La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Peakmedical.bg
Endovascular Treatment for Iliac Vein Compression Syndrome: a Comparison between the Presence and Absence of Secondary Thrombosis Objective: To evaluate the value of early identification and endovascular treat-
ment of iliac vein compression syndrome (IVCS), with or without deep vein throm-
Materials and Methods: Three groups of patients, IVCS without DVT (group 1,
n = 39), IVCS with fresh thrombosis (group 2, n = 52) and IVCS with non-fresh
thrombosis (group 3, n = 34) were detected by Doppler ultrasonography, magnetic
resonance venography, computed tomography or venography. The fresh venous
thrombosis were treated by aspiration and thrombectomy, whereas the iliac veincompression per se were treated with a self-expandable stent. In cases with freshthrombus, the inferior vena cava filter was inserted before the thrombosis suction,mechanical thrombus ablation, percutaneous transluminal angioplasty, stenting ortranscatheter thrombolysis.
Results: Stenting was performed in 111 patients (38 of 39 group 1 patients and
73 of 86 group 2 or 3 patients). The stenting was tried in one of group 1 and inthree of group 2 or 3 patients only to fail. The initial patency rates were 95%(group 1), 89% (group 2) and 65% (group 3), respectively and were significantlydifferent (p = 0.001). Further, the six month patency rates were 93% (group 1),
Index terms :
83% (group 2) and 50% (group 3), respectively, and were similarly significantly
different (p = 0.001). Both the initial and six month patency rates in the IVCS
patients (without thrombosis or with fresh thrombosis), were significantly greater
than the patency rates of IVCS patients with non-fresh thrombosis. Conclusion: From the cases examined, the study suggests that endovascular
treatment of IVCS, with or without thrombosis, is effective. Korean J Radiol 2009;10:135-143 Received April 30, 2008; accepted after revision July 28, 2008.
liac vein compression syndrome (IVCS) is a clinical syndrome which
All authors: Department of Interventional
causes lower extremity swelling, pain, varicosities and other symptoms
(Affiliated to Nanjing Medical University)
resulting from pelvic and lower extremity venous flow obstruction
caused by the compression of the iliac vein by the overlying iliac artery. McMurrich
Address reprint requests to : Jian-Ping Gu, MD, Department of
first discovered that the left leg swelling is caused by the left iliac vein compression in
1908. In 1956, May and Thurner described, for the first time, the anatomical features
Hospital Affiliated to Nanjing MedicalUniversity, No. 68 Chang Le Road,
of this disease which was then named the May-Thurner syndrome (1, 2). In 1965,
Cockett and Thomas reported the pathology and clinical features of this syndrome and
named it the IVCS. Since then, many people have called this syndrome the Cockett
syndrome. IVCS is not only the main cause of dysfunction in the deep venous valveand varicosities, but also the main cause of iliofemoral vein thrombosis and animportant factor contributing to the higher number of deep-vein thrombosis (DVT)cases in the left extremity (3). The surgical treatment of IVCS has been progressingover the last 40 years (4, 5). For instance, researchers have put the Fogarty balloon
Lou et al.
embolectomy method into practice in subsequent thrombo-
and 60 were of the mixed type (involving the entire lower
sis cases. Furthermore, over the last 20 years, the rapid
development of vascular imaging and intravascular
Stenosis of the iliac vein was observed in 43 cases,
interventional therapy enabled the improvement of
whereas iliofemoral vein occlusion, which included
diagnosis and microinvasive treatment of the IVCS and
common iliac vein occlusion (33 cases) and occlusion of the
secondary thrombosis (6, 7). We present our retrospective
common and external iliac vein (49 cases), was observed in
data from 125 patients to evaluate and compare the effects
82 cases (65.6%). Contrast stasis and emptying delay was
of the endovascular treatment of IVCS, with or without
observed in 122 cases (97.6%) by venography. Moreover,
124 cases (99.2%) had collateral circulation. MATERIALS AND METHODS Interventional Treatment
We treated 39 IVCS patients without DVT as follows: we
Patient Selection
accessed the femoral via local anesthesia and the
One hundred twenty-five cases with IVCS (50 males, 75
subsequent insertion of a F4-F5 sheath. Next, we passed a
females, age range 18-75 yrs, mean 52.5 yrs), with or
H1 catheter (Cordis Corporation, Miami, FL), and guide
without DVT, were enrolled in this study. The exclusion
wire (Terumo Corporation, Tokyo, Japan) through the
criteria included some other causes of DVT such as
stenosis lesion and advanced them up to the inferior vena
malignancy, recent limb trauma, recent surgery (except for
cava. In addition, we exchanged the H1 catheter with a
great saphenous vein stripping) and estrogen therapy.
