La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Sportsnutritionworkshop.com
Am J Physiol Endocrinol Metab 282: E551–E556, 2002.
First published October 30, 2001; 10.1152/ajpendo.00352.2001.
Effect of ibuprofen and acetaminophen on postexercisemuscle protein synthesis
T. A. TRAPPE,1 F. WHITE,1 C. P. LAMBERT,1 D. CESAR,2M. HELLERSTEIN,2 AND W. J. EVANS11Nutrition, Metabolism, and Exercise Laboratory, Donald W. Reynolds Center on Aging,Departments of Geriatrics and Physiology and Biophysics, University of Arkansas for MedicalSciences, and the Central Arkansas Veterans HealthCare System, Little Rock, Arkansas 72205;and 2Department of Nutritional Sciences, University of California, Berkeley, California 94720-3104
Received 3 August 2001; accepted in final form 29 October 2001
Trappe, T. A., F. White, C. P. Lambert, D. Cesar, M.
that ϳ5.5 million people in the United States consume
Hellerstein, and W. J. Evans. Effect of ibuprofen and
an analgesic, antipyretic, or nonsteroidal anti-inflam-
acetaminophen on postexercise muscle protein synthesis. AmJ Physiol Endocrinol Metab 282: E551–E556, 2002. First
Ibuprofen and acetaminophen are purported to re-
published October 30, 2001; 10.1152/ajpendo.00352.2001.—
lieve muscle soreness and pain through separate mech-
We examined the effect of two commonly consumed over-the-
anisms. Ibuprofen is known to block cyclooxgenase (EC
counter analgesics, ibuprofen and acetaminophen, on muscleprotein synthesis and soreness after high-intensity eccentric
1.14.99.1), which then reduces metabolites produced by
resistance exercise. Twenty-four males (25 Ϯ 3 yr, 180 Ϯ 6
this enzyme, such as prostaglandins, that are at least
cm, 81 Ϯ 6 kg, and 17 Ϯ 8% body fat) were assigned to one of
partially responsible for inflammation and algesia (14,
three groups that received either the maximal over-the-
35, 36). However, prostaglandins have also been shown
counter dose of ibuprofen (IBU; 1,200 mg/day), acetamino-
to regulate protein metabolism, and NSAIDs similar to
phen (ACET; 4,000 mg/day), or a placebo (PLA) after 10–14
ibuprofen have been shown to blunt protein metabo-
sets of 10 eccentric repetitions at 120% of concentric one-
lism in animal skeletal muscle (24, 30). Therefore,
repetition maximum with the knee extensors. Postexercise
skeletal muscle protein metabolism may be influenced
(24 h) skeletal muscle fractional synthesis rate (FSR) was
in individuals who consume ibuprofen after unaccus-
increased 76 Ϯ 19% (P Ͻ 0.05) in PLA (0.058 Ϯ 0.012%/h) and
tomed exercise. The mechanism of analgesic action of
was unchanged (P Ͼ 0.05) in IBU (35 Ϯ 21%; 0.021 Ϯ
acetaminophen, also known as paracetamol, is less
0.014%/h) and ACET (22 Ϯ 23%; 0.010 Ϯ 0.019%/h). Neitherdrug had any influence on whole body protein breakdown, as
clear; however, it is believed to have its analgesic
measured by rate of phenylalanine appearance, on serum
action within the central nervous system (8, 11, 15, 32,
creatine kinase, or on rating of perceived muscle soreness
36). Thus acetaminophen would not be expected to
compared with PLA. These results suggest that over-the-
interfere with muscle protein metabolism after exer-
counter doses of both ibuprofen and acetaminophen suppress
the protein synthesis response in skeletal muscle after eccen-
An important question is whether or not these drugs,
tric resistance exercise. Thus these two analgesics may work
when consumed at nonprescription levels, have any
through a common mechanism to influence protein metabo-
influence on metabolism and pain in humans after
unaccustomed exercise. Therefore, we studied the in-
paracetamol; analgesics; nonsteroidal anti-inflammatory
fluence of ibuprofen and acetaminophen, at their max-
imal over-the-counter daily dose, on skeletal muscleprotein fractional synthesis rate (FSR) and musclesoreness after high-intensity eccentric resistance exer-
ANALGESIC DRUGS ARE COMMONLY CONSUMED to reduce or
cise. This type of exercise has been shown to cause
prevent the pain and soreness encountered after com-
muscle soreness and damage and to stimulate a pro-
pletion of unaccustomed exercise. This is especially
tein metabolism response (13, 26). We hypothesized
true when the exercise contains eccentric (muscle
that a group that consumed no drug (placebo) or acet-
lengthening) contractions, which have been demon-
aminophen would elicit a large increase in FSR,
strated to result in relatively large amounts of muscle
whereas the ibuprofen group would respond with a
damage and soreness (13). Ibuprofen and acetamino-
blunted protein turnover response. We also hypothe-
phen are two popular over-the-counter analgesics con-
sized that both drugs would have an equal effect on
sumed for muscle soreness. In fact, it has been reported
reducing muscle soreness compared with placebo.
