La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Sustained benefits of infliximab therapy for dermatologic and articular manifestations of psoriatic arthritis: results from the infliximab multinational psoriatic arthritis controlled trial (impact)
Vol. 52, No. 4, April 2005, pp 1227–1236
2005, American College of Rheumatology
Sustained Benefits of Infliximab Therapy for Dermatologic and
Articular Manifestations of Psoriatic Arthritis
Infliximab Multinational Psoriatic Arthritis Controlled Trial (IMPACT)
Christian E. Antoni,1 Arthur Kavanaugh,2 Bruce Kirkham,3 Zuhre Tutuncu,2
Gerd R. Burmester,4 Udo Schneider,4 Daniel E. Furst,5 Jerry Molitor,6 Edward Keystone,7
Dafna Gladman,7 Bernhard Manger,1 Siegfried Wassenberg,8 Ralf Weier,8 Daniel J. Wallace,9
Michael H. Weisman,9 Joachim R. Kalden,1 and Josef Smolen10
Objective. To investigate the efficacy and tolera- receive active treatment at the same dose through week bility of infliximab therapy for the articular and derma- 50. The primary efficacy outcome was achievement of tologic manifestations of active psoriatic arthritis (PsA). the American College of Rheumatology 20% criteria for Methods. One hundred four patients with PsA in improvement in rheumatoid arthritis (ACR20) at week whom prior therapy with at least 1 disease-modifying 16. Additional predefined clinical efficacy assessments antirheumatic drug (DMARD) had failed were recruited included the Psoriasis Area and Severity Index (PASI) into this investigator-initiated, multicenter, random- score, the ACR50 and ACR70 criteria, the Disease ized, double-blind, placebo-controlled clinical trial. Activity Score in 28 joints, the Health Assessment During the initial blinded portion of the study, patients Questionnaire, ratings of enthesitis and dactylitis, and received infusions of infliximab (5 mg/kg) or placebo at the Psoriatic Arthritis Response Criteria score. weeks 0, 2, 6, and 14. After week 16, patients initially Results. The proportion of infliximab-treated pa- assigned to receive placebo crossed over to receive tients who achieved an ACR20 response at week 16 infliximab 5 mg/kg every 8 weeks through week 50, while (65%) was significantly higher than the proportion of patients initially randomized to infliximab continued to
Dr. Antoni has received consulting fees of less than $10,000
Supported in part by the NIH (grant M01-RR-00827 to the
from Centocor and more than $10,000 from Schering-Plough. Dr.
University of California, San Diego), an unrestricted grant from
Kavanaugh has received consulting fees of less than $10,000 from
Centocor, Inc., to the University of Erlangen, Erlangen, Germany, and
Centocor. Dr. Kirkham has received consulting fees of less than
by the Schering-Plough Research Institute. Dr. Burmester’s work was
$10,000 from Schering-Plough, Wyeth, and Abbott. Dr. Burmester has
supported by the Competence Network “Inflammatory Rheumatic
received consulting fees of less than $10,000 from Schering-Plough.
Diseases” of the German Federal Ministry of Education and Science.
Dr. Furst has received consulting fees of less than $10,000 from
1Christian E. Antoni, MD (current address: Schering-Plough
Centocor. Dr. Molitor has received consulting fees of less than $10,000
Research Institute, Kenilworth, NJ), Bernhard Manger, MD, Joachim
from Bristol-Myers Squibb and Abbott. Dr. Keystone has received
R. Kalden, MD: Friedrich-Alexander University, Erlangen-
consulting fees of less than $10,000 from Centocor. Dr. Gladman has
Nuremberg, Germany; 2Arthur Kavanaugh, MD, Zuhre Tutuncu, MD:
received consulting fees of less than $10,000 from Centocor, Schering-
Center for Innovative Therapy, University of California, San Diego;
Plough, Amgen, and Wyeth. Dr. Manger has received honoraria of less
3Bruce Kirkham, MD: Guy’s Hospital, London, UK; 4Gerd R. Burm-
than $10,000 from Essex, Wyeth, Abbott, and Novartis. Dr. Weisman
has received consulting fees of less than $10,000 from Bristol-Myers
Germany; 5Daniel E. Furst, MD: University of California, Los Ange-
Squibb, Amgen, ISIS Pharmaceutical, Centocor, and Regeneron, and
les; 6Jerry Molitor, MD, PhD: Virginia Mason Clinic, Seattle, Wash-
has received consulting fees of more than $10,000 from Abbott and
ington; 7Edward Keystone, MD, Dafna Gladman, MD, FRCPC:
TAP Pharmaceutical Products. Dr. Smolen has received consulting
University of Toronto, Toronto, Ontario, Canada; 8Siegfried Wassen-
fees of less than $10,000 from Schering-Plough and Centocor.
berg, MD, Ralf Weier, MD: Evangelisches Fachkrankenhaus, Ratin-
Address correspondence and reprint requests to Christian E.
gen, Germany; 9Daniel J. Wallace, MD, Michael H. Weisman, MD:
Antoni, MD, 2015 Galloping Hill Road, Kenilworth, NJ 07033. E-mail:
Cedars-Sinai Medical Center, Los Angeles, California; 10Josef Smolen,
MD: Medical University of Vienna and Lainz Hospital, Vienna,
Submitted for publication July 30, 2004; accepted in revised
placebo-treated patients who achieved this response
role of TNF in these conditions. Etanercept, a dimeric
(10%). In addition, 46% of infliximab-treated patients
p75–TNF receptor/Ig Fc fusion construct, has been
achieved an ACR50 response, and 29% achieved an
shown to be effective in PsA (18,19) and psoriasis (20). ACR70 response; no placebo-treated patient achieved
Infliximab, a chimeric monoclonal antibody specific for
these end points. Among patients who had PASI scores
TNF␣, has also been shown to be effective in psoriasis
of >2.5 at baseline, 68% of infliximab-treated patients
(21). In an open-label study of infliximab in PsA, clinical
achieved improvement of >75% in the PASI score at
benefits were accompanied by objective improvements
week 16 compared with none of the placebo-treated
in inflammatory synovitis as measured using magnetic
patients. Continued therapy with infliximab resulted in
resonance imaging (22). On the basis of these results, we
sustained improvement in articular and dermatologic
conducted a controlled trial to evaluate the efficacy and
manifestations of PsA through week 50. The incidence of
safety of infliximab, using multiple assessments of skin
adverse events was similar between the treatment
and joint disease activity in patients with active PsA in
whom treatment with at least 1 DMARD had failed. Conclusion. Therapy with infliximab at a dose of 5 mg/kg significantly improved the signs and symptoms PATIENTS AND METHODS of arthritis, psoriasis, dactylitis, and enthesitis in pa- tients with active PsA that had been resistant to Patients. The study group comprised 104 patients DMARD therapy. With continued infliximab treatment,
(ages 18 years and older) with an established diagnosis of PsAof 6 months duration or longer. Eligibility criteria included
benefits were sustained through 50 weeks. The benefit-
previous failure of treatment with Ն1 DMARDs. At enroll-
to-risk ratio appeared favorable in this study popula-
ment, patients were required to have active peripheral polyar-
ticular arthritis, defined as the presence of Ն5 swollen andtender joints (based on joint counts of 66 and 68, respectively)
Psoriatic arthritis (PsA) is a chronic inflamma-
in conjunction with at least 1 of the following criteria: eryth-rocyte sedimentation rate (ESR) Ն28 mm/hour, C-reactive
tory arthropathy that occurs in association with psoriasis.
protein (CRP) level Ն15 mg/liter, and/or morning stiffness
Among articular disorders, PsA was once considered to
lasting 45 minutes or longer. Patients also were required to
have a relatively benign course; however, a growing body
have negative results of serum tests for rheumatoid factor and
of data suggest that PsA is often progressive and refrac-
negative results for active or latent tuberculosis by purified
tory to therapy. Moreover, patients with PsA may expe-
protein derivative skin test and chest radiography.
