La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Metabolic improvements in obese type 2 diabetes subjects implanted for 1 year with an endoscopically deployed duodenal–jejunal bypass liner
DIABETES TECHNOLOGY & THERAPEUTICSVolume 14, Number 2, 2012
ª Mary Ann Liebert, Inc. DOI: 10.1089/dia.2011.0152
Metabolic Improvements in Obese Type 2 Diabetes
Subjects Implanted for 1 Year with an Endoscopically
Eduardo G.H. de Moura, M.D., Ph.D.,1 Bruno C. Martins, M.D.,1 Guilherme S. Lopes, M.D.,1
Ivan R. Orso, M.D.,1 Suzana L. de Oliveira, B.S.,1 Manoel P. Galva˜o Neto, M.D.,2 Marco A. Santo, M.D.,3
Paulo Sakai, M.D., Ph.D.,1 Almino C. Ramos, M.D.,2 Arthur B. Garrido Ju´nior, M.D.,3
Marcio C. Mancini, M.D.,4 Alfredo Halpern, M.D., Ph.D.,4 and Ivan Cecconello, M.D., Ph.D.3
Background: The purpose of this study was to evaluate the effect of the duodenal–jejunal bypass liner (DJBL), a60-cm, impermeable fluoropolymer liner anchored in the duodenum to create a duodenal–jejunal bypass, onmetabolic parameters in obese subjects with type 2 diabetes. Methods: Twenty-two subjects (mean age, 46.2 – 10.5 years) with type 2 diabetes and a body mass index between40 and 60 kg/m2 (mean body mass index, 44.8 – 7.4 kg/m2) were enrolled in this 52-week, prospective, open-label clinical trial. Endoscopic device implantation was performed with the patient under general anesthesia, andthe subjects were examined periodically during the next 52 weeks. Primary end points included changes infasting blood glucose and insulin levels and changes in hemoglobin A1c (HbA1c). The DJBL was removedendoscopically at the end of the study. Results: Thirteen subjects completed the 52-week study, and the mean duration of the implant period for allsubjects was 41.9 – 3.2 weeks. Reasons for early removal of the device included device migration (n = 3), gas-trointestinal bleeding (n = 1), abdominal pain (n = 2), principal investigator request (n = 2), and discovery of anunrelated malignancy (n = 1). Using last observation carried forward, statistically significant reductions in fastingblood glucose ( - 30.3 – 10.2 mg/dL), fasting insulin ( - 7.3 – 2.6 lU/mL), and HbA1c ( - 2.1 – 0.3%) were ob-served. At the end of the study, 16 of the 22 subjects had an HbA1c < 7% compared with only one of 22 atbaseline. Upper abdominal pain (n = 11), back pain (n = 5), nausea (n = 7), and vomiting (n = 7) were the mostcommon device-related adverse events. Conclusions: The DJBL improves glycemic status in obese subjects with diabetes and therefore represents anonsurgical, reversible alternative to bariatric surgery.
because of the increased risk of diabetes-associated morbidity,including heart disease, peripheral vascular disease, stroke,
The prevalence of obesity (defined as having a body kidney disease, retinopathy, and neuropathy.
mass index [BMI] of ‡ 30 kg/m2) is increasing in both
Treatment of diabetes is focused on glycemic control and
developing as well as developed countries.1 Obesity is a major
typically proceeds in a stepwise fashion when target glycemic
risk factor for type 2 diabetes,2 and thus it is not surprising
goals are not reached or maintained.7,8 The initial steps are
that the global prevalence of type 2 diabetes continues to in-
lifestyle changes aimed at controlling diet and increasing ac-
crease.3 In 2010, the estimated global prevalence of diabetes
tivity with the goal of reducing body weight, followed by the
among adults was 6.4% and is projected to increase to 7.7% by
addition of orally active pharmacologic agents (sulfonylureas,
2030.4 In Brazil, the 2006 prevalence of diabetes based on self-
metformin) and insulin to the treatment regimen.7,8
reports was 5.3%,5 although higher estimates have been re-
Of interest is the observation that obese patients with dia-
ported.6 This increasing prevalence of diabetes is alarming
betes who undergo certain gastric bypass procedures
1Gastrointestinal Endoscopy Unit, 3Gastrointestinal Surgery Unit, Gastroenterology Department, and 4Endocrinology Department,
University of Sa˜o Paulo Medical School, Sa˜o Paulo, Brazil.