Address for reprint requests and other correspondence: T. Trappe,
The costs of publication of this article were defrayed in part by the
Nutrition, Metabolism, and Exercise Laboratory, DWR Center on
payment of page charges. The article must therefore be hereby
Aging, Univ. of Arkansas for Medical Sciences, 4301 W. Markham,
marked ‘‘advertisement’’ in accordance with 18 U.S.C. Section 1734
Slot 806, Little Rock, AR 72205 (E-mail: trappetodda@uams.edu).
each morning and, if necessary to maintain body weight, thecarbohydrate and fat content of the diet was altered.
In the morning on days 5 and 8, each subject underwent a
stable isotope infusion protocol (see Isotope infusion protocol)for the measurement of skeletal muscle protein FSR before
and after (24 h) a bout of high-intensity eccentric exercise
(day 7, see Eccentric exercise protocol). The evening beforeeach infusion protocol, the subjects spent the night in the
Values are means Ϯ SD. * Nondominant leg. ACET, acetamino-
NMEL and were instructed to eat their evening meal so as to
provide a fast of 10 h before the beginning of the FSRmeasurements.
Before and each morning after the exercise bout, each
subject came to the laboratory in the fasted state for a resting
Subjects. Twenty-four males were recruited and randomly
blood draw for creatine kinase (CK) determination and a
divided into three groups of eight: placebo (PLA), ibuprofen
rating of perceived soreness (see Measurement of perceived
(IBU), or acetaminophen (ACET) (Table 1). All subjects were
muscle soreness). The blood draw and soreness rating were
accepted into the study after giving informed consent and
completed in the supine position after ϳ10 min of supine
after a screening for any metabolic abnormalities via a blood
draw, urinalysis, and medical history questionnaire. Subjects
Isotope infusion protocol. On the morning of the infusions
were sedentary or recreationally active and were not com-
(Fig. 1), each subject had an 18-gauge catheter placed in an
pleting any formal exercise during the study or any resis-
antecubital vein for the infusion of a stable, isotopically
tance exercise for Ն6 mo before the investigation. None of the
subjects was chronically consuming ibuprofen, acetamino-
Woburn, MA) for the measurement of skeletal muscle protein
phen, or any analgesic or anti-inflammatory drug before the
FSR. A 20-gauge catheter was placed in retrograde fashion in
study. This investigation was approved by the Institutional
a dorsal vein of the hand, which was heated to provide an
Review Board of the University of Arkansas for Medical
arterialized blood sample (1). [2H5]phenylalanine was dis-
solved in sterile 0.9% saline, filtered through a 0.2-m filter
Overall experimental protocol. After enrollment in the
before infusion, and infused with a calibrated infusion pump
study, each subject completed a 16-day protocol (Fig. 1). To
(PHD 2000, Harvard Apparatus, Natick, MA) at a rate of 0.05
standardize protein intake, all of the subjects’ meals were
mol⅐kgϪ1⅐minϪ1 after a priming dose of 2.0 mol/kg as
prepared and provided by the metabolic kitchen of the Nu-
previously described (26). This protocol has been shown to
trition, Metabolism, and Exercise Laboratory (NMEL) during
result in steady-state [2H5]phenylalanine enrichments in the
the 16 days. Total caloric content of the meals was deter-
blood and muscle intracellular free amino acid pool within
mined by estimating the daily energy expenditure from the
120 min (6, 26, 37). Before and during each infusion, blood
Harris-Benedict equation (17) multiplied by an activity factor
samples were drawn (t ϭ 0, 120, 180, 210, 240, 260, 280, and
of 1.5. Each diet was composed of 1.2 g protein ⅐ kg body
300 min) for the measurement of plasma enrichment of
wtϪ1 ⅐ dayϪ1, with the remaining calories coming from carbo-
[2H5]phenylalanine. Muscle biopsies were taken from the
hydrate (ϳ55%) and fat (ϳ25%). Body weight was measured
vastus lateralis muscle of the dominant leg before and from
Fig. 1. A: overall experimental proto-col. Nos. represent days of the protocol. NMEL, Nutrition, Metabolism, andExercise Laboratory; FSR, fractionalsynthesis rate. Nos. represent time indays. B: isotope infusion schematic. Nos. represent time in minutes. AJP-Endocrinol Metab • VOL 282 • MARCH 2002 • www.ajpendo.org
the nondominant leg after the eccentric exercise protocol (t ϭ
and selected ion monitoring of mass-to-charge ratios (m/z)
120 and 300 min). Each muscle biopsy was taken through a
264, 267, 269, and 272 for the mϩ0, mϩ3, mϩ5, and mϩ8
new incision proximal to the previous biopsy. Tissue was
ions, respectively. Protein-bound enrichment was deter-
obtained after local anesthetic (lidocaine HCl 1%) with the
mined by monitoring m/z 267 and 269, which are the mϩ3
use of a 6-mm Bergstrom needle with suction (5). The muscle
and mϩ5 enrichments, respectively, where mϩ0 is the lowest
was cleansed of excess blood, connective tissue, and fat and
mass isotopomer in the ion envelope. Enrichment of the
immediately frozen in liquid nitrogen. The tissue was stored
protein-bound samples was determined using a linear stan-
in liquid nitrogen (Ϫ190°C) until analysis.