This study was conducted at 9 centers in Europe, the
rience substantial morbidity and unfavorable outcomes
US, and Canada, and the protocol was approved by the
(1,2). Although the disease course can be variable,
institutional review boards at each of the participating sites. All
factors such as polyarticular inflammation have been
patients provided written informed consent prior to participat-
associated with the development of deformities, radio-
ing in any study-related activities.
graphic joint damage, and impaired functional status
Study design. The study was conducted in 2 phases. In
phase 1, patients were randomly assigned to receive placebo
(3,4). Despite the recent data on leflunomide (5), re-
(n ϭ 52) or infliximab 5 mg/kg (n ϭ 52) at weeks 0, 2, 6, and
sponses to traditional disease-modifying antirheumatic
14. At the start of phase 2, in order to preserve the blinding
drugs (DMARDs) have been suboptimal, leaving an
and allow for a treatment introduction course for the placebo
group, patients in the infliximab group received placebo infu-
Recent advances in the understanding of the
sions at weeks 16 and 18, followed by infliximab 5 mg/kg atweeks 22, 30, 38, and 46; patients in the placebo group received
immunopathogenesis of psoriasis and PsA, combined
infliximab 5 mg/kg at weeks 16, 18, 22, 30, 38, and 46. Patients,
with developments in biotechnology, have led to the
investigators, and study personnel other than the pharmacist
introduction of novel therapeutic options (11). Several
were unaware of the initial assignments throughout the 50-
studies have suggested that proinflammatory cytokines,
in particular tumor necrosis factor ␣ (TNF␣), serve a key
Study agent. Infliximab (Remicade; Centocor,
Malvern, PA) was supplied in 20-ml vials containing 100 mg of
role in potentiating inflammatory responses associated
the lyophilized concentrate; placebo was identically formulated
with both psoriasis and PsA (12–17). Increased levels of
but did not contain infliximab. Infusions were administered
TNF␣ have been observed in skin, synovial fluid, and
over 2 hours by blinded personnel using an infusion set with an
synovial tissue from affected patients (14–16), and allelic
in-line, sterile, nonpyrogenic, low protein-binding filter (pore
polymorphisms in the promoter region for TNF␣ have
size 1.2 m) through a peripheral venous access site. Concomitant medications. Patients were allowed to
been shown to correlate with certain aspects of the
receive concomitant therapy with 1 of the following DMARDs:
disease (13). More recently, evidence from trials of
methotrexate (MTX; dosage of 15 mg/week or more, with folic
biologic agents targeting TNF have highlighted the key
acid supplementation), leflunomide, sulfasalazine, hydroxy-
chloroquine, intramuscular gold, penicillamine, or azathio-prine. For patients who were receiving a DMARD at the timeof enrollment, the dosage was required to have been stable forat least 4 weeks prior to randomization and to remain stablethroughout the study. Concomitant therapy with oral cortico-steroids (dosage of 10 mg prednisone equivalent/day or less)and nonsteroidal antiinflammatory drugs (NSAIDs) was per-mitted, provided that dosages had been stable for at least 2weeks prior to screening. Dosages of corticosteroids andNSAIDs were required to remain stable throughout the study. Use of intramuscular or intravenous corticosteroids, cyclo-sporine, or tacrolimus was prohibited within 4 weeks ofscreening and throughout the study. One injection of intraar-ticular corticosteroids was permitted in phase 2 of the study,and the injected joint would be excluded from subsequentefficacy assessment. Standard topical treatments for psoriaticlesions (e.g., topical steroids) were permitted, provided theyremained stable throughout the study. Therapy with psoralenultraviolet A was not permitted. Eligible patients could nothave received any investigational drug within 3 months ofscreening or any previous treatment with a monoclonal anti-body or fusion protein. Study procedures and evaluations. The primary effi-
cacy assessment was the achievement at week 16 of theAmerican College of Rheumatology 20% criteria for improve-ment (ACR20) in rheumatoid arthritis (RA) (23). Assessmentof skin involvement was made using the Psoriasis Area andSeverity Index (PASI) at the time of screening and at weeks 16and 50 (24). For the PASI, lesional erythema, scaling, andthickness were rated for 4 anatomic regions (head, trunk,upper extremities, and lower extremities). The area of eachanatomic region was factored into the overall score. The
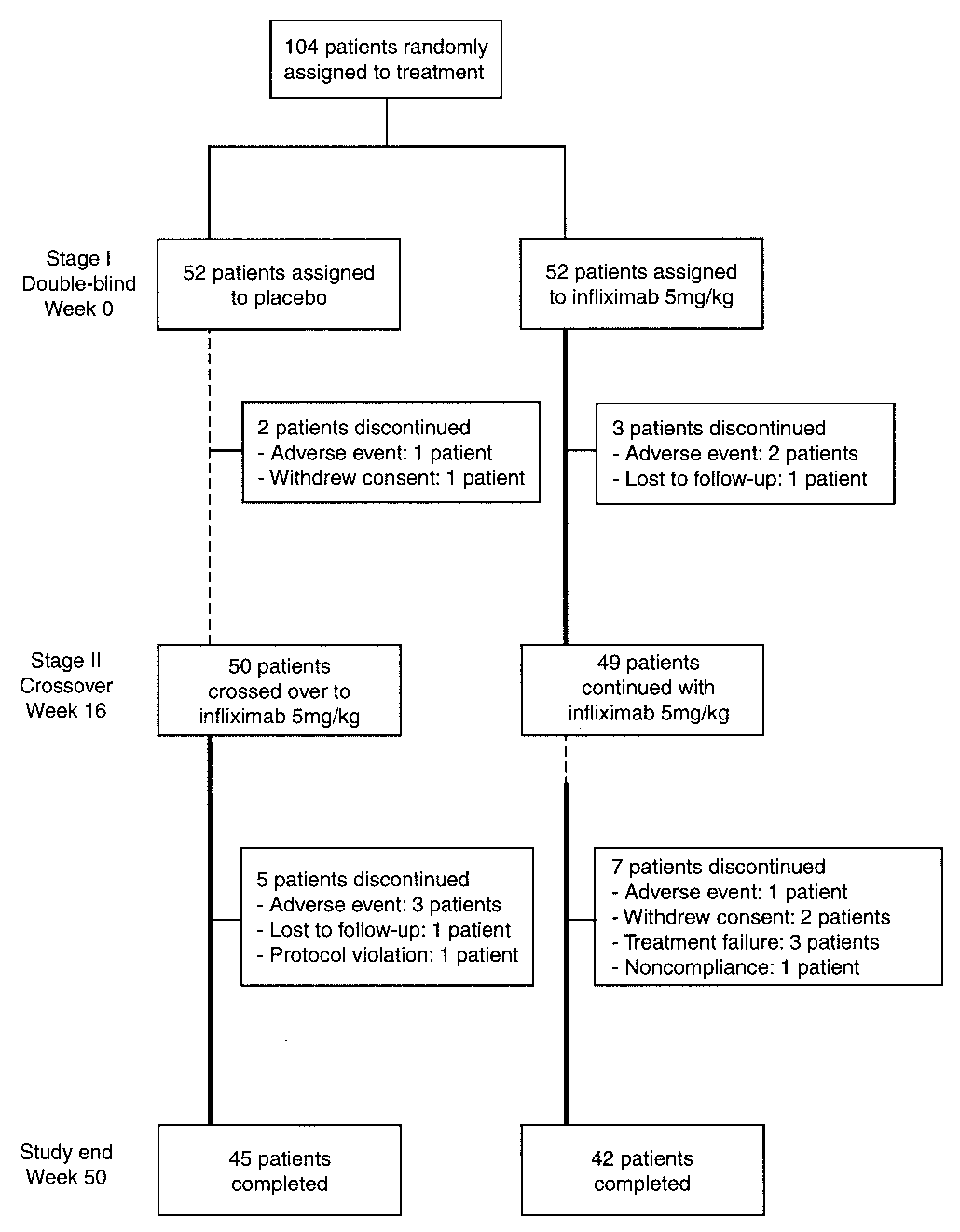
Figure 1. Study design and patient disposition. Broken line indicates
maximum possible PASI score is 72. Patients with a baseline
period during which patients were receiving placebo. Solid boldface
PASI score of Ն2.5 were included in the efficacy evaluation of
line indicates period during which patients were receiving infliximab 5
mg/kg. Patients initially assigned to the infliximab group received
Additional response evaluations made at weeks 2, 6,
infusions of placebo at weeks 16 and 18 in order to maintain blinding.
10, 14, 16, 18, 22, 30, 38, 46, and 50 included graded assess-ments of pain and swelling in 68 and 66 joints, respectively (0–3scale); the number of digits with dactylitis (maximum 20 digits;
