, leukorrhea, and sinusitis (2 percent
gestational-age groups. Severe vomiting resulted in
each). Endometritis occurred in 19 women; it was
one hospitalization and was the reason for one med-
considered study-related in 10, in 1 of whom it was
ically indicated surgical intervention.
Downloaded from www.nejm.org at WELCH MEDICAL LIBRARY-JHU on April 17, 2005 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
E A R LY P R E G N A N CY T E R M I N AT I O N W I T H M I F E P R I STO N E A N D M I S O P RO STO L I N T H E U N I T E D STAT E S Figure 3. Types of Vaginal Bleeding as Recorded by the Women from Day 1 (Administration of Mife- pristone) to Day 15.
The data are from 1506 women who did not undergo surgical termination of pregnancy and who re-corded the types of bleeding they had from study day 1 to day 15 on menstrual-diary cards. Bleedingwas characterized as spotting, as similar to normal menstrual bleeding (normal), or as heavier thannormal menstrual bleeding (heavy). TABLE 2. INCIDENCES OF ABDOMINAL PAIN, NAUSEA, VOMITING, AND DIARRHEA
ACCORDING TO GESTATIONAL GROUP, GRAVIDITY, AND PARITY. ABDOMINAL VARIABLE VOMITING DIARRHEA
*PϽ0.001 for the comparison with the р49-days group (by Fisher’s exact test). †Pϭ0.01 for the comparison with the р49-days group (by Fisher’s exact test). ‡0.001рPр0.03 for the comparison with the women who had had three or more pregnancies (by
§0.001рPр0.004 for the comparison with the women who had had no children (by Fisher’s exact
Downloaded from www.nejm.org at WELCH MEDICAL LIBRARY-JHU on April 17, 2005 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
T h e New E n g l a n d Jo u r n a l o f Me d i c i n e
DISCUSSION
did almost half the expulsions, and some women
In this large, multicenter U.S. trial, the success of
may prefer to be in the clinic during these events.
medical termination of pregnancy decreased gradu-
Moreover, in the women with pregnancies of longer
ally with advancing gestational age. We confirmed
duration, the majority of the hospitalizations or sur-
the international experience that mifepristone and
gical interventions occurred on day 3, whereas in the
misoprostol can terminate pregnancies of up to 49
women with pregnancies of shorter duration, these
days’ duration, although the success rate was lower
events were evenly distributed throughout the 15-
than previously described.7,10-12 As noted in other
day study period. Thus, the four-hour visit may be
countries,13 this lower success rate may be related to
most appropriate for women with pregnancies of
the lack of experience with medical abortion in the
longer duration. Nonetheless, on the basis of the re-
United States as well as to the design of our study.
sults of a small study, mifepristone combined with
We considered the need for surgical intervention on
home application of vaginal misoprostol is a safe al-
day 15 as representing failure, but abortion might
ternative in women with pregnancies of up to 56
have occurred later.13,14 Also, a surgical termination
performed at the woman’s request was classified as a
Careful medical follow-up is essential to ensure that
failure instead of being excluded from the efficacy
surgical termination is performed in cases of failed
analysis.10,12,13 Unexpectedly, success was also less fre-
medical abortion. In this study, 5 percent of the
quent among women who had previous elective
women did not return for final confirmation of the
abortions. Although the reason is unknown, this fac-
outcomes of their pregnancies, and five of these wom-
tor could also have contributed to the differences,
en had continuing pregnancies when last seen at visit
because 51 percent of the women in our study had
2. The ultimate outcome of these pregnancies is un-
had previous elective abortions, as compared with
known, despite our repeated attempts to contact the
25 to 27 percent in two British studies.12,13
women. In other studies, the loss to follow-up has
Efficacy decreased after 49 days’ gestation. A sim-
ranged from 3 to 11 percent.5-7,10,12,21 Although mife-
ilar trend has previously been reported with miso-
pristone is not teratogenic in rats, mice, or mon-
prostol but not with gemeprost.10-15 Thus, the lower
keys,22,23 skull deformities attributed to uterine con-
success rates later in gestation are probably related
tractions occurred in rabbits.24 Misoprostol, on the
to the prostaglandin component of the regimen.