dard curve from mixtures of known mϩ5-to-mϩ3 ratios. Eccentric exercise protocol. On day 7, each subject com-
Precursor enrichment for calculation of FSR was determined
pleted a bout of unilateral high-intensity eccentric exercise
from intracellular [2H5]phenylalanine by monitoring the
with each leg. The maximal load that each subject could lift
mϩ5-to-mϩ0 ratio (mass 269 and 264 amu) enrichment of
concentrically with his knee extensors (i.e., one repetition
the NABE-phenylalanine. Plasma [2H5]phenylalanine en-
maximum, 1RM) was first determined and the eccentric
richments were measured from the mϩ5-to-mϩ0 ratio.
workload set to 120% of 1RM. The eccentric exercise con-
Calculations. FSR was calculated as the rate of [2H5]phenyl-
sisted of 10–14 sets of 10 repetitions with a 60-s rest between
alanine tracer incorporation into muscle protein, using the
sets of knee extensor exercise on a muscle dynamometer in
muscle intracellular free phenylalanine enrichment as the
the isotonic mode (Cybex Norm, Lumenex, Ronkonkoma,
NY). The range of 10–14 sets was achieved as a result of the
FSR ͑%/h͒ ϭ ͕͑Et Ϫ Et ͒/͓E ⅐ ͑t Ϫ t ͔͖͒ ⅐ 100
variation in fatigue of the muscles of each subject. When the
weight was lowered in less than 0.5 s, the subject completed
where Et0 is the enrichment in the protein-bound phenylal-
that set, was deemed fatigued, and the protocol was stopped.
anine tracer from the t ϭ 120-min biopsy, Et1 is the enrich-
Drug dose and administration. Drugs were administered
ment in the protein-bound phenylalanine tracer from t ϭ
in a double-blind placebo-controlled fashion. Each drug was
300-min biopsy, (t1 Ϫ t0) is the phenylalanine tracer incorpo-
administered in three doses each day (8 AM, 2 PM, and 8 PM)
ration time, and Ep is the mean intracellular free [2H5]phe-
corresponding to the maximal over-the-counter daily dose
nylalanine enrichment from both biopsies (t ϭ 120 and 300
(ibuprofen: 400 mg per dose, total of 1,200 mg; acetamino-
phen: 1,500, 1,500, and 1,000 mg, total of 4,000 mg). The
Whole body phenylalanine appearance, taken as a mea-
placebo group was given the same number of pills, which
sure of whole body protein breakdown, was calculated using
were indistinguishable from the drug doses. The first dose
was given at the start of the eccentric exercise protocol (ϳ8AM on day 7). On the day of the postexercise infusion proto-
col, the 8 AM dose was given at the start of the [2H5]phenyl-
alanine infusion. The times of dosing were chosen to divide
a is the rate of appearance (mol ⅐ kgϪ1 ⅐ minϪ1), F is
the infusion rate (mol ⅐ kgϪ1 ⅐ minϪ1), and E
the maximal over-the-counter dose evenly over the day and
as a result of the pharmacokinetic studies that had previ-
CK measurement. Serum CK activity was measured using
ously been completed on these drugs (2, 11, 19). When single
a commercial assay kit (Sigma Chemical, St. Louis, MO).
doses at or near those used in the current study are con-
Statistics. Subject characteristics (height, weight, age,
sumed, ibuprofen and acetaminophen have similar pharma-
%body fat, and eccentric load) among the groups were com-
cokinetic parameters. Both drugs appear in the plasma
pared using a one-way analysis of variance (ANOVA). FSR,
within 10 min; peak levels in plasma occur within 0.5–2.0 h;
phenylalanine Ra, CK, and muscle soreness before and after
and the half-life of both drugs is ϳ2 h (2, 11, 19). The subjects
exercise among the groups were compared using a two-way
were asked not to consume any other prescription or nonpre-
ANOVA with repeated measures over time. A two-way
ANOVA with repeated measures over time was also used to
Measurement of perceived muscle soreness. A subjective
compare blood and muscle intracellular free [2H5]phenylala-
measure of muscle soreness was obtained from each subject
nine enrichments over the blood draw and muscle biopsy
before the eccentric exercise protocol and each morning
time points, respectively, for both trials. Because of sample
throughout the protocol. Each subject was presented a scale
loss during mass spectrometry processing, FSR data include
from 1 to 9, with 1 being the absence of soreness and 9 being
n ϭ 7 (IBU), 6 (PLA), and 4 (ACET); all other data are
unbearable soreness, and was asked to rate the level of
represented by n ϭ 8 per group. When a significant difference
soreness after the application of 40 N of force using a force
was obtained, a Tukey’s post hoc analysis was used to find
transducer with a 2-cm-diameter tip (22, 23). Rating of per-
the location of the differences. Significance was accepted at a
ceived soreness was measured two times in random order
over nine sites over the four heads of the quadriceps femoris. Each site was maintained over the study period by re-mark-
ing with a permanent marker. The average of the two mea-surements and all nine sites was taken to represent the
There were no differences in any of the subject char-
average level of perceived soreness. The highest average
acteristics among the three groups (Table 1). Body
value of the nine sites was taken to represent the maximal
weight was maintained (P Ͼ 0.05) in all three groups
over the study (PLA: 86.5 Ϯ 22.7 vs. 85.6 Ϯ 23.0; IBU:
Measurement of isotope enrichment. Blood samples were
78.2 Ϯ 10.5 vs. 78.5 Ϯ 10.2; ACET: 77.6 Ϯ 14.9 vs.