2Gastro Obeso Center, Sa˜o Paulo, Brazil.
demonstrate improvement in glycemia, often within days of
disease or other GI disease, pancreatitis, symptomatic coro-
surgery and before significant weight loss.9,10 The mechanism
nary artery disease or pulmonary dysfunction, known gall-
responsible for this improvement is not fully understood;
stones, severe coagulopathy, upper GI bleeding conditions
however, the surgical rearrangement of the anatomy of the
(e.g., esophageal or gastric varices, congenital or acquired
gastrointestinal (GI) tract changes the location where partially
intestinal telangiectasia), congenital or acquired anomalies of
digested nutrients first contact the intestine, suggesting that
the GI tract (e.g., atresias or stenoses), inability to discontinue
correction of dysfunctional homeostatic mechanisms may
nonsteroidal anti-inflammatory drugs during the study, pre-
contribute to the glycemic improvement.11
vious GI surgery that could interfere with placement of the
A nonsurgical method of altering the location of the initial
device, or family or patient history of a known diagnosis or
contact of partially digested nutrients with the intestine is by
symptoms of systemic lupus erythematosus, scleroderma, or
use of the duodenal–jejunal bypass liner (DJBL).12,13 The DJBL
other autoimmune connective tissue disorder.
consists of a 60-cm, impermeable fluoropolymer liner and anitinol anchor, which reversibly fixes the device to the wall of
the duodenum. The DJBL is open at both ends and functions
The study was a 52-week, prospective, open-label, single-
to prevent the partially digested food from contacting the
center clinical trial intended to assess the safety and efficacy of
proximal intestine. A pilot study of the DJBL in obese subjects
the DJBL in obese subjects with type 2 diabetes. Following
with type 2 diabetes resulted in a mean reduction of 50 mg/dL
screening and up to 30 days prior to implanting the DJBL,
in fasting plasma glucose (FPG) after 1 week that was sus-
baseline demographics and medical history were obtained.
tained through 24 weeks.14 Here we describe a 52-week study
Excess body weight was calculated as the amount of body
that was designed to investigate the effect of the DJBL on
weight that exceeded a BMI of 25 kg/m2. In addition, a
metabolic parameters in obese subjects with type 2 diabetes.
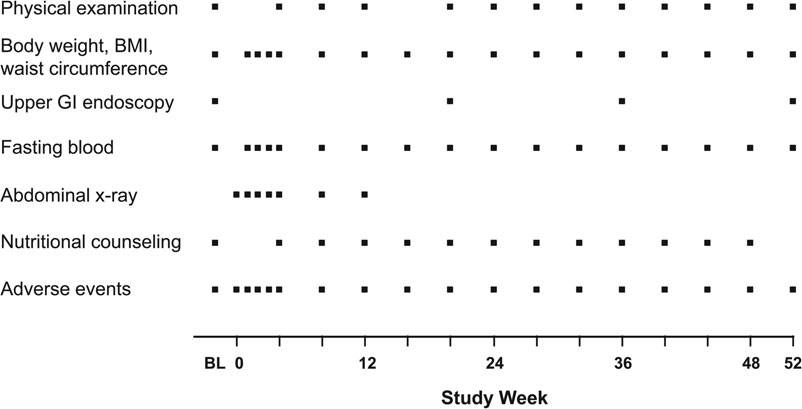
physical examination, electrocardiogram, chest x-ray, liver,biliary duct, and pancreas ultrasound, upper GI endoscopy,
and fasting blood tests were conducted. A schedule of study
assessments and activities is presented in Figure 1. In accor-dance with the protocol, all subjects received nutritional
This study was conducted in compliance with international
counseling at the baseline visit and at all monthly follow-up
guidelines and local country regulations. The study protocol
visits. Baseline counseling consisted of a 30-min visit with a
and subject informed consent forms were reviewed and ap-
study nurse to discuss nutritional, behavioral, and lifestyle
proved by the Ethics and Research Committee of the Uni-
modifications recommended throughout the study. At follow-
versity of Sa˜o Paulo, Sa˜o Paulo, Brazil. All subjects or their
up visits, subjects were only asked if they were following
legal guardians provided written informed consent prior to
their diet, and results were recorded. Therefore, nutritional
counseling was minimal at the post-implant follow-up visits. During the period starting 3 days prior to device implantation
and ending 2 weeks after explantation of the device, subjects
Male and female subjects with type 2 diabetes between the
were instructed to take an over-the-counter proton pump in-
ages of 18 and 65 years who had a BMI of ‡ 40 and < 60 kg/m2
hibitor (40 mg twice a day). Daily multivitamin and iron
were eligible for inclusion in the study. Exclusion criteria in-
supplements were also recommended throughout the study.
cluded use of prescription anticoagulation therapy, iron de-
Subjects were instructed to follow a liquid diet during the first
ficiency or iron deficiency anemia, inflammatory bowel
2 weeks following implantation and to gradually transition to
Schedule of study assessments. BL, baseline; BMI, body mass index; GI, gastrointestinal.