other hand, has been reported to be teratogenic in
Such lower rates were not found when misoprostol
was given by the vaginal route,16,17 presumably be-
Recently, other methods of medical abortion have
cause of greater tissue bioavailability.18 Higher doses
been evaluated. Oral misoprostol alone is not effec-
of oral misoprostol increase uterine contractility19
tive.19,27 The efficacy of vaginal misoprostol in the
and are also associated with improved results.11,12,15
first trimester varies widely, from 47 to 94 per-
Efficacy is not, however, related to differences in
cent,28,29 but it is highly effective in the second tri-
the dose of mifepristone, and similarly good results
mester.30 Success rates with methotrexate and vagi-
have been reported with single doses as low as 200
nal misoprostol range from 83 to 98 percent.31-35 As
compared with mifepristone, this latter regimen has
The incidence of adverse events rose with the du-
the advantage of being an effective treatment for ec-
ration of pregnancy.7,10,13 These events included both
topic pregnancy.36 However, misoprostol has to be
subjective symptoms (abdominal pain, nausea, and
given three to seven days after methotrexate, de-
vomiting) and more objective markers (hospitaliza-
laying the abortion process.35 Unlike mifepristone,
tions and surgical interventions). The majority of
methotrexate is cytotoxic to proliferating trophoblast
hospitalizations and surgical interventions were for
tissue, and persisting pregnancies may represent a
vaginal bleeding. With advancing pregnancy, the du-
ration of bleeding increased, as did the administra-
In conclusion, the regimen of mifepristone and
tion of uterotonic drugs and intravenous fluids. De-
misoprostol is safe and effective for women seeking
spite the increases in the numbers of failures and
medical abortions of pregnancies of 49 days’ dura-
adverse events, the majority of the women in this
tion or less. With longer durations of pregnancy, the
study reported that they were satisfied with their
regimen is less effective and the incidence of adverse
medical abortions, regardless of whether the out-
come was successful (Winikoff B, et al.: unpublisheddata).
One drawback of this method of pregnancy termi-
We are indebted to Dr. Elof Johansson for his helpful advice and
nation is the inconvenience of the four-hour clinic
continuing support; to Dr. Brigid M. O’Connor, Dr. Charlotte El-
stay after the administration of misoprostol. In its fa-
lertson, Dr. Beverly Winikoff, and Ms. Batya Elul for their contri-butions to the data analysis; to Mr. Evan Read for preparation of
vor is the fact that many adverse events, including
the figures; and to Mr. Peter Conlon and Ms. Irina Shmerlin for
those rated as severe, occurred during this period, as
Downloaded from www.nejm.org at WELCH MEDICAL LIBRARY-JHU on April 17, 2005 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
E A R LY P R E G N A N CY T E R M I N AT I O N W I T H M I F E P R I STO N E A N D M I S O P RO STO L I N T H E U N I T E D STAT E S APPENDIX
Fertility Regulation. Termination of pregnancy with reduced doses of mife-pristone. BMJ 1993;307:532-7.