analyzed for [2H5]phenylalanine enrichment, and muscle
samples were analyzed for free intracellular and protein-bound [2H
Blood and muscle intracellular free [2H5]phenylala-
5]phenylalanine enrichment by mass spectrometry
as previously described (6, 26), by use of the N-acetyl-n-butyl
nine enrichments did not change significantly over the
ester (NABE) derivative of phenylalanine. Derivatives were
time course (120–300 min) of both infusions (data not
analyzed by gas chromatography-mass spectrometry (Hew-
shown), which has been shown previously (6, 26, 37).
lett-Packard 5973, series II) using electron impact ionization
Postexercise (24 h) skeletal muscle FSR was increased
AJP-Endocrinol Metab • VOL 282 • MARCH 2002 • www.ajpendo.org
primary findings of this study were that ibuprofenblunted the protein synthesis response that is nor-mally seen after the type of exercise used in this study;surprisingly, acetaminophen also had a similar effecton protein metabolism.
From our data, it appears that the mechanism of
blunting protein metabolism in skeletal muscle by cy-clooxygenase inhibition outlined by Rodemann andGoldberg (30) nearly 20 yr ago in rats may also beintact in humans. These authors showed an inhibitionof protein synthesis in isolated rat skeletal muscle withthree different cyclooxygenase inhibitors (aspirin, in-domethacin, and meclofenamate). In the current study,we hypothesized that ibuprofen would also block cyclo-oxygenase and have a similar effect on muscle protein
Fig. 2. FSR (%/h) of mixed skeletal muscle protein before and afterthe eccentric exercise bout. ACET, acetaminophen group (n ϭ 4);
metabolism. However, it is difficult to determine how
IBU, ibuprofen group (n ϭ 7); PLA, placebo group (n ϭ 6). *P Ͻ 0.05
the amount of inhibitors (drugs) used in the previous
studies that showed this effect in isolated muscles (24,25, 30, 34) compare with the levels in human muscle
76 Ϯ 19% (P Ͻ 0.05) in PLA (0.058 Ϯ 0.012%/h), and
after consumption of maximal over-the-counter doses
was unchanged (P Ͼ 0.05) in IBU (35 Ϯ 21%; 0.021 Ϯ
of ibuprofen. Nonetheless, from our data, it is clear
0.014%/h) and ACET (22 Ϯ 23%; 0.010 Ϯ 0.019%/h)
that the 1.2 g/day maximal over-the-counter dose of
(Fig. 2). Whole body phenylalanine turnover (Ra phenyl-
ibuprofen is potent enough to blunt the protein synthe-
alanine) was unchanged (P Ͼ 0.05) in response to
sis response to resistance exercise.
exercise (PLA: 0.67 Ϯ 0.05 vs. 0.63 Ϯ 0.05 mol ⅐ kgϪ1 ⅐
What is less clear is why acetaminophen also inhib-
minϪ1) or either drug (IBU: 0.67 Ϯ 0.04 vs. 0.63 Ϯ 0.03;
ited the increase in FSR after the resistance exercise
ACET: 0.66 Ϯ 0.05 vs. 0.62 Ϯ 0.03 mol ⅐ kgϪ1 ⅐ minϪ1).
bout. The most logical hypothesis is that acetamino-
The CK response to the exercise was large and
phen also inhibits cyclooxygenase in skeletal muscle;
highly variable among the three groups. CK was sig-
however, to our knowledge, no other studies have ex-
nificantly elevated in all three groups after the exer-
amined the influence of acetaminophen on skeletal
cise, but the overall response was not different among
muscle metabolism. In addition, all of the previous
the groups (Table 2). Because some of the nine sites
data and the resultant nonperipheral effect of acet-
did not elicit a soreness response, the average level
aminophen hypothesis are derived from studies of the
of perceived muscle soreness underrepresented the
central nervous system and other nonskeletal muscle
amount of soreness that the subjects experienced.
However, average and maximal ratings of perceived
The small sample size of the FSR values for the
muscle soreness were elevated in a similar fashion
ACET group may appear to limit the interpretation of
after the exercise, and there was no difference among
the findings. However, in an attempt to determine an
the three groups at any time point in either average or
underlying mechanism for the drug-induced blunting
maximal soreness. Both average and maximal per-
of the postexercise increase in FSR, we measured pros-
ceived soreness for the three groups combined in-
taglandin (PG)F2␣ in the same muscle samples ana-
creased within 1 day postexercise (4 Ϯ 1 and 6 Ϯ 1),
lyzed for the measurement of FSR taken during the
peaked at 2 days postexercise (5 Ϯ 1 and 7 Ϯ 1), and
pre- and postexercise infusions (33). PGF2␣ is a product
returned to baseline by days 6 and 7 postexercise.