DUODENAL–JEJUNAL BYPASS LINER AND DIABETES
a normal diet over the next 10 days. Follow-up examinations
were to be conducted 1, 3, and 6 months after the explantation
All device implantations were performed with the patient
under general anesthesia using a minimally invasive endo-
scopic procedure.13 At the end of the study period (or earlier if
indicated by an adverse event), the DJBL was removed en-
doscopically using a custom grasper passed through the
working channel of a standard endoscope with the patient
under conscious sedation for 21 of 22 subjects; one subject
The DJBL (EndoBarrier Gastrointestinal LinerÒ) and the
implantation and removal devices were manufactured by GI
Several subject populations were included in the analyses.
The safety analysis population included all subjects in whom
an implant procedure was attempted. The full efficacy anal-
ysis population included all enrolled subjects in whom an
implantation was successful. The completer population in-
cluded all subjects who completed the 52-week implantation
The study had two primary efficacy end points: percentage
change in excess body weight and change in type 2 diabetes
status, including hemoglobin A1c (HbA1c) and fasting blood
glucose and insulin levels. Secondary efficacy end points in-
cluded changes in blood lipid levels and blood pressure.
All statistical analyses were performed using SASÒ version
9.2 or later (SAS Institute, Cary, NC). Efficacy variables were
evaluated as a change from baseline. Missing values were not
imputed. However, last observation carried forward (LOCF)
on or before explantation was also used when calculating
change from baseline. A P value (calculated using Student’s
t test) of £ 0.05 was considered statistically significant.
Twenty-two subjects were screened, and all were enrolled
in the study. The baseline characteristics of the study subjects
BMI, body mass index; GERD, gastroesophageal reflux disease;
are presented in Table 1. At baseline, 17 of 22 subjects were
HbA1c, hemoglobin A1c; HDL, high-density lipoprotein; LDL, low-
receiving drugs to control their diabetes, including 11 re-
ceiving metformin alone, two receiving glibenclamide alone,two receiving chlorpropamide alone, one receiving metfor-min plus glibenclamide, and one receiving metformin plus
weeks after implantation. Subsequent computed tomography
acarbose. A DJBL was successfully implanted in all subjects,
scan revealed a 30-cm abdominal tumor that was identified as
with the procedure taking an average of 26.7 – 11.0 min
metastatic ovarian cancer. This event was considered not re-
Thirteen subjects completed the 52-week period, and 18
Baseline FPG, fasting plasma insulin, and HbA1c levels are
subjects completed at least 24 weeks. The mean duration of
presented in Table 1, and changes in these parameters are
the implant period for all subjects was 41.9 – 3.2 weeks. The
shown in Table 2. Reductions in FPG were seen as early as
reasons for early removal of the device were migration or
week 1 and reached statistical significance at week 24. At
rotation of the device (n = 3; 36, 36, and 48 weeks post-
week 52, the completer population demonstrated a decrease
implantation), GI bleeding (n = 1; 4 weeks post-implantation),
in plasma glucose of - 37.1 – 11.8 mg/dL (mean – SEM,
abdominal pain (n = 2; 21 and 30 weeks post-implantation),
P < 0.01). A similar reduction was seen in the full analysis
and principal investigator request due to subject’s noncom-
population using LOCF analysis (Table 2). Mean HbA1c was
pliance with study visits (n = 2; 20 and 32 weeks post-
statistically significantly decreased by week 24 and remained
implantation). The device was removed from one subject who
statistically significantly decreased thereafter (Table 2). The
presented with fever and mild abdominal symptoms 17
decrease in HbA1c was evident in subgroups of subjects with
Data are mean – SEM values (number of patients).
aP < 0.01, bP < 0.001, cP < 0.0001, dP < 0.05 for change from baseline. HbA1c, hemoglobin A1c; LOCF, last observation carried forward.