multi-sidehole catheter (Cook, Bloomington, IN) followed
IVCS is a condition defined by a greater than 50% stenosis
by performing a venography of the iliac vein and inferior
or occlusion of the common iliac vein, accompanied with
vena cava to assess the location and severity of the iliac
significant venous collateral vessels. We did not routinely
vein stenosis or occlusion and ensure that the catheter was
measure venous pressure at our institution as we consider
positioned in the real lumen. A F6-F7 sheath was
these measurements of lesser value for patients in the
exchanged in an 8-12 mm diameter balloon catheter (C.R.
supine position. Contrast stasis and the predominant collat-
Bard, Murray Hill, NJ) was inflated for 20-30 seconds at
eral vein indicated that the hemodynamic significance of
the usual 6-10 ATM, to treat the iliac vein stenosis or
iliac vein stenosis or obstruction. The duration of patient
occlusion. For patients with more than 30% residual
symptoms, including leg swelling, pain and varicose veins,
stenosis, a 10-16 mm diameter self-expandable stent
ranged from one day to two months. The patient
(Luminexx, C.R. Bard, Murray Hill, NJ) should be placed
demographic data are itemized in Table 1.
for patients with 3-4 mm of the cephalad end of the stent
Iliac vein compression syndrome without DVT was
placed into the inferior vena cava. We performed post-
detected in 39 patients by means of venous duplex
stenting dilatation for patients with intra-stent stenosis.
ultrasonography (n = 9), magnetic resonance venography
Of the 125 cases of IVCS, 86 employed an alternative
(n = 7), computed tomography (n = 19) or venography (n =
strategy according to their course, features and position of
4), and confirmed by a femoral venogram. In total, we
the DVT as well as the angiograms of the femoral popliteal
diagnosed 12 patients before stripping the great saphenous
veins. The definition of fresh thrombus consisted of the
vein or endovascular closure, whereas nine cases were
intraluminal-filling defect and double track sign in a
diagnosed by a venography performed due to the aggrava-
venography. In addition, the aspirated thrombus was soft
tion of leg swelling after the stripping of the greatsaphenous vein. The remaining 18 diagnosed IVCS cases
Table 1. Demographic Data of Patients (n = 125)
presented with isolated unilateral lower extremity edema.
In total, 32 cases occurred on the patient’s left side,
whereas seven cases occurred on the right side (left : right
Iliac vein compression syndrome was confirmed in 86
DVT patients by a venography after the aspiration or
mechanical thrombectomy, in which, 71 cases occurred on
the patient’s left side, whereas 15 cases occurred on the
right side (left : right = 4.7 : 1). Of the 86 diagnosed cases
of DVT, 26 were of the central type (involving the
common iliac, external iliac and common femoral vein)
Endovascular Treatment for Iliac Vein Compression Syndrome
and red, or less than 14 days of symptoms.
According to the DSA road map or ultrasound guidance,
All patients were observed using a blood coagulation
followed by other procedures described above, 11 central
function monitor when practicing anticoagulation and
type DVT cases (> 2 weeks, without fresh thrombosis)
thrombolytic therapy. We injected the patients with low
experienced a punctured popliteal vein. Next, a self-
molecular heparin (Nadroparin, GlaxoSmithKline, Tianjin,
expandable stent was implanted. The distal end of the stent
China) twice a day for 3-5 days (4,100 IU abdominal
subcutaneous injection) as well as Warfarin (1.25-5.00 mg
In the 23 mixed DVT cases (> 2 weeks, without fresh
orally) once per day for 1-6 months. We treated patients
thrombosis), the femoral vein in the normal side or the
implanted with a permanent filter with warfarin for a
right internal jugular vein was accessed for the implanta-
longer time than patients with temporary filters. For
tion of the catheter into to iliofemoral vein, followed by a
patients with fresh thrombus who were undergoing
percutaneous transluminal angioplasty (PTA) in the lesion.