of the cyclooxygenase enzyme and has been shown tostimulate skeletal muscle protein synthesis (24, 30). DISCUSSION
Similar to the FSR results, PGF2␣ after exercise was
Given the mechanisms of action and the widespread
significantly increased (77%) in the PLA group,
use of ibuprofen and acetaminophen, we believed it
whereas it was unchanged in the ACET and IBU
was necessary to better understand the potential
groups (33). Thus it appears that both ACET and IBU
metabolic implications of consuming these over-the-
attenuate the postresistance exercise increase in FSR
counter drugs after eccentric resistance exercise. The
by blocking the production of PGF2␣ via the cyclooxy-
Table 2. Serum creatine kinase levels before and after the eccentric exercise bout
74 Ϯ 13 227 Ϯ 52 828 Ϯ 485 2,568 Ϯ 1,568 4,143 Ϯ 2,857 5,209 Ϯ 3,052 4,837 Ϯ 2,934 2,192 Ϯ 1,118 1,460 Ϯ 919 1,034 Ϯ 647
1,751 Ϯ 1,449 2,246 Ϯ 1,965 1,697 Ϯ 1,416
Values are means Ϯ SE and expressed as units per liter. Pre, preexercise; Post, hours after exercise. There were no differences (P Ͼ 0.05)
in the responses among the 3 groups. AJP-Endocrinol Metab • VOL 282 • MARCH 2002 • www.ajpendo.org
genase enzyme. These results, coupled with the fact
one used in the present study. It may appear somewhat
that the PGF2␣ measurements were completed on all
surprising that neither of these drugs provided any
eight subjects from each group, suggest that the effect
level of analgesia compared with placebo, given the
of ACET on postexercise FSR is valid.
aforementioned study and the proven pain-reducing
The implications of our data are important for those
benefits of acetaminophen and ibuprofen for individu-
individuals that chronically consume either ibuprofen
als with arthritis, headaches, and other symptoms (10,
or acetaminophen during a period in which muscle
11). However, the level of pain, soreness, and edema
hypertrophy is expected (i.e., resistance training). Al-
was high enough to severely inhibit the gait of the
though we did not measure the long-term effects of
subjects in our study during the days after the exercise
consumption of either of these drugs on muscle hyper-
bout. It is quite possible that the level of soreness and
trophy during resistance training, we speculate that
pain was too severe for the dose of these drugs to be
the continued attenuation of the normal increase in
effective. It is also possible that the scale used for the
protein synthesis after each resistance training bout
measurement of perceived soreness among the groups
would result in a blunting of the hypertrophic re-
was not able to discern small differences in soreness
sponse. Our speculation assumes that the muscle pro-
tein breakdown response coincides with the protein
We included only males in our study population, and
synthesis response. This assumption seems appropri-
it is unclear whether these same responses would hold
ate, since the resting and postresistance exercise skel-
in a similar group of females. However, there are no
etal muscle FSR and fractional breakdown rate have
data to suggest that the metabolism of ibuprofen or
been shown to be significantly correlated (26), suggest-
acetaminophen or the mechanism of action of these two
ing that these two processes are linked.
drugs is different between men and women. Further-
Our resting (preexercise) protein synthesis (FSR)
more, several studies of muscle protein metabolism at
results are comparable to previous studies of young to
rest and after resistance exercise have not shown a
middle-aged men in the postabsorptive state that have
difference between women and men (26, 27, 31, 38).
examined mixed muscle protein from the vastus late-
In conclusion, the increased rate of muscle protein
ralis (7, 29). The increase in FSR of the PLA group in
synthesis normally seen 24 h after high-intensity ec-
the current study (76%) also compares favorably with
centric resistance exercise was attenuated by con-
previous studies when training status, dietary state,
sumption of ibuprofen and acetaminophen at over-the-
muscle studied, and the amount of exercise are consid-
counter levels. The long-term influence of this acute
response after resistance exercise for individuals who
In this study, we used the Ra of phenylalanine as a
chronically consume these (or similar) drugs cannot be
measure of whole body protein breakdown. Our data
determined from this study. However, long-term use of
suggest, as others have found (26), that whole body
these drugs may inhibit the normal hypertrophic re-
protein breakdown is unchanged 24 h after resistance
sponse to resistance training. Future studies on the
exercise. Our data also suggest that neither ibuprofen
impact of chronic consumption of over-the-counter
nor acetaminophen had any influence on protein
doses of these drugs on skeletal muscle are warranted.
breakdown at the whole body level. To this end, Gannet al. (16) have shown that chronic consumption of the
We thank the subjects for their participation and effort, the
kitchen staff at the Nutrition, Metabolism, and Exercise Laboratory,
NSAID indomethacin does not affect whole body pro-
and Aaron Roland for the creatine kinase analysis.
tein synthesis or nitrogen retention in elderly subjects.
The work was supported by a grant from The McNeil Consumer
This finding is consistent with the fact that the action
Products Company (W. J. Evans) and National Institutes of Health
of the drugs in the current study appears to be at the
level of the skeletal muscle, and muscle protein metab-
REFERENCES
olism constitutes only about one-third of whole bodyprotein metabolism (21).