Chi-square testing with Yates’ correction for contin-
0–3 scale); the Psoriatic Arthritis Response Criteria (PsARC)
gency tables was used to compare the primary efficacy end
(25); the Disease Activity Score in 28 joints (DAS28) (26,27);
point between the 2 treatment groups. To assess the onset of
the presence of enthesitis (at bilateral Achilles tendons and
clinical effect, the ACR20 response rates were assessed at
calcaneal insertions); patient’s and physician’s assessments of
weeks 2, 6, 10, and 14. The Mantel-Haenszel test was con-
pain and overall disease activity (0–10-cm visual analog scale);
ducted to estimate the common odds ratio of the 2 treatment
responses to the 20-question Health Assessment Question-
groups. In secondary efficacy analyses, the chi-square test was
naires (HAQ) (28); measurement of serum CRP levels; and
used for end points with discrete data, and a one-way analysis
determination of the ESR. Joints that had undergone surgical
of variance with treatment group as a factor was used for end
replacement or fusion operations were excluded from evalua-
tion. Joints that had undergone synovectomy within 12 monthsprior to screening or radiosynovectomy within the monthsprior to screening were also excluded from evaluation. Statistical analysis. The sample size calculation for
this trial was based on the assumption that 50% of infliximab-
Baseline characteristics, patient disposition, and
treated patients and 20% of placebo-treated patients would
concomitant therapy. Of the 104 enrolled patients, 99
achieve an ACR20 response. A sample size of 45 patients per
(95%) completed the study through week 16 (Figure 1).
group provided power of 0.8 and a 2-sided alpha value of 0.05.
A summary of baseline characteristics of the patients is
The predefined primary efficacy end point was the
provided in Table 1. The baseline characteristics for the
proportion of patients achieving an ACR20 response at week16 in the intent-to-treat analysis. The secondary end points
2 treatment groups were generally similar, with a few
were compared between treatment groups.
exceptions. The mean CRP value was 31.1 mg/liter in the
Baseline characteristics of the study population*
Global assessment of disease activity (0–10-cm VAS)
Patient’s assessment of pain (0–10-cm VAS)
Health Assessment Questionnaire (0–3 scale)
* Except where indicated otherwise, values are the mean Ϯ SD. PsA ϭ psoriatic arthritis; ACR20 ϭAmerican College of Rheumatology 20% criteria for improvement; VAS ϭ visual analog scale; PASI ϭPsoriasis Area and Severity Index. † Forty patients in the placebo group and 42 patients in the infliximab group were evaluated.
placebo group and 21.7 mg/liter in the infliximab group,
[65%]) was significantly higher than the proportion of
with medians of 14.0 mg/liter and 9.9 mg/liter, respec-
placebo-treated patients (5 of 52 [10%]) who achieved
tively (P ϭ 0.15). Patients in both treatment groups had
this end point (P Ͻ 0.001). In addition, at week 16, 24 of
active and severe psoriatic arthritis.
52 infliximab-treated patients (46%) achieved an
Five patients discontinued study treatment dur-
ACR50 response, and 15 of 52 infliximab-treated pa-
ing phase 1 (Figure 1). In the placebo group, 1 patient
tients (29%) achieved an ACR70 response; no placebo-
was withdrawn before the first infusion due to suspected
treated patient achieved these end points (P Ͻ 0.001)
atypical mycobacterial infection, and 1 patient withdrew
(Table 2). As shown in Figure 2, the response to
after the third infusion, at her request. In the infliximab
infliximab therapy was evident as early as week 2, and
group, 1 patient discontinued at week 16 due to a
improvement continued through the week 50 evaluation
suspected joint infection after a steroid injection into the
in patients initially randomized to infliximab. Following
wrist, 1 patient was lost to followup after 2 infusions, and
initiation of infliximab therapy, patients initially ran-
1 patient withdrew at week 14 after experiencing a lower
domized to placebo who received infliximab therapy at
respiratory tract infection and worsening of asthma.
weeks 16, 18, 22, 30, 38, and 46 exhibited a pattern of
During phase 2 of the study, when all patients were
clinical response similar to that of patients initially
receiving infliximab, 12 additional patients discontinued
randomized to infliximab (Table 2 and Figure 2).
treatment for the following reasons: adverse events (n ϭ
Among infliximab-treated patients, significant
4), patient request (n ϭ 3), treatment failure/lack of
improvement from baseline to week 16 was also ob-
benefit (n ϭ 3), and noncompliance and lost to followup
served in the individual components of the ACR20
(n ϭ 1 each). Data for all 104 patients were included in
(Table 2). In particular, the mean HAQ score improved
significantly from 1.2 at baseline to 0.6 at week 16 in
Efficacy. Articular manifestations. The proportion
infliximab-treated patients, while the mean HAQ scores
of infliximab-treated patients who achieved the primary
in placebo-treated patients showed no improvement (1.2
end point of an ACR20 response at week 16 (34 of 52
at baseline and week 16) (P Ͻ 0.001). By week 50, mean
mg/liter for the infliximab/infliximab and placebo/infliximab groups, respectively).