thrombus aspiration or mechanical thrombectomy, we kept
In 13 of the 23 cases, which experienced higher blood flow
a multi-sidehole catheter for 3-5 days of thrombolysis
in femoral or external iliac vein, a self-expandable stent
and/or 5-7 days of antegrade thrombolysis. We adminis-
was implanted. The remaining 10 cases with lower blood
tered a daily urokinase dose of approximately 250,000-
flow in the femoral vein, we only performed a PTA to
1,000,000 units. In addition, the patient took a 75-300 mg
daily dose of Aspirin for 6-12 months. We also monitored
If fresh thrombus was found in central DVT patients (15
for blood coagulation to provide evidence for adjustments
case), a retrievable filter (n = 8) was inserted in patients
with less than 14 days of symptoms or a permanent filter(n = 7) in patients with more than 14 days of symptoms via
Assessment of Effect
the contralateral femoral vein, jugular vein or antecubital
Seventy-eight cases had follow-up data. Each patient was
vein. After accessing the popliteal vein, we advanced the
followed by clinical symptom (edema and pain) at 1, 3, 6
H1 catheter and guide wire through the stenosis lesion, up
and 12 months after discharge and annually thereafter. At
to the inferior vena cava. In addition, we exchanged in a
six months after discharge, we performed a venography.
long sheath or guiding catheter, through which we
The average follow-up period was 10.2±0.3 months
suctioned the thrombosis in the iliac and femoral veins.
(range: 0.5-3.0 yrs). We lost 47 cases to follow-up. Based
When a relatively large quantity of thrombosis was
on the comparison of the symptoms and the venography
present, we performed a mechanical thrombectomy via a
performed prior to and six months after discharge, the
Clot Buster Thrombectomy Device (ev3, Plymouth, MN)
clinical effect was graded into four classes as follows:
or a Straub Rotarex system (SRS, Straub Medical AG,
Excellent: disappearance of edema and pain; blood flow
Switzerland). Next, we performed PTA and self-expand-
completely restored on venography; disappearance of
collateral vein; no contrast stasis; and the vessel wall was
If fresh thrombus was found in the mixed DVT patients
smooth. Good: edema and/or pain; blood flow completely
(37 cases), a retrievable filter (n = 9) was inserted in
restored on venography; no collateral vein remained; no
patients with less than 14 days of symptoms, or a
contrast stasis; and the vessel wall was smooth. Moderate:
permanent filter (n = 28) in patients with more than 14
edema and/or pain; blood flow partially restored (greater
days of symptoms via contralateral femoral vein. We used
than 50% patency rate in stent) on venography; collateral
a C3 catheter (Cordis Corporation, Miami, FL) through the
vessels remained; contrast stasis or the vessel wall was not
filter carrier sheath to find the mouth of the affected
smooth. Poor: no improvement of symptoms; no recovery
common iliac vein. Once the catheter attained the external
of blood flow on venography; collateral vein was the main
iliac vein, a H1 catheter was exchanged in and advanced
down to the femoral-popliteal vein, followed by exchang-
Group 1 included IVCS patients without thrombosis,
ing in an 8 Fr long sheath (Arrow International Inc.,
whereas group 2 included IVCS patients with fresh
Reading, PA), through which thrombosis suction was
thrombus and group 3 included IVCS patients with non-
performed in the popliteal, femoral and iliac vein using the
fresh thrombus and the effect of the procedure was
8 Fr guiding catheter (Cordis Corporation, Miami, FL). If
assessed for each group, respectively.