The participating principal investigators and their associated centers are
15. el-Refaey H, Templeton A. Early abortion induction by a combination
listed below (at the investigator’s request, Planned Parenthood of Greater
of mifepristone and oral misoprostol: a comparison between two dose reg-
imens of misoprostol and their effect on blood pressure. Br J Obstet Gy-
P. Blumenthal, Johns Hopkins Bayview Medical Center, Baltimore; L.
Borgatta, Planned Parenthood of Westchester and Rockland, White Plains,
16. el-Refaey H, Rajasekar D, Abdalla M, Calder L, Templeton A. Induc-
N.Y.; M.D. Creinin, University of Pittsburgh, Pittsburgh; C.L. Dean,
tion of abortion with mifepristone (RU 486) and oral or vaginal misopros-
Washington University School of Medicine, St. Louis.; S. Haskell, Planned
Parenthood of Greater Iowa, Des Moines; T.C. Malloy, Feminist Women’s
17. Schaff EA, Stadalius LS, Eisinger SH, Franks P. Vaginal misoprostol ad-
Health Center, Atlanta; D.R. Mishell, Jr., University of Southern California
ministered at home after mifepristone (RU486) for abortion. J Fam Pract
School of Medicine, Los Angeles; M. Nichols and E. Newhall, Oregon
Health Sciences University, Portland; Planned Parenthood Clinic of Great-
18. Zieman M, Fong SK, Benowitz NL, Banskter D, Darney PD. Absorp-
er Boston, Boston; A.N. Poindexter, Planned Parenthood of Houston and
tion kinetics of misoprostol with oral or vaginal administration. Obstet Gy-
Southeast Texas, Houston; S.T. Poppema, Aurora Medical Services, Seattle;
E. Rothenberg, Planned Parenthood of Central New Jersey, Shrewsbury;
19. Norman JE, Thong KJ, Baird DT. Uterine contractility and induction
K.L. Sheehan, Planned Parenthood of San Diego and Riverside Counties,
of abortion in early pregnancy by misoprostol and mifepristone. Lancet
San Diego, Calif.; L. Sogor, Preterm, Cleveland; J. Tyson, Planned Parent-
hood of Northern New England, Burlington, Vt.; P. Vargas, Planned Par-
20. Prasad RN, Choolani M. Termination of early human pregnancy with
enthood of the Rocky Mountains, Denver; and C. Westhoff, Columbia
either 50 mg or 200 mg single oral dose of mifepristone (RU486) in com-
University College of Physicians and Surgeons, New York.
bination with either 0.5 mg or 1.0 mg vaginal gemeprost. Aust N Z J Ob-stet Gynaecol 1996;36:20-3. REFERENCES 21. Broome M. Using mifepristone in a family planning clinic. Br J Fam Plann 1994;20:11-2. 1. Spitz IM, Bardin CW. Mifepristone (RU 486) — a modulator of 22. Baulieu E-E, Segal SJ, eds. The antiprogestin steroid RU 486 and hu-
progestin and glucocorticoid action. N Engl J Med 1993;329:404-12.
man fertility control. New York: Plenum Press, 1985:123-40. 2. Couzinet B, Le Strat N, Ulmann A, Baulieu EE, Schaison G. Termina- 23. Wolf JP, Chillik CF, Dubois C, Ulmann A, Baulieu EE, Hodgen GD.
tion of early pregnancy by the progesterone antagonist RU 486 (mifepris-
Tolerance of perinidatory primate embryos to RU 486 exposure in vitro
tone). N Engl J Med 1986;315:1565-70.
and in vivo. Contraception 1990;41:85-92. 3. Spitz IM, Bardin CW. Clinical pharmacology of RU 486 — an anti- 24. Jost A. Nouvelles donnése sur le besoin hormonal de la lapine ges-
progestin and antiglucocorticoid. Contraception 1993;48:403-44.
tante: grossesses partielles et anomalies foetales après traitement par un an-
4. Bygdeman M, Swahn ML. Progesterone receptor blockage — effect on
tagoniste hormonal à dose sub-abortive. C R Acad Sci III 1986;303:281-4.
uterine contractility and early pregnancy. Contraception 1985;32:45-
25. Fonseca W, Alencar AJC, Mota FSB, Coelho HLL. Misoprostol and
congenital malformations. Lancet 1991;338:56. 5. Ulmann A, Silvestre L, Chemama L, et al. Medical termination of early 26. Gonzalez CH, Vargas FR, Perez AB, et al. Limb deficiency with or
pregnancy with mifepristone (RU 486) followed by a prostaglandin ana-
without Mobius sequence in seven Brazilian children associated with miso-
logue: study in 16,369 women. Acta Obstet Gynecol Scand 1992;71:278-
prostol use in the first trimester of pregnancy. Am J Med Genet 1993;47:
6. Silvestre L, Dubois C, Renault M, Rezvani Y, Baulieu E-E, Ulmann A. 27. Coêlho HL, Teixeira AC, de Fátima Cruz M, et al. Misoprostol: the
Voluntary interruption of pregnancy with mifepristone (RU 486) and a
experience of women in Fortaleza, Brazil. Contraception 1994;49:101-10.
