La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Hip replacement
A Patient’s Guide to Hip Replacement Dr Ashish Mittal, MBBS, MS(Orth), MRCS, MCH(Orth), Diploma in Sports & Exercise Medicine (London) Consultant Orthopaedic Surgeon
The Royal Orthopaedic & Sports Injury Center, Jaipur & Kota
Understanding Your Hip Replacement Surgery INTRODUCTION
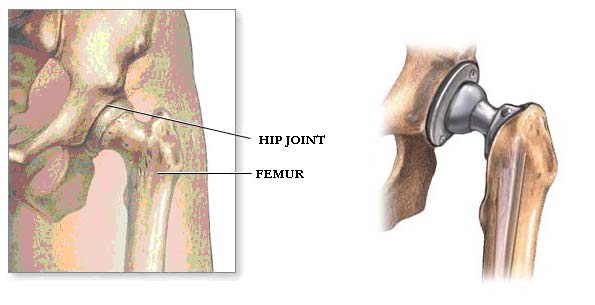
A Hip replacement is an operation for serious arthritis of the hip. To understand your total hip replacement you should first understand a little about the structure of the hip joint. The hip joint is a ball and socket joint with the ball component attached to the top of the femur (the long bone of the thigh). The socket is part of the pelvis. These ends are covered by a slippery material called cartilage.
This allows the hip to glide easily when moving. The ball rotates in the socket to permit you to move your leg backward, forward, sideways and in a twisting motion Arthritis damages the surfaces where the parts of your hip slide over each other. The worn cartilage no longer serves as a cushion and the damaged bones rub together, they become rough, with a surface like sandpaper. This hurts, and stops your hip moving the way it should. It also makes your hip weak and sometimes makes your leg painful and shorter in length.
This is a picture of a healthy hip, and to the right, a total hip replacement
BEFORE YOUR HIP REPLACEMENT SURGERY
It important that, despite the discomfort in your hip, you remain as mobile and active as possible. This will maintain your muscle strength and improve the speed and quality of you recovery form the surgery. If you smoke, then this is an ideal opportunity to consider giving up. Smoking increases a number of potential complications following surgery and to gain the full benefit you should stop at least 6 weeks before your surgery. The pre assessment visit before surgery
You will undergo a number of tests and x-rays, you will receive a clinical examination and have a consultation with me. I will make sure you understand the procedure and potential pitfalls / complications. You will then be asked to sign the Consent form. This is a document stating you understand what is involved and want to proceed with the surgery. You will receive a copy of this document. The Night Prior to Surgery
You will be asked not to eat or drink anything for 6 hours before your surgery. THE OPERATION What type of anaesthesia is used in my Hip Replacement Surgery?
Most of our hip replacement patients receive, epidural or spinal anaesthesia, however general anaesthesia is also used in certain patients. Your anaesthetist will discuss the type of anaesthesia used with you prior to surgery.
With epidural or spinal anaesthesia, a narrow catheter is placed between two bones of your spine. A controlled flow of anaesthetic goes through the narrow catheter, anaesthetising your body from the abdomen down so you will not feel anything during surgery. You will also be offered a sedative so that you are asleep for the operation.
If you are undergoing general anaesthesia, you will first be put to sleep by IV medication. A mask or a breathing tube then gives an anaesthetic gas to keep you asleep. What is involved in my Hip Replacement Surgery?
A hip replacement is a big operation. It generally takes 1 to 1 1⁄2 hours. I will make an incision over the side of your hip / buttock and remove the arthritic ends of the ball and socket. I will then replace these with a combination of metal, polyethylene or ceramic implants. The combination of components I will use for you will depend on your age, level of activity and the type of arthritis you have. The components are either ‘press fit’ into the bone, or held using screws or a medical glue we call cement.
Explain to your relatives / friends that you will be away form the ward for up to 4 hours. The theatre schedule is flexible and no specific time can be given to you as to when in the day your surgery will occur. After surgery is completed you will be moved to the recovery area in the operating
department for a short time. You will then be transferred to your ward bed where your relatives and friends will be allowed to be with you. Is there much Pain with Hip Replacement Surgery?