baseline HbA1c < 8%, 8% to < 10%, and ‡ 10% (Fig. 2). The
Blood levels of total cholesterol, low-density lipoprotein
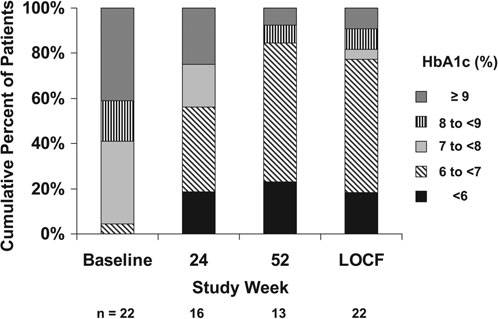
progressive improvement in HbA1c is illustrated in Figure 3.
cholesterol, and triglycerides were significantly reduced
At baseline, only one subject (4.5%) had an HbA1c level below
during the study (Table 3). Nonsignificant decreases in mean
7%. For final HbA1c measurement, 16 of 22 subjects (73%) had
systolic (6.6 – 4.4 mm Hg, P = 0.15, LOCF) and diastolic
an HbA1c below 7%. In the nine subjects who experienced an
( - 1.6 – 3.5 mm Hg, P = 0.65, LOCF) blood pressure were ob-
early device explantation, HbA1c decreased from 8.9 – 0.5% at
baseline to 7.2 – 0.4% at final measurement (median, 28
Sixteen subjects had HbA1c measured 3 and/or 6 months
after explantation of the DJBL. These subjects demonstrated a
During the study, nine subjects experienced no change in
mean decrease in HbA1c during the original 52-week study of
their diabetes medications, three subjects reduced their dose
- 2.3 – 0.4%. Three and 6 months after removal of the device,
of metformin, and one subject stopped other diabetes medi-
their mean changes from baseline were - 2.3 – 0.3% (n = 15)
cation. One subject who was previously untreated began
and - 1.7 – 0.7% (n = 11), respectively.
treatment with metformin, five subjects increased their dose
All 22 subjects reported at least one treatment-emergent
of metformin, and three subjects added an additional drug to
adverse event. Treatment-emergent adverse events that oc-
curred in ‡ 10% of the subjects are presented in Table 4. The
Figure 4 shows the percentage change in excess body
most common adverse events that were deemed to be possi-
weight observed during the study. The 13 subjects who
bly or probably related to the device or procedure were GI
completed the study weighed 121.8 – 7.6 kg (mean – SE) at
disorders, including upper abdominal pain, nausea, and vo-
baseline and 101.6 – 5.7 kg at week 52. This change re-
miting. With one exception, all adverse events were mild or
presented a mean loss of excess body weight (percentage ex-
moderate in severity. The one exception was the 43.5-year-old
cess weight loss) of 39.0 – 3.9% (P < 0.0001). In the full analysis
white woman in whom metastatic ovarian cancer was dis-
population using LOCF, the mean percentage excess weight
covered 17 weeks after device implantation (see above). No
loss was 35.5 – 3.1% (P < 0.0001). The reduction in excess body
weight (LOCF) was reflected by reductions in BMI and waistcircumference of - 6.7 – 0.7 kg/m2 and - 13.0 – 1.7 cm, re-
The present study represents the longest evaluation of the
safety and efficacy of the DJBL in obese patients with type 2diabetes. The mean duration of the DJBL implant was 41.9weeks; 18 subjects completed at least 24 weeks, and 13
Change in hemoglobin A1c (HbA1c) in subgroups
of subjects. No statistical analysis was performed on thesedata. SE bars are hidden within symbols at some time points.
Distribution of hemoglobin A1c (HbA1c) levels
BL, baseline; LOCF, last observation carried forward.
during the study. LOCF, last observation carried forward.
DUODENAL–JEJUNAL BYPASS LINER AND DIABETES
Other clinical studies provide anecdotal observations of the
effect of the DJBL on type 2 diabetes. In the initial 12-weekstudy of the DJBL, four of the 12 obese subjects had type 2diabetes;15 the authors reported that ‘‘all 4 diabetic patientshad normal FPG levels without hypoglycemic medication forthe entire 12 weeks. Of those 4 patients, 3 had decreased he-moglobin A1c of 0.5% by week 12.’’ A second study enrolled40 obese subjects who were candidates for Roux-en-Y gastricbypass and randomly assigned them to either DJBL (n = 26, 25implanted) or low-calorie diet alone (n = 14) with the objectiveof weight loss before surgery.16 Three subjects with type 2diabetes were included in the DJBL group, and one was in-cluded in the diet group. After 12 weeks, two of the three DJBLsubjects demonstrated decreases in HbA1c, and the third,who had a baseline HbA1c of 5.5%, was able to discontinue
Percentage excess weight loss by visit. The number
of subjects represented by each point is shown above the x-
diabetes medications within 1 week of implantation. A similar
axis. The dotted line reflects the loss of excess body weight in
12-week study randomly assigned obese subjects to either
the completer population during the study.