At the 16-week evaluation, 39 of 52 infliximab-
treated patients (75%) were improved according to thePsARC, compared with 11 of 52 placebo-treated pa-tients (21%) (P Ͻ 0.001). By week 50, the treatmentgroups showed similar PsARC response rates (76% and74% of patients in the placebo/infliximab and infliximab/infliximab groups, respectively). Infliximab-treated pa-tients also showed a significantly greater mean percentimprovement from baseline to week 16 in the dactylitisscore (85%) when compared with placebo-treated pa-tients (29%) (P Ͻ 0.001). Of note, 72% of infliximab-treated patients had a dactylitis score of 0 at week 16,compared with 31% of placebo-treated patients. Atbaseline, 25% of patients in each group had enthesitis; at
Figure 2. Percentages of patients achieving improvement by the
week 16, the proportion of infliximab-treated patients
American College of Rheumatology 20% criteria for improvement in
with enthesitis (14%) was significantly lower than the
rheumatoid arthritis (ACR20) through week 50. Arrows indicateweeks at which infusions were administered: open arrows denote
proportion of placebo-treated patients (31%; P ϭ
placebo (Pbo) infusions, and solid arrows denote infusions of inflix-
The mean baseline DAS28 scores (5.4 and 5.5 for
the placebo and infliximab groups, respectively) indicatethat the study population comprised patients with a high
HAQ scores were 0.7 and 0.5 in patients initially ran-
level of articular disease activity. At week 16, patients in
domized to placebo and infliximab, respectively. Despite
the infliximab group showed a mean improvement in the
slightly higher CRP values among placebo patients at
DAS28 score of 46%, compared with an improvement of
baseline, the median CRP values were similarly im-
2.8% among patients in the placebo group (P Ͻ 0.001).
proved at week 50 in both groups (9.9 mg/liter and 7.5
Furthermore, at week 16, 89% of patients in the inflix-
Summary of clinical efficacy parameters at weeks 16 and 50*
* For the American College of Rheumatology (ACR) parameters, values are the proportion (%) of patients meeting thecriteria for 20%, 50%, and 70% improvement. Except where indicated otherwise, all other values are the mean Ϯ SDpercent improvement (a negative value indicates worsening). CRP ϭ C-reactive protein; HAQ ϭ Health AssessmentQuestionnaire; DAS28 ϭ Disease Activity Score in 28 joints. † P Ͻ 0.001 versus placebo, for all comparisons. ‡ Week 16 results show number of patients with enthesitis at any time from baseline to week 16. Week 50 results shownumber of patients with enthesopathies at week 50.
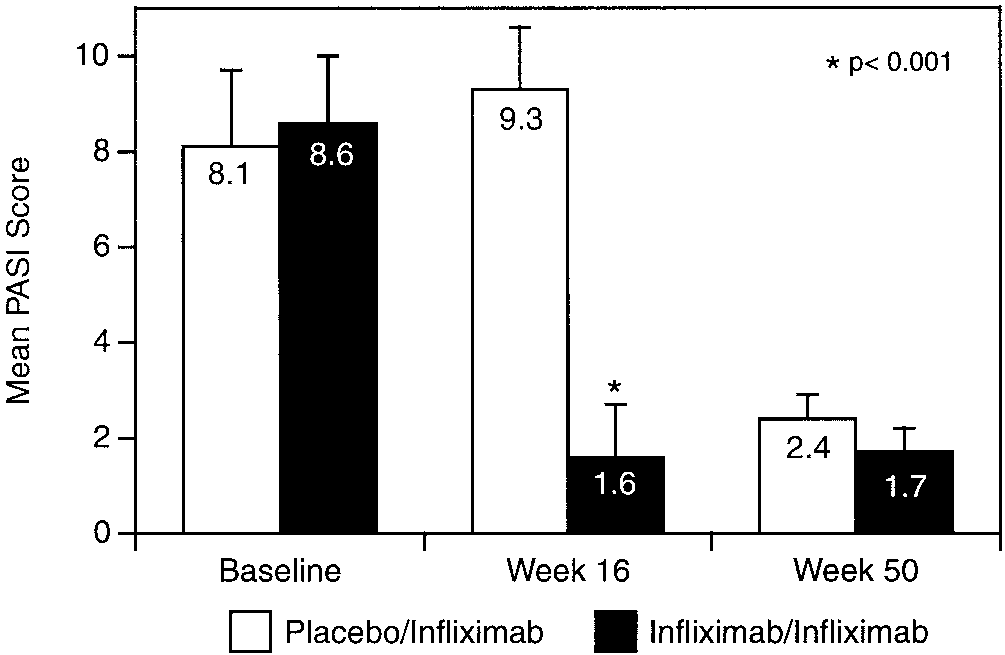
response following initiation of infliximab therapy (Fig-ure 4). At week 50 PASI scores were 2.4 and 1.7,respectively, in the placebo/infliximab and infliximab/infliximab groups. Looking at dermatologic responses inanother way, 100% (22 of 22), 68% (15 of 22), and 36%(8 of 22) of infliximab-treated patients experienced atleast 50%, 75%, and 90% improvement in the PASIscore from baseline to week 16. None of the placebo-treated patients achieved any of these end points at week16. At week 50, 50%, 75%, and 90% improvement in thePASI score was sustained in 86% (19 of 22 patients),59% (13 of 22 patients), and 41% (9 of 22 patients) ofpatients in the infliximab/infliximab group, respectively. By week 50, 69% (11 of 16), 50% (8 of 16), and 38% (6of 16) of patients in the placebo/infliximab groupachieved these end points. Figure 3. Values (mean Ϯ SD) for the Disease Activity Score in 28 joints (DAS28) during the 50-week treatment period. Broken lines Effect of concomitant DMARD use. Overall, 74 of
indicate the thresholds defining low disease activity (Ͻ3.2) and high
104 patients (71%) were receiving a concomitant
DMARD at baseline, including 41 of 52 patients in theplacebo group (79%) and 33 of 52 patients in theinfliximab group (63%) (P ϭ 0.08). The most commonly
imab group were DAS responders (i.e., had a good or
used DMARD was MTX; 34 patients in the placebo
moderate response according to the DAS28 criteria)
group were receiving a mean MTX dosage of 16.2
compared with 25% of patients in the placebo group
mg/week, and 24 patients in the infliximab group were
(P Ͻ 0.001). The treatment groups showed similar levels
receiving a mean MTX dosage of 15.9 mg/week. The
of improvement at week 50 (Table 2), with 82% of
concomitant use of DMARDs appeared to have little
patients in the infliximab/infliximab group and 84% of
effect on ACR20 response rates at week 16. Thus, 62.5%
patients in the placebo/infliximab group achieving a
of infliximab patients also receiving MTX achieved an
DAS28 response. Moreover, the mean DAS28 value
ACR20 response at week 16, as did 68% of infliximab
in both groups after initiation of infliximab therapy
patients not receiving MTX and 74% of those not
was below the threshold defining low disease activity
receiving any DMARDs (P not significant). Adverse events. A summary of adverse events by Dermatologic response. Baseline PASI scores
treatment group is provided in Table 3. The treatment
were similar between the 2 treatment groups (Table 1). Thirty-nine patients (22 in the infliximab group and 17 inthe placebo group) had PASI scores of Ն2.5 at baselineand were therefore eligible for evaluation of changes inskin scores during treatment. At week 16, patients in theinfliximab group had a mean improvement from base-line in their PASI score of 86%; this compared with a12% worsening in the PASI score for patients in theplacebo group (P Ͻ 0.001). Among patients with base-line PASI scores of Ն2.5, 68% of infliximab-treatedpatients achieved improvement of Ն75% in the PASIscore at week 16 compared with none of the placebo-treated patients (P Ͻ 0.001).