Normally following your surgery you will experience a little pain. If following the surgery you are experiencing severe pain, please inform the nurse. The nurse will notify the Doctor who will then make an assessment and provide you with appropriate pain medication. We aim to keep your pain scores below 4 out of 10. RECOVERING FROM YOUR HIP REPLACEMENT SURGERY
A dressing over the hip and mid thigh area will be present. Normally this is left untouched and will be changed on the day prior to your discharge. It may be necessary to change the dressing earlier, particularly if you have some minor bleeding from the wound.
I will use a type of stitch to close your incision that is buried beneath the skin and will dissolve with time. This means there are no stitches / staples to remove.
You may have a foam wedge pillow between your legs. This is to help keep your new hip in place during early healing .
You may have a drain from the surgical site. This drainage tube collects any bloody fluid that has accumulated under the skin and muscle. This tube is usually removed the day after surgery
A bar (trapeze) will be hanging over the bed. Use it to help lift your body when you change positions
An IV (intravenous infusion) will be running fluid into your arm.
Vital signs will be taken which consist of blood pressure, pulse, respiratory rate and temperature
You may have a catheter (urine bag) to monitor the amount and colour of your urine. This is usually removed 1 or 2 days after surgery
You can normally drink fluids and eat as soon as your appetite returns.
It will normally take 3 days to become fully mobile following your Hip Replacement Surgery, and you should expect to go home within 2-3 days of the surgery. Please remember that each person is different so times will vary, if you are older or in poor physical condition, or not very mobile it may take longer to recover from your surgery.
Please note that after Hip Replacement Surgery it is not recommended to drive for 2 months. Check with you insurance company if in doubt. REHABILITATION AND PHYSIOTHERAPY
Your participation in physical therapy is essential to the success of your surgery. The more committed and enthusiastic you are, the quicker your improvement and recovery will be. You will receive extensive physiotherapy during your stay in the hospital, and we will make sure you are safe and mobile prior to your discharge. A physiotherapist will visit you on the day after surgery and will start to
instruct you on the exercise program. You will receive physiotherapy each day following the surgery and we strongly encourage you to achieve three goals before discharge. The physiotherapist will guide you through your recovery. Please take note of the ward staff and physiotherapists advice when you commence your mobilisation for the first time.These sessions are normally one on one with a physiotherapist. If it is deemed necessary for you to have outpatient physiotherapy, this will be organized prior to your discharge home. ALTERNATIVES, BENEFITS AND POTENTIAL PROBLEMS ALTERNATIVES Do I need this operation ? Lots of people have arthritis in their hips and only a small number need a hip replacement. Total hip replacement surgery is very successful in eliminating pain form the arthritic hip. When your pain has reached a level where your hip wakes you from sleep, restricts your mobility, or stops you from doing things you used to do, such as working, going out with friends and family, gardening, housework or shopping you are suitable for a hip replacement surgery. It will reduce / eliminate your pain and improve your mobility.
If you have reached this stage the only alternatives to replacement surgery are continued non operative treatment with pain killers, weight loss, walking aids and physiotherapy.
If you choose not to have this operation, your arthritis will not get better but the disease usually progresses very slowly, often over many years. Your pain and stiffness may even ease a little with
time. Having arthritis can make your life more difficult, but it's unlikely to make it shorter. If you are younger (< 60 years old) or have less severe arthritis, alternatives which may exist include keyhole surgery to wash out the hip (Arthroscopy) or breaking and re-setting your bone (Osteotomy). The goal of this surgery is to restore the joint to its correct position, which helps to distribute weight evenly in the joint. For some people, an osteotomy relieves pain. Recovery from an osteotomy takes 6 to 12 months. After an osteotomy, the function of the hip joint may continue to worsen and the patient may need additional treatment. The length of time before another surgery is needed varies greatly and depends on the condition of the joint before the procedure. Not all patients are suitable for these procedures and I do not perform either of them myself. I would however be happy to discuss them with you.
BENEFITS
Hip replacement surgery is continually evolving, however is very successful in treating the pain of arthritis. It is not an operation to give you back a ‘normal’ hip, but aims to provide a painless hip with adequate movement for the majority of daily activities. Success of hip replacement surgery depends upon many factors of which rehabilitation is of utmost importance. The most perfectly performed surgery can be quickly undone by inappropriate or unsupervised rehabilitation, particularly in the early stages following surgery. POTENTIAL COMPLICATIONS
These are uncommon, but may occur occasionally: Bleeding into the hip joint / wound may require draining in the immediate postoperative period. Infection (2%) may result in redness / heat in the skin of the thigh or groin. DO NOT TREAT WITH ANTIBIOTICS until you have contacted your surgeon. Bruising around your hip, thigh or buttocks is common and not of great significance. Dislocation (3%) occurs when the artificial hip jumps out of joint. There are many different causes for this and if it occurs in the initial period will be treated with a manipulation under anaesthesia.