DJBL (n = 30) or low-calorie diet (n = 11).13 Eight subjects withtype 2 diabetes were included in the DJBL group and dem-onstrated a reduction in mean HbA1c from 8.8 – 1.7% at
subjects completed the entire 52-week study. During the 52-
baseline to 7.7 – 1.8% after 12 weeks (P reported as nonsig-
week study, substantial improvements in diabetes status were
nificant). Six of the eight subjects were able to reduce their
seen as shown by the decreased blood glucose and HbA1c
dosage of oral diabetes medication or insulin after 1 week, and
levels in the study population (Table 2 and Figs. 2 and 3). The
at 12 weeks, one subject had completely stopped taking an-
improvement in glycemic control is convincingly demon-
strated by the results presented in Figure 3, which shows that
In the present study, device-related early removal of the
the percentage of subjects with HbA1c < 7% at baseline im-
DJBL occurred in six of the 22 (27%) subjects after a median of
proved from 4.5% to 73.0% at final study assessment. It is
31 weeks. There were three non–device-related early remov-
important that the improvements in HbA1c were seen re-
als: one after 17 weeks due to a metastatic ovarian tumor and
gardless of baseline value (Fig. 2).
two (weeks 20 and 32, respectively) due to principal investi-
A single previous study of the DJBL for the treatment of
gator request as subjects were noncompliant with study visits.
type 2 diabetes has been reported.14 In that pilot study, 12
In previous studies, device-related early explantation oc-
obese patients with type 2 diabetes received a DJBL, and a
curred in 15–33% of subjects after a median of 21 days (range,
comparable control group of six patients underwent a sham
3–120 days, n = 18).12–16 Although the early explantation rate
procedure. After 1 week, FPG had declined significantly in the
of the present study was high, these subjects still derived a
DJBL group ( - 50 – 18 mg/dL, mean – SE) compared with the
metabolic benefit from the DJBL; at their last measurement,
sham group ( + 25 – 29 mg/dL, P = 0.042). In addition, post-
HbA1c was 7.2% compared with a baseline value of 8.9%.
prandial glucose excursions were improved in the DJBL
Based on the safety results of previous clinical studies of the
group but not in the sham group. Of interest is the observation
DJBL, no unanticipated adverse events were observed. The
that at the 1-week time point, the improvement in glucose
primary device-related safety issues seen in the present study
metabolism seen in the DJBL could not be explained by
were GI pain, nausea, vomiting, and back pain (Table 4). All
changes in body weight, as both groups had experienced the
cases were mild to moderate in severity. Two subjects cited
same median weight change from baseline (about - 3.5 kg).
abdominal pain as the reason for requesting early explanta-
The improvements in glucose metabolism were sustained
tion of the device. It is important that the rates of GI or ab-
through the end of the study (mean, 200 – 22 days [28.6
dominal pain adverse events appeared to be similar to those
weeks]). At week 24, FPG had declined by 83 – 39 mg/dL
reported in previous studies, suggesting that the longer im-
(from a baseline of 199 – 71 mg/dL), and HbA1c had declined
plant duration of the present study was not responsible for an
by 2.4 – 0.7% (from a baseline of 9.2 – 1.7%).
increased incidence of these events.
Data are mean – SEM values (number of patients).
aP < 0.05, bP < 0.01 for change from baseline. HDL, high-density lipoprotein; LDL, low-density lipoprotein; LOCF, last observation carried forward; TG, triglycerides.
Table 4. Treatment-Emergent Adverse Events
durability of the response. Although these results are similar
to results reported for bariatric surgery, the study provides noinformation regarding the relative efficacy and safety com-
pared with the surgical procedures. Finally, the study results
provide no information about the biologic mechanisms that
contribute to the improvement in glycemic control.
The study was not randomized and did not include a
control group. Therefore, it is possible that behavioral changes
in the subjects may have contributed to some of the benefits
observed. The pharmacologic treatment of type 2 diabetes
was not specified or standardized in this study, and changes
in antidiabetes drug regimens may have influenced the re-
sults. Finally, the study was small, and device-related early
explantation of the DJBL was required in 27% of patients.