1. Abumrad NN, Rabin D, Diamond MP, and Lacy WW. Use of
a heated superficial hand vein as an alternative site for the
The exercise bout resulted in large increases in se-
measurement of amino acid concentrations and for the study of
rum CK activity and ratings of perceived muscle sore-
glucose and alanine kinetics in man. Metabolism 30: 936–940,
ness, which have been shown in previous studies (3,
13). The lack of effect of either drug on CK response to
2. Albert KS, Sedman AJ, Wilkinson P, Stoll RG, Murray WJ,
this type of exercise has also been reported (3, 9, 18),
and Wagner JG. Bioavailability studies of acetaminophen and nitrofurantoin. J Clin Pharmacol 14: 264–270, 1974.
although higher prophylactic doses of ibuprofen (5 days
3. Almekinders LC. Anti-inflammatory treatment of muscular
before; 2.4 mg/day) have been shown to reduce circu-
injuries in sport. An update of recent studies. Sports Med 28:
lating CK compared with placebo after eccentric mus-
cular activity (28). The lack of effect of similar over-
4. Barlas P, Craig JA, Robinson J, Walsh DM, Baxter GD, and Allen JM. Managing delayed-onset muscle soreness: lack of
the-counter analgesic drugs on ratings of perceived
effect of selected oral systemic analgesics. Arch Phys Med Reha-
muscle soreness has also been shown previously (3, 4,
9). However, Hasson et al. (18) reported that prophy-
5. Bergstrom J. Muscle electrolytes in man. Scand J Clin Lab
lactic and therapeutic doses of ibuprofen similar to
those used in the current study do reduce levels of
6. Biolo G, Fleming D, Maggi SP, and Wolfe RR. Transmem-
brane transport and intracellular kinetics of amino acids in
perceived muscle soreness 24 or 48 h after exercise
human skeletal muscle. Am J Physiol Endocrinol Metab 268:
with the use of a protocol that was less intense than the
AJP-Endocrinol Metab • VOL 282 • MARCH 2002 • www.ajpendo.org
7. Biolo G, Tipton KD, Klein S, and Wolfe RR. An abundant
25. Palmer RM, Reeds PJ, Atkinson T, and Smith RH. The
supply of amino acids enhances the metabolic effect of exercise
influence of changes in tension on protein synthesis and prosta-
on muscle protein. Am J Physiol Endocrinol Metab 273: E122–
glandin release in isolated rabbit muscles. Biochem J 214: 1011–
8. Bjorkman R. Central antinociceptive effects of non-steroidal
26. Phillips SM, Tipton KD, Aarsland A, Wolf SE, and Wolfe
anti-inflammatory drugs and paracetamol. Acta AnaesthesiolRR. Mixed muscle protein synthesis and breakdown after resis-
tance exercise in humans. Am J Physiol Endocrinol Metab 273:
9. Bourgeois J, MacDougall D, MacDonald J, and Tarnopol- sky M. Naproxen does not alter indices of muscle damage in
27. Phillips SM, Tipton KD, Ferrando AA, and Wolfe RR.
resistance-exercise trained men. Med Sci Sports Exerc 31: 4–9,
Resistance training reduces the acute exercise-induced increase
in muscle protein turnover. Am J Physiol Endocrinol Metab 276:
10. Bradley JD, Brandt KD, Katz BP, Kalasinski LA, and Ryan SI. Comparison of an antiinflammatory dose of ibuprofen, an
analgesic dose of ibuprofen, and acetaminophen in the treatment
28. Pizza FX, Cavender D, Stockard A, Baylies H, and Beighle
of patients with osteoarthritis of the knee. N Engl J Med 325:
A. Anti-inflammatory doses of ibuprofen: effect on neutrophils
and exercise-induced muscle injury. Int J Sports Med 20: 98–
11. Burnham TH and Short RM (Editors). Drugs Facts and Com- parisons. St. Louis, MO: Facts and Comparisons, 1999.
29. Rennie MJ, Edwards RHT, Halliday D, Matthews DE, Wol-
12. Chesley A, MacDougall JD, Tarnopolsky MA, Atkinson SA, man SL, and Millward DJ. Muscle protein synthesis mea- and Smith K. Changes in human muscle protein synthesis after
sured by stable isotope techniques in man: the effects of feeding
resistance exercise. J Appl Physiol 73: 1383–1388, 1992.
and fasting. Clin Sci (Colch) 63: 519–523, 1982.
13. Evans WJ and Cannon JG. The metabolic effects of exercise-
30. Rodemann HP and Goldberg AL. Arachidonic acid, prosta-
induced muscle damage. In: Exercise and Sport Sciences Re-
glandin E2 and F2␣ influence rates of protein turnover in skeletal
views, edited by JO Holloszy. Baltimore: Williams & Wilkins,
and cardiac muscle. J Biol Chem 257: 1632–1638, 1982.
31. Tipton KD, Ferrando AA, Phillips SM, Doyle D Jr, and
14. Ferreira SH. Prostaglandins, aspirin-like drugs and analgesia. Wolfe RR. Postexercise net protein synthesis in human muscle Nat New Biol 240: 200–203, 1972.
from orally administered amino acids. Am J Physiol Endocrinol
15. Flower RJ and Vane JR. Inhibition of prostaglandin syn- Metab 276: E628–E634, 1999.
thetase in brain explains the anti-pyretic activity of paracetamol
32. Tolman EL, Fuller BL, Marinan BA, Capetola RJ, Levin-
(4-acetamidophenol). Nature 240: 410–411, 1972. son SL, and Rosenthale ME. Tissue selectivity and variability
16. Gann ME, McNurlan MA, McHardy KC, Milne E, and Gar- lick PJ. Non-steroidal anti-inflammatory agents and protein
of effects of acetaminophen on arachidonic acid metabolism.
turnover in the elderly (Abstract). Proc Nutr Soc 47: 133A, 1988. Prostaglandins Leukotrienes Med 12: 347–356, 1983.