Activities that predispose to dislocation will be discussed with you by your physiotherapist. Nerve injury (1%) may result in weakness of your thigh or calf muscle leaving you with a ‘dropped foot’. This is usually temporary but occasionally permanent. Thrombotic disease. Blood clots in the legs (10%) and in the lungs (1%) can occur. We take precautions to minimise the risks of these and after the surgery will give you medication to thin the blood slightly. We will also ask you to wear anti-thrombotic stockings until 6 weeks following your surgery. Becoming active and mobile soon after the surgery will also reduce your risks. If these clots do occur you will be prescribed Warfarin (a blood thinning medication) to take. Leg Length difference. It is likely that before the operation, due to the arthritis, your legs were of slightly different lengths. We aim to restore normal lengths during the operation but occasionally, we have to adjust the leg length to achieve a stable joint. This is unusual and if it occurs only rarely will you notice it. If you do you may need a build up on your shoe. Loosening. This is an artificial joint. It has a finite life span and although techniques and implants are constantly evolving the recognised life span of most hip replacement is 10 yrs in 90% of patients. If the replacement wears out you may experience further discomfort and require a revision (re-do) procedure. General medical / anaesthetic problems. This is a big operation and will put strain on your lungs and heart. A small number of people have serious problems such as a heart attack, a stroke, or a bad chest infection soon afterwards. These things are more likely to happen if you already have heart disease, or a bad chest. It is a good idea to stop smoking before an operation because smoking makes all these problems more likely. QUESTIONS
If you have questions about your surgery please ask one of my team at the pre-assessment clinic or once admitted for surgery. If you have questions about your rehabilitation please contact your physiotherapist.
If you have any problems, especially if you experience any excessive skin redness, persistent wound discharge, excessive swelling, or severe pain, please call Dr Mittal’s secretary on the numbers on the
front of this pack, or call the ward where you had your surgery.
Call your GP immediately if you develop calf pain and tightness, shortness of breath, or if you develop a fever and feel unwell.
So that you do not forget in clinic, please use this space to write down any questions you may have for me.
SEGUE DALLA PRIMA Gentile direttore , (…) gli uomini d'affari cinesi a investire inBertinotti; al principio, il rifiuto di ogniItalia e a fidarsi di noi, questo poco edifican-offerta di dimissioni e, alla fine, il sacrificiote "caso" ha fatto sempre da sottofondo, dan-necessario dell'"amico Angelo". neggiando l'immagine pubblica del governo. La vera novità è
WASTEWATER TREATMENT SYSTEM TANK PUMPING INSTRUCTIONS These instructions provide a general guideline concerning when and how to pump out the Singulair system. This literaturesupplements other instructional materials included in the Singulair Bio-Kinetic System Service Manual. In order to maximize performance, protect system components and insure protection of the surrounding environment










 A Patient’s Guide to Hip Replacement
A Patient’s Guide to Hip Replacement 





 You may have a catheter (urine bag) to monitor the amount and colour of your urine. This is usually removed 1 or 2 days after surgery
You can normally drink fluids and eat as soon as your appetite returns.
It will normally take 3 days to become fully mobile following your Hip Replacement Surgery, and you should expect to go home within 2-3 days of the surgery. Please remember that each person is different so times will vary, if you are older or in poor physical condition, or not very mobile it may take longer to recover from your surgery.
Please note that after Hip Replacement Surgery it is not recommended to drive for 2 months. Check with you insurance company if in doubt.
You may have a catheter (urine bag) to monitor the amount and colour of your urine. This is usually removed 1 or 2 days after surgery
You can normally drink fluids and eat as soon as your appetite returns.
It will normally take 3 days to become fully mobile following your Hip Replacement Surgery, and you should expect to go home within 2-3 days of the surgery. Please remember that each person is different so times will vary, if you are older or in poor physical condition, or not very mobile it may take longer to recover from your surgery.
Please note that after Hip Replacement Surgery it is not recommended to drive for 2 months. Check with you insurance company if in doubt.