The results of this study provide clear evidence that the
DJBL can improve glycemic status and cardiometabolic fac-
tors in obese subjects with type 2 diabetes and that it therefore
may represent a nonsurgical and reversible alternative to
bariatric surgery and an effective adjunct to pharmacotherapy
GI Dynamics paid for professional medical writing
and editorial assistance that was provided by Edward
Weselcouch, Ph.D., of PharmaWrite (Princeton, NJ). The au-
thors participated fully in the planning and drafting of this
manuscript and are fully responsible for its content. GI
Dynamics reviewed the final draft of this manuscript to en-
sure the accuracy of the data reported from this company-sponsored clinical trial. Finally, the authors would like to thank
Dr. Lee Kaplan for his discussions regarding the manuscript.
The mechanism responsible for the improvement in type 2
diabetes in this and previous studies is not well understood.
No competing financial interests exist.
However, the rapid improvement in plasma glucose and in-sulin levels suggests that the reduction in body weight was
not solely responsible. This rapid metabolic response has beenobserved in many studies of gastric bypass surgery, sug-
1. Selassie M, Sinha AC: The epidemiology and aetiology of
gesting that rearrangement of GI anatomy plays a role.9,10,17
obesity: a global challenge. Best Pract Res Clin Anaesthesiol
Hickey et al.18 suggested that dysregulated neuroendocrine
signaling between the proximal intestine and pancreas might
2. Nguyen NT, Nguyen XM, Lane J, Wang P: Relationship
participate in the insulin resistance of type 2 diabetes and that
between obesity and diabetes in a US adult population:
bypassing a portion of the foregut may interrupt this abnor-
findings from the National Health and Nutrition Examina-tion Survey, 1999–2006. Obes Surg 2011;21:351–355.
mality. Incretins, like glucagon-like peptide-1 and glucose-
3. Rato Q: Diabetes mellitus: a global health problem. Rev Port
dependent insulinotropic peptide, have been implicated in
this response,19 as has a yet-to-be-identified counter-
4. Shaw JE, Sicree RA, Zimmet PZ: Global estimates of the
prevalence of diabetes for 2010 and 2030. Diabetes Res Clin
The results of this study leave several questions un-
answered. The first is how long does the antidiabetes response
5. Schmidt MI, Duncan BB, Hoffmann JF, Moura L, Malta DC,
last after removal of the device? The results from 11 subjects
Carvalho RM: Prevalence of diabetes and hypertension
indicated that the HbA1c response continued for up to 6
based on self-reported morbidity survey, Brazil, 2006. Rev
months after device removal. It is tempting to speculate that
Saude Publica 2009;43(Suppl 2):74–82.
the stability of the response is an indication of a ‘‘resetting’’ of
6. Malerbi DA, Franco LJ: Multicenter study of the prevalence
glucose homeostasis, but no data from this study support this
of diabetes mellitus and impaired glucose tolerance in the
concept. Clearly, the weight loss may have contributed to the
urban Brazilian population aged 30–69 yr. The Brazilian
DUODENAL–JEJUNAL BYPASS LINER AND DIABETES
Cooperative Group on the Study of Diabetes Prevalence.
bypass liner for the treatment of type 2 diabetes. Diabetes
7. Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR,
15. Rodriguez-Grunert L, Galvao Neto MP, Alamo M, Ramos
Sherwin R, Zinman B: Medical management of hyperglycemia
AC, Baez PB, Tarnoff M: First human experience with en-
in type 2 diabetes: a consensus algorithm for the initiation and
doscopically delivered and retrieved duodenal-jejunal by-
adjustment of therapy: a consensus statement of the American
pass sleeve. Surg Obes Relat Dis 2008;4:55–59.
Diabetes Association and the European Association for the
16. Tarnoff M, Rodriguez L, Escalona A, Ramos A, Neto M,
Study of Diabetes. Diabetes Care 2009;32:193–203.
Alamo M, Reyes E, Pimentel F, Ibanez L: Open label, pro-
8. Turner RC, Cull CA, Frighi V, Holman RR: Glycemic control
spective, randomized controlled trial of an endoscopic
with diet, sulfonylurea, metformin, or insulin in patients
duodenal-jejunal bypass sleeve versus low calorie diet for
with type 2 diabetes mellitus: progressive requirement for
pre-operative weight loss in bariatric surgery. Surg Endosc
multiple therapies (UKPDS 49). UK Prospective Diabetes
Study (UKPDS) Group. JAMA 1999;281:2005–2012.