For patients initially assigned to infliximab treat-
ment, the response to infliximab therapy was sustainedthrough the week 50 evaluation. Patients initially ran-
Figure 4. Psoriasis Area and Severity Index (PASI) scores (mean and
domized to placebo, who received infliximab therapy
SD) at baseline, week 16, and week 50 in patients who had a PASI
after week 16, exhibited a similar pattern of PASI
* Values are the number (%). † One patient was randomly assigned to the placebo group but did not receive any infusions. This patient was included in theefficacy analysis but was excluded from the safety analysis.
groups were similar with regard to the incidence of all
ported during phase 2 included unrelated events of
adverse events, treatment-related adverse events,
inguinal hernia, surgical procedure (4 patients), angina
infusion-associated adverse events, severe adverse
pectoris, atrial fibrillation, urinary retention, chest pain,
events, and serious adverse events during both phase 1
and cerebrovascular event, as well as the following
(double-blind phase; weeks 0–16) and phase 2 (cross-
events with a possible or probable relationship to the
over phase; weeks 16–50) of the study.
study drug: fever, acute Salmonella gastroenteritis, pye-
The most frequently reported treatment-related
lonephritis, and leg weakness. The incidence of infusion
adverse events (i.e., those reported by Ն4 patients
reactions between groups was comparable in both
overall) during phase 1 of the study were as follows:
phases of the study (Table 3). One patient who received
headache (3 patients assigned to placebo and 4 patients
placebo in phase 1 followed by infliximab in phase 2 had
assigned to infliximab), bronchitis (4 placebo patients
dyspnea and urticaria at week 38, resulting in the only
and 3 infliximab patients), upper respiratory tract infec-
infusion-related study discontinuation.
tion (5 placebo patients and 1 infliximab patient),
No patients experienced an opportunistic infec-
influenza-like symptoms (4 placebo patients and 1 inflix-
tion, including tuberculosis, during the study. There
imab patient), rhinitis (2 placebo patients and 3 inflix-
were no reports of autoimmune, cytopenic, or neuro-
imab patients), and rash (2 placebo patients and 3
infliximab patients). During phase 2 of the study, themost frequently occurring treatment-related adverse
DISCUSSION
events were upper respiratory tract infection (23 pa-tients), headache (7 patients), dizziness (6 patients),
Although at one time PsA was considered to be a
influenza-like symptoms (5 patients), nonproductive
relatively benign condition, it is now known that PsA can
cough (5 patients), rhinitis (4 patients), hypertension (4
be associated with substantial morbidity, comparable
patients), and sinusitis (4 patients). Most treatment-
with that of RA, especially in patients with active
related adverse events were mild to moderate in inten-
polyarticular and oligoarticular PsA involving the large
sity. Severe treatment-related events were reported by 3
joints (3). Patients with PsA may also experience accel-
patients through week 16 (1 in the placebo group and 2
erated mortality and a significantly impaired quality of
in the infliximab group) and by 6 patients between week
life (2). However, in contrast to studies of RA, the use of
traditional DMARDs has not uniformly been shown to
Two patients reported serious adverse events
be associated with notable efficacy in randomized con-
during phase 1. One patient in the placebo group had
trolled trials of PsA, particularly with regard to treating
rectal bleeding due to diverticulitis, and 1 patient in the
cutaneous symptoms (25,29–31). Thus, patients with
infliximab group had synovitis suspected to be infectious
PsA, particularly those with severe disease, have an
that was culture negative. Serious adverse events re-
Patients in the Infliximab Multinational Psoriatic
and sustained improvement in skin psoriasis. At week
Arthritis Controlled Trial, all but 1 of whom were
16, the mean PASI score for patients with notable
negative for serum rheumatoid factor at baseline, had
psoriasis involvement at baseline (i.e., baseline PASI
severe refractory disease, as shown by their polyarticular
score of Ն2.5) was reduced in the infliximab group,
involvement, high global disease severity ratings, ele-
whereas the placebo group showed a slight worsening in
vated HAQ scores, high DAS28 scores, and their lack of
the mean PASI score. At week 16, a 50% improvement,
response to DMARD therapy. In addition, the majority
a 75% improvement, and a 90% improvement in the
of patients had skin involvement, approximately half had
PASI score was reached by 100%, 68%, and 36% of
dactylitis, and a quarter had enthesitis.
patients, respectively, in the infliximab treatment group
Assessments of improvement in the arthritis
and by none of the patients in the placebo group. After
symptoms of PsA in recent randomized controlled trials
crossing over to active treatment, patients in the
of DMARDs and biologic agents have focused primarily
placebo/infliximab group had skin response that mir-
on the ACR and PsARC criteria. Patients in this trial
rored those of patients in the infliximab group, and both
responded very well to infliximab treatment according to
groups were able to maintain the skin responses until
these assessments. The primary end point of the trial
week 50. Because of the relatively small number of
was clearly met, with 65% of patients in the infliximab
patients with substantial skin involvement, these results
group achieving an ACR20 response at week 16, com-
will have to be confirmed in a larger trial.
pared with 10% of patients in the placebo group; the
Although it is potentially tenuous to compare
response for infliximab-treated patients was maintained
results across trials, the articular responses noted in this
through week 50. The rapidity of response was notewor-
study of infliximab were quite comparable with those
thy, with many patients improving at the initial assess-
noted in 2 previous studies of etanercept in PsA (18,19).
ment (week 2). Furthermore, patients in the placebo
However, dermatologic responses in these studies of
group who crossed over to active treatment achieved a
etanercept appeared to be somewhat lesser than those
response that was similar in magnitude, rapidity, and
observed in this current trial of infliximab. Thus, at 12
sustainability to that of patients originally assigned to
weeks a 75% improvement in the PASI score was
achieved by 26% of etanercept-treated patients in one
In addition to the response shown with tradi-
study (18) and by 23% of etanercept-treated patients in
tional assessments of improvement in patients with PsA,
another study (19), with no placebo-treated patients in
to our knowledge this is the first published randomized,
either study achieving this end point. The reasons for the
controlled study that has also incorporated DAS28,
comparability of articular responses and the potential
enthesitis, and dactylitis assessments. The results
differentiation in dermatologic responses remain to be
showed that the study population consisted mostly of
fully delineated. Interestingly, whereas clinical efficacy
patients with high disease activity at baseline according
appears to be quite comparable among the various TNF
to the DAS28. It is noteworthy that the PsARC, ACR,
inhibitors in RA, differential efficacy has been noted in
and DAS28 criteria have not been validated for PsA.