17. Harris JA and Benedict FG. A Biometric Study of Basal
33. Trappe TA, Fluckey JD, White F, Lambert CP, and Evans Metabolism in Man. Washington, DC: Carnegie Institution of
WJ. Skeletal muscle PGF2␣ and PGE2 in response to eccentric
resistance exercise: Influence of ibuprofen and acetaminophen.
18. Hasson SM, Daniels JC, Divine JG, Niebuhr BR, Rich- J Clin Endocrinol Metab 86: 5067–5070, 2001. mond S, Stein PG, and Williams JH. Effect of ibuprofen use
34. Vandenburgh HH, Hatfaludy S, Sohar I, and Shansky J.
on muscle soreness, damage, and performance: a preliminary
Stretch-induced prostaglandins and protein turnover in cultured
investigation. Med Sci Sports Exerc 25: 9–17, 1993.
skeletal muscle. Am J Physiol Cell Physiol 259: C232–C240,
19. Lockwood GF, Albert KS, Gillespie WR, Bole GG, Hark- com TM, Szpunar GJ, and Wagner JG. Pharmacokinetics of
35. Vane JR. Inhibition of prostaglandin synthesis as a mechanism
ibuprofen in man. I. Free and total area/dose relationships. Clin
of action for aspirin-like drugs. Nat New Biol 231: 232–235,
Pharmacol Ther 34: 97–103, 1983.
20. Matzke GR. Nonrenal toxicities of acetaminophen, aspirin, and
36. Vane JR. Towards a better aspirin. Nature 376: 215–216, 1994.
nonsteroidal anti-inflammatory agents. Am J Kidney Dis 28:
37. Volpi E, Mittendorfer B, Wolf SE, and Wolfe RR. Oral amino
acids stimulate muscle protein anabolism in the elderly despite
21. Nair KS. Muscle protein turnover: methodological issues and
higher first-pass splanchnic extraction. Am J Physiol Endocrinol
the effect of aging. J Geron Med Sci 50A: 107–112, 1995. Metab 277: E513–E520, 1999.
22. Newham DJ, Jones DA, and Edwards RHT. Large delayed
plasma creatine kinase changes after stepping exercise. Muscle
38. Welle S and Thornton CA. High-protein meals do not enhance
myofibrillar synthesis after resistance exercise in 62- to 75-yr-old
23. Newham DJ, Mills KR, Quigley BM, and Edwards RHT.
men and women. Am J Physiol Endocrinol Metab 274: E677–
Pain and fatigue after concentric and eccentric muscle contrac-
tions. Clin Sci (Colch) 64: 55–62, 1983.
39. Yarasheski KE, Campbell JA, Smith K, Rennie MJ, Hol-
24. Palmer RM. Prostaglandins and the control of muscle protein loszy JO, and Bier DM. Effect of growth hormone and resis-
synthesis and degradation. Prostaglandins Leukotrienes Essent
tance exercise on muscle growth in young men. Am J PhysiolFatty Acids 39: 95–104, 1990. Endocrinol Metab 262: E261–E267, 1992. AJP-Endocrinol Metab • VOL 282 • MARCH 2002 • www.ajpendo.org
Running heads: First page: Development in Practice, Volume 16, Number 6, November 2006 Verso: Mike Powell Recto: Which knowledge? Whose reality? GUEST INTRODUCTION Which knowledge? Whose reality? An overview of knowledge used in the development sector Mike Powell This article provides an overview of issues relating to the use of knowledge by development organisations. It starts
MEDICATION, VITAMINS, SURGERIES, & MORE Preventative Health Care As we age at some point everyone wil be diagnosed with some sort medical condition whether it be dry mouth or cancer, it does not matter. What matters is that you need to learn to become your own health care advocate. Everyone should at least have a primary care physician they see yearly. If you don’t have one, you should get
 Am J Physiol Endocrinol Metab 282: E551–E556, 2002.