17. Hussain A, Mahmood H, El-Hasani S: Can Roux-en-Y gas-
9. Greenway SE, Greenway FL 3rd, Klein S: Effects of obesity
tric bypass provide a lifelong solution for diabetes mellitus?
surgery on non-insulin-dependent diabetes mellitus. Arch
18. Hickey MS, Pories WJ, MacDonald KG Jr, Cory KA, Dohm
10. Rubino F, Gagner M: Potential of surgery for curing type 2
GL, Swanson MS, Israel RG, Barakat HA, Considine RV,
diabetes mellitus. Ann Surg 2002;236:554–559.
Caro JF, Houmard JA: A new paradigm for type 2 diabetes
11. Rubino F: Is type 2 diabetes an operable intestinal disease? A
mellitus: could it be a disease of the foregut? Ann Surg
provocative yet reasonable hypothesis. Diabetes Care
1998;227:637–643; discussion 643–634.
19. Bose M, Olivan B, Teixeira J, Pi-Sunyer FX, Laferrere B: Do
12. Gersin KS, Rothstein RI, Rosenthal RJ, Stefanidis D, Deal SE,
incretins play a role in the remission of type 2 diabetes after
Kuwada TS, Laycock W, Adrales G, Vassiliou M, Szomstein
gastric bypass surgery: what are the evidence? Obes Surg
S, Heller S, Joyce AM, Heiss F, Nepomnayshy D: Open-label,
sham-controlled trial of an endoscopic duodenojejunal by-pass liner for preoperative weight loss in bariatric surgerycandidates. Gastrointest Endosc 2010;71:976–982.
13. Schouten R, Rijs CS, Bouvy ND, Hameeteman W, Koek GH,
Janssen IM, Greve JW: A multicenter, randomized efficacy
study of the EndoBarrier Gastrointestinal Liner for presurgical
weight loss prior to bariatric surgery. Ann Surg 2010;251:236–
14. Rodriguez L, Reyes E, Fagalde P, Oltra MS, Saba J, Aylwin
CG, Prieto C, Ramos A, Galvao M, Gersin KS, Sorli C: Pilotclinical study of an endoscopic, removable duodenal-jejunal
Fig. 1.1 Plaques of viruses. (a) Plaques of a bacteriophage on a lawn of Escherichia coli . (b) Local lesions on a leaf of Nicotiana caused by tobacco mosaic virus. (c) Plaques of influenza virus on a monolayer culture of chick embryo fibroblast cells. Fig. 1.2 A one-step growth curve of bacteriophage λ following infection of susceptible bacteria ( Escherichia coli ). During the eclipse
NANO KOREA 2013_Poster Presentation List • Set-up : July 10(Wed.) - July 12(Fri.) 08:00-09:00 • Presentation : July 10 (Wed.) 10:45-12:00 • Tear-down : July 10(Wed.) - July 11(Thu.) 17:00-18:00 July 11 (Thu.) 09:45-11:00 July 12(Fri.) 15:00-16:00 July 12 (Fri.) 09:00-10:15 Examination Abstract No. Date & Time Presenter’s Name Affiliation Poster A
 demonstrate improvement in glycemia, often within days of
disease or other GI disease, pancreatitis, symptomatic coro-
surgery and before significant weight loss.9,10 The mechanism
nary artery disease or pulmonary dysfunction, known gall-
responsible for this improvement is not fully understood;
stones, severe coagulopathy, upper GI bleeding conditions
however, the surgical rearrangement of the anatomy of the
(e.g., esophageal or gastric varices, congenital or acquired
gastrointestinal (GI) tract changes the location where partially
intestinal telangiectasia), congenital or acquired anomalies of
digested nutrients first contact the intestine, suggesting that
the GI tract (e.g., atresias or stenoses), inability to discontinue
correction of dysfunctional homeostatic mechanisms may
nonsteroidal anti-inflammatory drugs during the study, pre-
contribute to the glycemic improvement.11
vious GI surgery that could interfere with placement of the
A nonsurgical method of altering the location of the initial
device, or family or patient history of a known diagnosis or
contact of partially digested nutrients with the intestine is by
symptoms of systemic lupus erythematosus, scleroderma, or
use of the duodenal–jejunal bypass liner (DJBL).12,13 The DJBL
other autoimmune connective tissue disorder.