Crohn’s disease, another systemic inflammatory auto-
However, in published trials, both the PsARC and the
ACR criteria have been used and have appeared to be
helpful. After treatment with infliximab, disease activity
among infliximab-treated patients in this trial is partic-
was significantly reduced at week 16, and the response
ularly noteworthy for this patient population; that is,
was maintained until week 50. The average DAS28
relatively young patients with the potential for many
response achieved was below the threshold defining low
additional years of productive work. HAQ scores in
disease activity. Enthesitis and dactylitis are common
patients initially treated with infliximab improved from
and clinically meaningful manifestations of PsA (32,33).
1.2 at baseline to 0.6 at week 16, while the HAQ scores
However, they have not received significant attention in
in patients receiving placebo showed no improvement
therapeutic trials. In the infliximab group in this study,
(1.2 at both baseline and week 16). By week 50, HAQ
significant reductions from baseline were observed in
scores were 0.7 and 0.5 in patients initially assigned to
mean dactylitis scores and the number of patients with
placebo and infliximab, respectively. These HAQ scores
enthesitis at week 16, and these responses were main-
represent a level of function that approaches what is
In addition to experiencing improvements in joint
Infliximab was generally well tolerated by all
symptoms, patients in the infliximab group showed rapid
study participants, and the safety profile observed in this
study was similar to previously reported findings
6. Veale DJ, FitzGerald O. Psoriatic arthritis: pathogenesis and
(21,34,35). The incidence of adverse events, treatment-
epidemiology. Clin Exp Rheumatol 2002;20 Suppl 28:S27–33.
7. Rahman P, Nguyen E, Cheung C, Schentag CT, Gladman DD.
related adverse events, infusion-associated adverse
Comparison of radiological severity in psoriatic arthritis and
events, severe events, serious adverse events, and ad-
rheumatoid arthritis. J Rheumatol 2001;28:1041–4.
verse events leading to discontinuation was similar be-
8. Gladman DD, Hing EN, Schentag CT, Cook RJ. Remission in
psoriatic arthritis. J Rheumatol 2001;28:1045–8.
tween placebo- and infliximab-treated patients.
9. Pipitone N, Kingsley GH, Manzo A, Scott DL, Pitzalis C. Current
In this trial, infliximab or placebo was added to
concepts and new developments in the treatment of psoriatic
the DMARD regimen that the patient was receiving at
arthritis. Rheumatology (Oxford) 2003;42:1138–48.
10. Kane D, Stafford L, Bresnihan B, Fitzgerald O. A prospective,
baseline. Overall, 56% of patients were receiving MTX
clinical and radiological study of early psoriatic arthritis: an early
at baseline, while 22% were receiving other DMARDs.
synovitis clinic experience. Rheumatology (Oxford) 2003:42:
Of note, the concomitant use of MTX or other
11. Bos JD, de Rie MA. The pathogenesis of psoriasis: immunological
DMARDs seemed to have little effect on the clinical
facts and speculations. Immunol Today 1999;20:40–6.
efficacy of infliximab. Whether there might be synergy in
12. Ettehadi P, Greaves MW, Wallach D, Aderka D, Camp RD.
clinical efficacy, alterations in dose response, or other
Elevated tumor necrosis factor-␣ (TNF-␣) biological activity inpsoriatic skin lesions. Clin Exp Immunol 1994;96:146–51.
interactions between infliximab and MTX or other
13. Hohler T, Kruger A, Schneider PM, Schopf RE, Knop J, Rittner
DMARDs, as has been suggested in RA (36), remains to
C, et al. A TNF-␣ promoter polymorphism is associated with
juvenile onset psoriasis and psoriatic arthritis. J Invest Dermatol1997;109:562–5.
In conclusion, infliximab was effective and gen-
14. Partsch G, Steiner G, Leeb BF, Dunky A, Broll H, Smolen JS.
erally well tolerated in patients with PsA who were
Highly increased levels of tumor necrosis factor-␣ and other
unresponsive to DMARD therapy. Infliximab at a dose
proinflammatory cytokines in psoriatic arthritis synovial fluid. J Rheumatol 1997;24:518–23.
of 5 mg/kg rapidly improved the signs and symptoms of
15. Ritchlin C, Haas-Smith SA, Hicks D, Cappuccio J, Osterland CK,
arthritis and significantly improved dermatologic mani-
Looney RJ. Patterns of cytokine production in psoriatic synovium.
festations, as shown by multiple assessments including
16. Danning CL, Illei GG, Hitchon C, Greer MR, Boumpas DT,
the ACR criteria, the DAS28, enthesitis, dactylitis, the
McInnes IB. Macrophage-derived cytokine and nuclear factor B
PsARC, and the PASI. The treatment effect was main-
p65 expression in synovial membrane and skin of patients with
tained throughout 1 year of therapy. Infliximab was
psoriatic arthritis. Arthritis Rheum 2000;43:1244–56.
17. Partsch G, Wagner E, Leeb BF, Dunky A, Steiner G, Smolen J.
generally well tolerated, and the benefit-versus-risk pro-
Upregulation of cytokine receptors sTNF-R55, sTNF-R75, and
file appeared to be favorable in this study population.
sIL-2R in psoriatic arthritis synovial fluid. J Rheumatol 1998;25:105–10.
18. Mease PJ, Goffe BS, Metz J, VanderStoep A, Finck B, Burge DJ. ACKNOWLEDGMENTS
Etanercept in the treatment of psoriatic arthritis and psoriasis: arandomised trial. Lancet 2000;356:385–90.
We thank the patients and study site personnel who
19. Mease PJ, Kivitz AJ, Burch FX, Siegel EL, Cohen S, Ory P, et al.
made this trial possible and Scott Newcomer from Centocor
Etanercept treatment of psoriatic arthritis: safety, efficacy, and
effect on disease progression. Arthritis Rheum 2004;50:2264–72.
20. Leonardi CL, Powers JL, Matheson RT, Goffe BS, Zitnik R,
Wang A, et al. Etanercept as monotherapy in patients with
REFERENCES
psoriasis. N Engl J Med 2003;349:2014–22.