Am J Physiol Endocrinol Metab 282: E551–E556, 2002.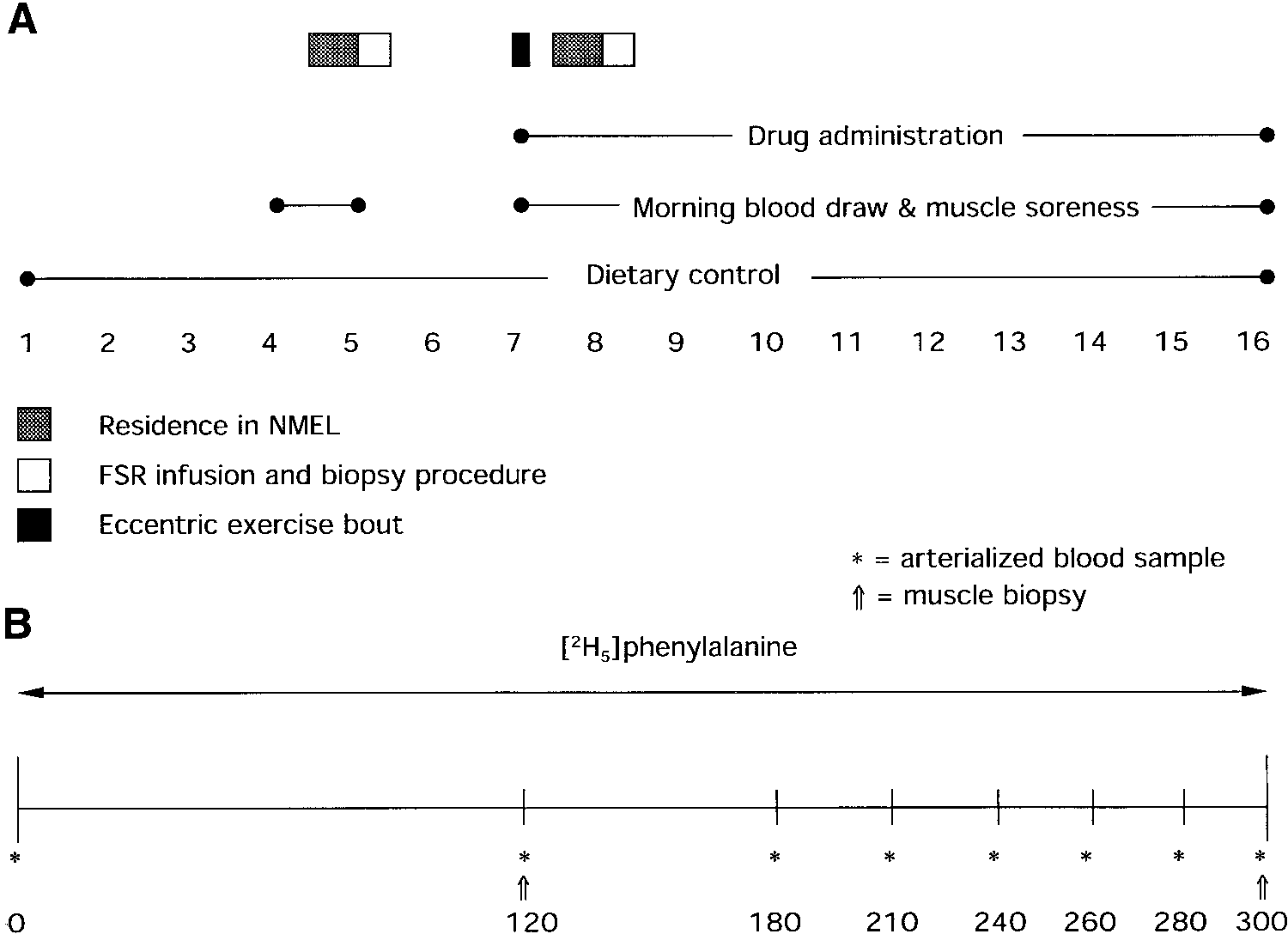 each morning and, if necessary to maintain body weight, thecarbohydrate and fat content of the diet was altered.
each morning and, if necessary to maintain body weight, thecarbohydrate and fat content of the diet was altered.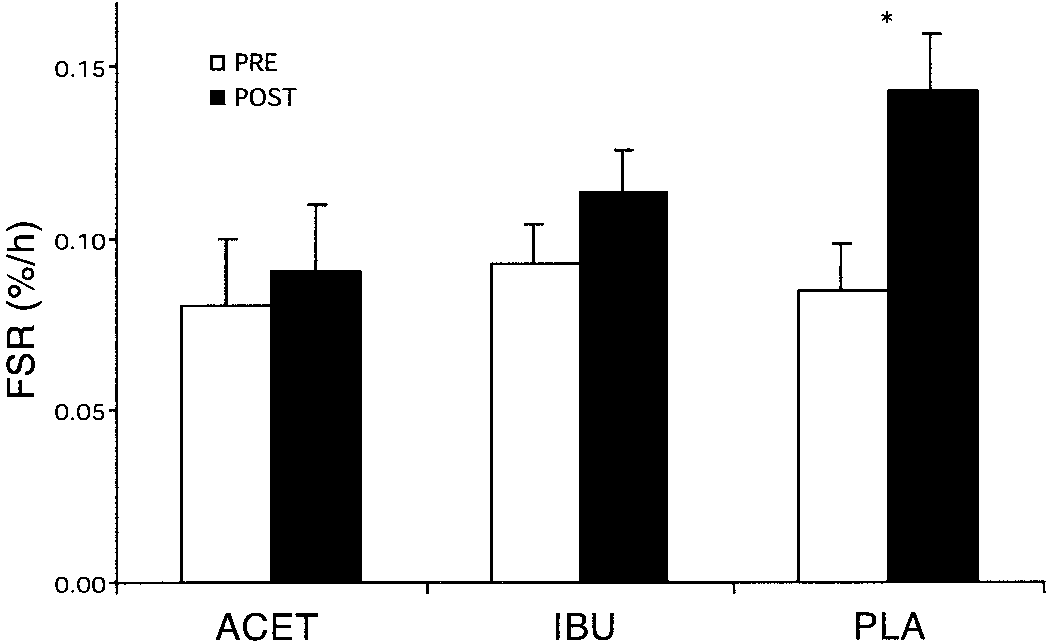 primary findings of this study were that ibuprofenblunted the protein synthesis response that is nor-mally seen after the type of exercise used in this study;surprisingly, acetaminophen also had a similar effecton protein metabolism.
primary findings of this study were that ibuprofenblunted the protein synthesis response that is nor-mally seen after the type of exercise used in this study;surprisingly, acetaminophen also had a similar effecton protein metabolism.