demonstrate improvement in glycemia, often within days of
disease or other GI disease, pancreatitis, symptomatic coro-
surgery and before significant weight loss.9,10 The mechanism
nary artery disease or pulmonary dysfunction, known gall-
responsible for this improvement is not fully understood;
stones, severe coagulopathy, upper GI bleeding conditions
however, the surgical rearrangement of the anatomy of the
(e.g., esophageal or gastric varices, congenital or acquired
gastrointestinal (GI) tract changes the location where partially
intestinal telangiectasia), congenital or acquired anomalies of
digested nutrients first contact the intestine, suggesting that
the GI tract (e.g., atresias or stenoses), inability to discontinue
correction of dysfunctional homeostatic mechanisms may
nonsteroidal anti-inflammatory drugs during the study, pre-
contribute to the glycemic improvement.11
vious GI surgery that could interfere with placement of the
A nonsurgical method of altering the location of the initial
device, or family or patient history of a known diagnosis or
contact of partially digested nutrients with the intestine is by
symptoms of systemic lupus erythematosus, scleroderma, or
use of the duodenal–jejunal bypass liner (DJBL).12,13 The DJBL
other autoimmune connective tissue disorder.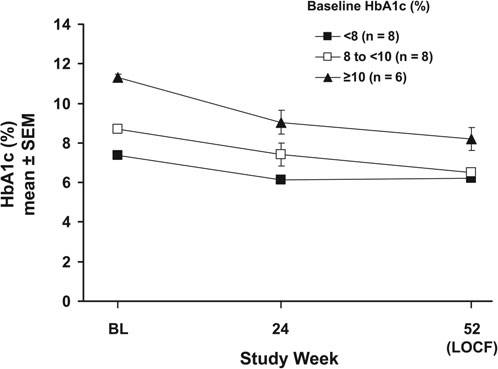
 Data are mean – SEM values (number of patients).
Data are mean – SEM values (number of patients).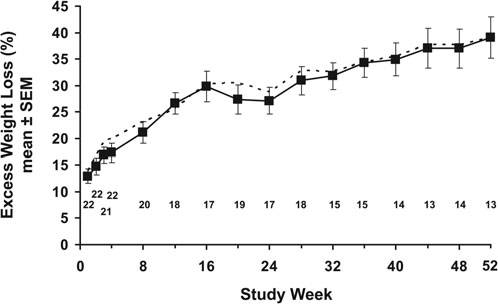 DUODENAL–JEJUNAL BYPASS LINER AND DIABETES
Other clinical studies provide anecdotal observations of the
effect of the DJBL on type 2 diabetes. In the initial 12-weekstudy of the DJBL, four of the 12 obese subjects had type 2diabetes;15 the authors reported that ‘‘all 4 diabetic patientshad normal FPG levels without hypoglycemic medication forthe entire 12 weeks. Of those 4 patients, 3 had decreased he-moglobin A1c of 0.5% by week 12.’’ A second study enrolled40 obese subjects who were candidates for Roux-en-Y gastricbypass and randomly assigned them to either DJBL (n = 26, 25implanted) or low-calorie diet alone (n = 14) with the objectiveof weight loss before surgery.16 Three subjects with type 2diabetes were included in the DJBL group, and one was in-cluded in the diet group. After 12 weeks, two of the three DJBLsubjects demonstrated decreases in HbA1c, and the third,who had a baseline HbA1c of 5.5%, was able to discontinue
Percentage excess weight loss by visit. The number
of subjects represented by each point is shown above the x-
diabetes medications within 1 week of implantation. A similar
axis. The dotted line reflects the loss of excess body weight in
12-week study randomly assigned obese subjects to either
the completer population during the study.
DUODENAL–JEJUNAL BYPASS LINER AND DIABETES
Other clinical studies provide anecdotal observations of the
effect of the DJBL on type 2 diabetes. In the initial 12-weekstudy of the DJBL, four of the 12 obese subjects had type 2diabetes;15 the authors reported that ‘‘all 4 diabetic patientshad normal FPG levels without hypoglycemic medication forthe entire 12 weeks. Of those 4 patients, 3 had decreased he-moglobin A1c of 0.5% by week 12.’’ A second study enrolled40 obese subjects who were candidates for Roux-en-Y gastricbypass and randomly assigned them to either DJBL (n = 26, 25implanted) or low-calorie diet alone (n = 14) with the objectiveof weight loss before surgery.16 Three subjects with type 2diabetes were included in the DJBL group, and one was in-cluded in the diet group. After 12 weeks, two of the three DJBLsubjects demonstrated decreases in HbA1c, and the third,who had a baseline HbA1c of 5.5%, was able to discontinue
Percentage excess weight loss by visit. The number
of subjects represented by each point is shown above the x-
diabetes medications within 1 week of implantation. A similar
axis. The dotted line reflects the loss of excess body weight in
12-week study randomly assigned obese subjects to either
the completer population during the study.