21. Chaudhari U, Romano P, Mulcahy LD, Dooley LT, Baker DG,
1. Wong K, Gladman DD, Husted J, Long JA, Farewell VT. Mor-
Gottlieb AB. Efficacy and safety of infliximab monotherapy for
tality studies in psoriatic arthritis: results from a single outpatient
plaque-type psoriasis: a randomised trial. Lancet 2001;357:1842–7.
clinic. I. Causes and risk of death. Arthritis Rheum 1997;40:
22. Antoni C, Dechant C, Lorenz PD, Wendler J, Ogilvie A, Lueftl M,
et al. Open-label study of infliximab treatment for psoriatic
2. Gladman DD, Farewell VT, Wong K, Husted J. Mortality studies
arthritis: clinical and magnetic resonance imaging measurements
in psoriatic arthritis: results from a single outpatient center. II.
of reduction of inflammation. Arthritis Rheum 2002;47:506–12.
Prognostic indicators for death. Arthritis Rheum 1998;41:1103–10.
23. Felson DT, Anderson JJ, Boers M, Bombardier C, Furst D,
3. Gladman DD, Farewell VT, Nadeau C. Clinical indicators of
Goldsmith C, et al. American College of Rheumatology prelimi-
progression in psoriatic arthritis: multivariate relative risk model.
nary definition of improvement in rheumatoid arthritis. Arthritis
4. Queiro-Silva R, Torre-Alonso JC, Tinture-Eguren T, Lopez-
24. Fredriksson T, Pettersson U. Severe psoriasis: oral therapy with a
Lagunas I. A polyarticular onset predicts erosive and deforming
new retinoid. Dermatologica 1978;157:238–44.
disease in psoriatic arthritis. Ann Rheum Dis 2003;62:68–70.
25. Clegg DO, Reda DJ, Mejias E, Cannon GW, Weisman MH,
5. Kaltwasser JP, Nash P, Gladman D, Rosen CF, Behrens F, Jones
Taylor T, et al. Comparison of sulfasalazine and placebo in the
P, et al. Efficacy and safety of leflunomide in the treatment of
treatment of psoriatic arthritis: a Department of Veterans Affairs
psoriatic arthritis and psoriasis: a multinational, double-blind,
Cooperative Study. Arthritis Rheum 1996;39:2013–20.
randomized, placebo-controlled clinical trial. Arthritis Rheum
26. Van der Heijde DM, van ‘t Hof MA, van Riel PL, Theunisse LA,
Lubberts EW, van Leeuwen MA, et al. Judging disease activity in
clinical practice in rheumatoid arthritis: first step in the develop-
and symptomatic therapy in the treatment of psoriatic arthritis.
ment of a disease activity score. Ann Rheum Dis 1990;49:916–20.
27. Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de
32. Scarpa R. Peripheral enthesopathies in psoriatic arthritis. J Rheu-
Putte LB, van Riel PL. Modified disease activity scores that
include twenty-eight–joint counts: development and validation in a
33. Veale D, Rogers S, Fitzgerald O. Classification of clinical subsets
prospective longitudinal study of patients with rheumatoid arthri-
in psoriatic arthritis. Br J Rheumatol 1994;33:133–8.
tis. Arthritis Rheum 1995;38:44–8.
34. Maini R, St Clair EW, Breedveld F, Furst D, Kalden J, Weisman
28. Pincus T, Swearingen C, Wolfe F. Toward a Multidimensional
M, et al, and the ATTRACT Study Group. Infliximab (chimericanti-tumour necrosis factor ␣ monoclonal antibody) versus pla-
Health Assessment Questionnaire (MDHAQ): assessment of ad-
cebo in rheumatoid arthritis patients receiving concomitant meth-
vanced activities of daily living and psychological status in the
otrexate: a randomised phase III trial. Lancet 1999;354:1932–9.
patient-friendly health assessment questionnaire format. Arthritis
35. Lipsky PE, van der Heijde DM, St Clair EW, Furst DE, Breedveld
FC, Kalden JR, et al, and the Anti-Tumor Necrosis Factor Trial in
29. Hochberg MC, Silman AJ, Smolen JS, Weinblatt ME, Weisman
Rheumatoid Arthritis with Concomitant Therapy Study Group.
MH, editors. Rheumatology. 3rd ed. New York: Mosby; 2003.
Infliximab and methotrexate in the treatment of rheumatoid
30. Willkens RF, Williams HJ, Ward JR, Egger MJ, Reading JC,
arthritis. N Engl J Med 2000;343:1594–602.
Clements PJ, et al. Randomized, double-blind, placebo controlled
36. Maini RN, Breedveld FC, Kalden JR, Smolen JS, Davis D,
trial of low-dose pulse methotrexate in psoriatic arthritis. Arthritis
Macfarlane JD, et al. Therapeutic efficacy of multiple intravenous
infusions of anti–tumor necrosis factor ␣ monoclonal antibody
31. Salvarani C, Macchioni P, Olivieri I, Marchesoni A, Cutolo M,
combined with low-dose weekly methotrexate in rheumatoid ar-
Ferraccioli G, et al. A comparison of cyclosporin, sulfasalazine,
thritis. Arthritis Rheum 1998;41:1552–63.
ACNE THERAPY Experience with Palomar LuxV™ Intense Pulsed Light Therapy Robert S. Berger, MD, FAAD, FASDS., Assistant Professor, Department of Dermatology,The Johns Hopkins University, Baltimore, Private Practice, Waldorf, MarylandCathleen S. Berger, RN, BSN, Waldorf, MarylandAcne is a disease that affects almost 100% of the popu-hair (bangs as well as shoulder length). Some feel acne
Trana Discovery, Inc. Management Team Biographies Steve Peterson, Chief Executive Officer Steve brings 30 years of experience in drug development and commercialization to Trana Discovery. His career spans several major pharmaceutical companies including Eli Lilly, Glaxo and GlaxoWellcome where he held positions in sales, marketing, product development and as liaison with ke
 chloroquine, intramuscular gold, penicillamine, or azathio-prine. For patients who were receiving a DMARD at the timeof enrollment, the dosage was required to have been stable forat least 4 weeks prior to randomization and to remain stablethroughout the study. Concomitant therapy with oral cortico-steroids (dosage of 10 mg prednisone equivalent/day or less)and nonsteroidal antiinflammatory drugs (NSAIDs) was per-mitted, provided that dosages had been stable for at least 2weeks prior to screening. Dosages of corticosteroids andNSAIDs were required to remain stable throughout the study.