prostaglandin analogue: a large-scale French experience. N Engl J Med
28. Creinin MD, Vittinghoff E. Methotrexate and misoprostol vs miso-
prostol alone for early abortion: a randomized controlled trial. JAMA
7. Peyron R, Aubény E, Targosz V, et al. Early termination of pregnancy
with mifepristone (RU 486) and the orally active prostaglandin misopros-
29. Carbonell JL, Varela L, Valezco A, Fernandez C. The use of misopros-
tol for termination of early pregnancy. Contraception 1997;55:165-8. 8. Henshaw SK, Van Vort J. Abortion services in the United States, 1991 30. Jain JK, Mishell DR Jr. A comparison of intravaginal misoprostol with
and 1992. Fam Plann Perspect 1994;26:100-6, 112.
prostaglandin E for termination of second-trimester pregnancy. N Engl J
9. Idem. Induced abortion: a world review, 1990. Fam Plann Perspect 31. Hausknecht RU. Methotrexate and misoprostol to terminate early 10. Aubeny E, Peyron R, Turpin CL, et al. Termination of early pregnancy
pregnancy. N Engl J Med 1995;333:537-40.
(up to 63 days of amenorrhea) with mifepristone and increasing doses of
32. Schaff EA, Eisinger SH, Franks P, Kim SS. Methotrexate and misopros-
misoprostol. Int J Fertil Menopausal Stud 1995;40:Suppl 2:85-91.
tol for early abortion. Fam Med 1996;28:198-203. 11. McKinley C, Thong KJ, Baird DT. The effect of dose of mifepristone 33. Wiebe ER. Abortion induced with methotrexate and misoprostol. Can
and gestation on the efficacy of medical abortion with mifepristone and
misoprostol. Hum Reprod 1993;8:1502-5. 34. Creinin MD, Vittinghoff E, Galbraith S, Klaisle C. A randomized trial 12. Baird DT, Sukcharoen N, Thong KJ. Randomized trial of misoprostol
comparing misoprostol three and seven days after methotrexate for early
and cervagem in combination with a reduced dose of mifepristone for in-
abortion. Am J Obstet Gynecol 1995;173:1578-84.
duction of abortion. Hum Reprod 1995;10:1521-7. 35. Creinin MD, Vittinghoff E, Keder L, Darney PD, Tiller G. Methotrex- 13. The efficacy and tolerance of mifepristone and prostaglandin in termi-
ate and misoprostol for early abortion: a multicenter trial. I. Safety and ef-
nation of pregnancy of less than 63 days gestation: UK Multicenter Study
ficacy. Contraception 1996;53:321-7.
— final results. Contraception 1997;55:1-5. 36. Grimes DA. Medical abortion in early pregnancy: a review of the evi- 14. World Health Organization Task Force on Post-ovulatory Methods of
dence. Obstet Gynecol 1997;89:790-6.
Downloaded from www.nejm.org at WELCH MEDICAL LIBRARY-JHU on April 17, 2005 .
Copyright 1998 Massachusetts Medical Society. All rights reserved.
CURRICULUM VITAE Amanda M. Loya, Pharm.D. BUSINESS ADDRESS/CONTACT INFORMATION: UTEP/UT Austin Cooperative Pharmacy Program 1101 N. Campbell St., El Paso, TX 79902 Office number: 915-747-8534 Fax: 915-747-8521 Email: amloya1@utep.edu LICENSES: Pharmacy Licensure: Texas State Board of Pharmacy, License # 41726 ACADEMIC PREPARATION: Scott & White/University of Texas at
SOYBEANS PLANNING BUDGETS Mississippi State University Department of Agricultural Economics Budget Report 2012-03 December 2012 Foreword This report is designed to provide necessary planning data to farmers, research and extension staffs, lending agencies, and others in agriculture. Readers are cautioned that returns presented are labeled " Returns Above Specified
 E A R LY P R E G N A N CY T E R M I N AT I O N W I T H M I F E P R I STO N E A N D M I S O P RO STO L I N T H E U N I T E D STAT E S
E A R LY P R E G N A N CY T E R M I N AT I O N W I T H M I F E P R I STO N E A N D M I S O P RO STO L I N T H E U N I T E D STAT E S