chloroquine, intramuscular gold, penicillamine, or azathio-prine. For patients who were receiving a DMARD at the timeof enrollment, the dosage was required to have been stable forat least 4 weeks prior to randomization and to remain stablethroughout the study. Concomitant therapy with oral cortico-steroids (dosage of 10 mg prednisone equivalent/day or less)and nonsteroidal antiinflammatory drugs (NSAIDs) was per-mitted, provided that dosages had been stable for at least 2weeks prior to screening. Dosages of corticosteroids andNSAIDs were required to remain stable throughout the study.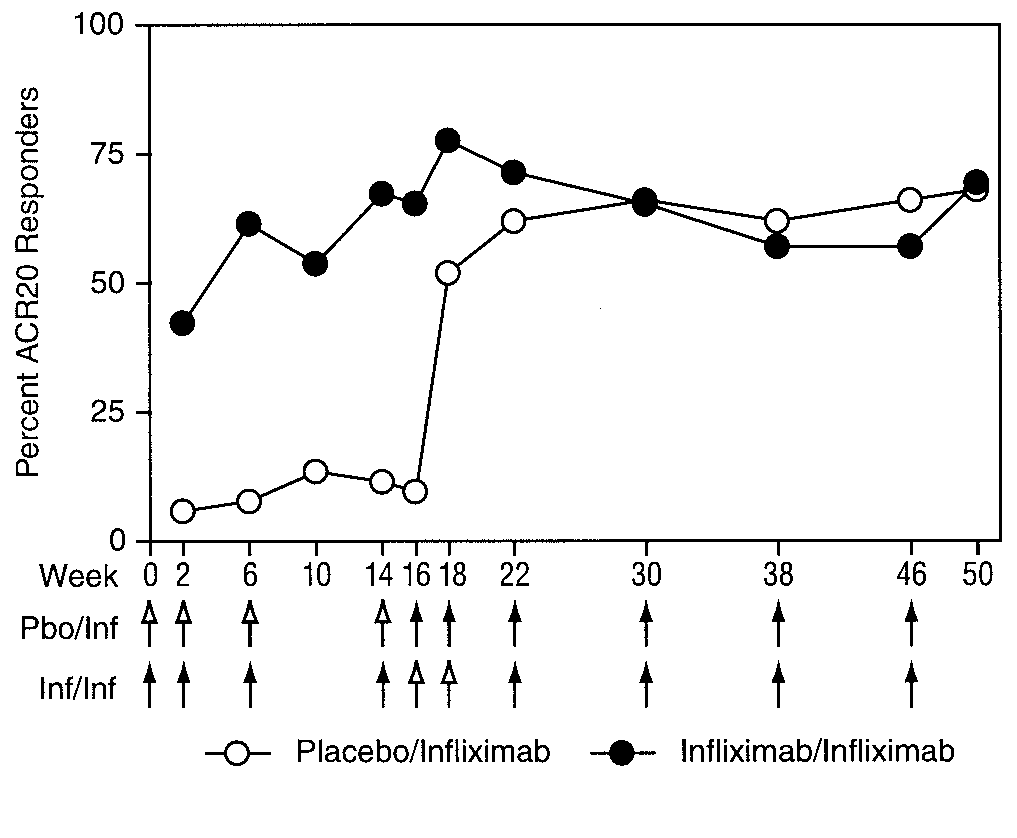 mg/liter for the infliximab/infliximab and placebo/infliximab groups, respectively).
mg/liter for the infliximab/infliximab and placebo/infliximab groups, respectively).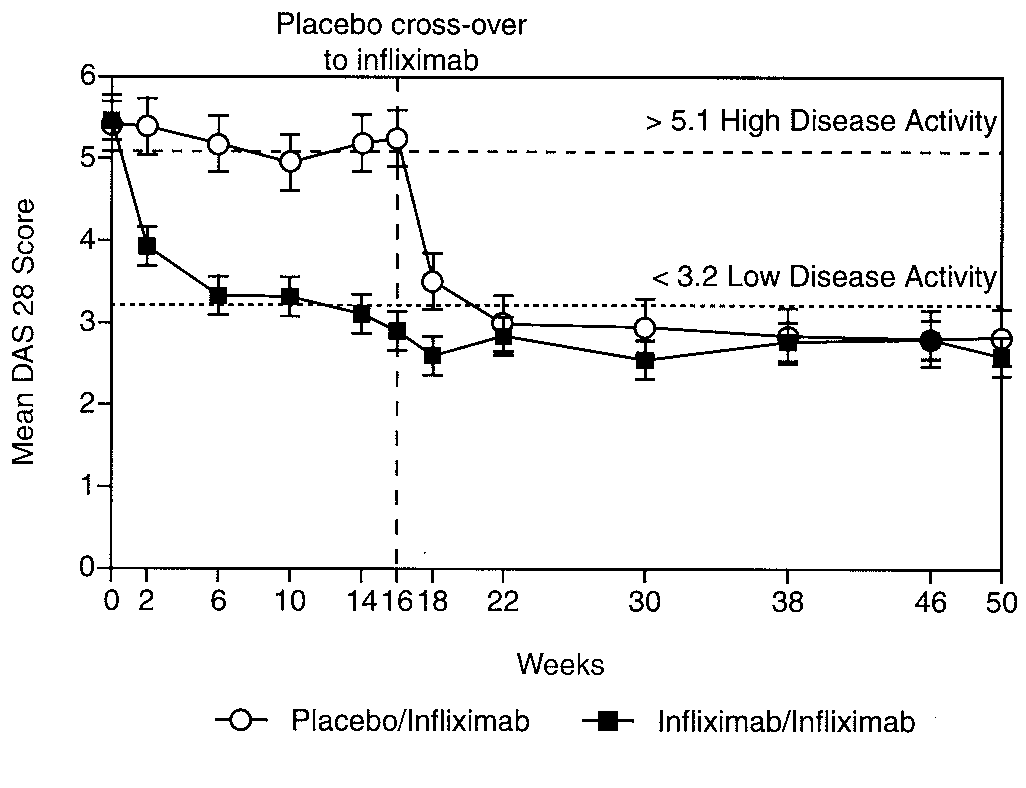
 response following initiation of infliximab therapy (Fig-ure 4). At week 50 PASI scores were 2.4 and 1.7,respectively, in the placebo/infliximab and infliximab/infliximab groups. Looking at dermatologic responses inanother way, 100% (22 of 22), 68% (15 of 22), and 36%(8 of 22) of infliximab-treated patients experienced atleast 50%, 75%, and 90% improvement in the PASIscore from baseline to week 16. None of the placebo-treated patients achieved any of these end points at week16. At week 50, 50%, 75%, and 90% improvement in thePASI score was sustained in 86% (19 of 22 patients),59% (13 of 22 patients), and 41% (9 of 22 patients) ofpatients in the infliximab/infliximab group, respectively.
response following initiation of infliximab therapy (Fig-ure 4). At week 50 PASI scores were 2.4 and 1.7,respectively, in the placebo/infliximab and infliximab/infliximab groups. Looking at dermatologic responses inanother way, 100% (22 of 22), 68% (15 of 22), and 36%(8 of 22) of infliximab-treated patients experienced atleast 50%, 75%, and 90% improvement in the PASIscore from baseline to week 16. None of the placebo-treated patients achieved any of these end points at week16. At week 50, 50%, 75%, and 90% improvement in thePASI score was sustained in 86% (19 of 22 patients),59% (13 of 22 patients), and 41% (9 of 22 patients) ofpatients in the infliximab/infliximab group, respectively.