excessive residual thrombus was present, we performed amechanical thrombectomy (such as Clot Buster thrombec-
Definition
tomy device or SRS). Next, we performed a PTA and self-
We defined a technical success as the restoration of
expandable stenting for the residual stenosis found in the
continuous inline flow with the abolition of collaterals
Lou et al.
through the femoral and iliac vein segment into the inferior
(97.4%) had stenting in the iliac vein stenosis (n = 20) and
vena cava. We defined an effective case as a complete or a
occlusion (n = 18) (Fig. 1), either at pre-stent balloon
greater than 50% patency rate for the stenting, and
dilatation (n = 21) or post-stent dilatation (n = 6). In one
included patients classified as excellent, good and
case, the catheter and wire failed to pass the lesion, which
moderate. Patency was defined as the inline flow through
rendered PTA and stenting impossible. The clinical evalua-
the implanted stent segment, into the inferior vena cava,
tions before discharge were classified as: “Excellent” - 21
without contrast stasis and emptying delay, and including
(53.8%), “Good” - 16 (41.0%), “Moderate” - one (2.6%),
patients classified as “excellent” and “good”.
and “Poor” - one (2.6%). Overall, the effective rate was
We performed all statistical calculations using the SPSS
97% (38 of 39 cases), and the patency rate was 95% (37
software package, version 13.0 (SPSS Software Inc,
of 39 cases). In 27 of 39 cases (69.2%), patients were kept
Chicago, IL). We used the 2 test to determine the presence
for obtaining follow-up data. The assessment of the effect
of a statistical difference. For the three groups, we used a
at six months after discharge was as follows: 16 (59.3%)
p-value of less than 0.05 as a threshold for statistical signif-
patients were “Excellent”; nine (33.3%) patients were
icance, and a p-value of less than 0.05 to indicate a statisti-
“Good”; one (3.7%) patient was “moderate” and 1 (3.7%)
cal difference between the two groups.
patient was “poor”. The effective rate was 96% (26 of 27cases) and the patency rate was 93% (25 of 27 cases).
Among the 86 IVCS cases with iliofemoral vein
thrombosis, we performed a thrombosis aspiration or
The overall technical success rate of the treatment was
mechanical thrombectomy in 83 cases (96.5%). Further,
97% (121 of 125 cases). Moreover, the balloon diameter
we performed PTA (n = 67) and stenting (n = 73) in cases
ranged from 8 to 12 mm, with a length ranging from 20 to
of stenosis or occlusion of the iliac vein (Fig. 2), both at
40 mm. The stent diameter ranged from 10 to 16 mm, with
pre- and post-stent dilatation (post-stent performed in one
patient). The catheter and wire failed to pass the occlusion
Among the 39 IVCS cases belonging to group 1, 38
in three cases. This rendered the mechanical thrombec-
Table 2. Effective Rate and Patency Rate Comparison at Discharge (n = 125)
Note.─ Group 1 = iliac vein compression syndrome without thrombosis, group 2 = iliac vein compression syndrome with fresh thrombosis, group 3 = iliac vein compression syndrome with non-fresh thrombosis. No significant difference in patency rates were observed between group 1 and group 2 ( 2 = 0.483,p = 0.487). Conversely, significant difference was observed for patency rate between group 1 and group 3 ( 2 = 10,664, p = 0.001) and between group 2and group 3 ( 2 = 7,010, p = 0.008). Table 3. Effective Rate and Patency Rate Comparison at Six Months Follow-up (n = 78)
Note.─ Group 1 = iliac vein compression syndrome without thrombosis, group 2 = iliac vein compression syndrome with fresh thrombosis, group 3 = iliac vein compression syndrome with non-fresh thrombosis. No significant difference was observed for patency rates between group 1 and group 2 ( 2 = 0,501,p = 0.479). Conversely, significant difference was observed for patency rates between group 1 and group 3 ( 2 = 11,282, p = 0.001) and between group 2and group 3 ( 2 = 6,235, p = 0.013). Endovascular Treatment for Iliac Vein Compression Syndrome
tomy, PTA and stenting impossible, and consequently,
condition, five (22.7%) were in “good” condition; seven
thrombus aspiration only was performed for these three
(31.8%) were in “moderate” condition and four (18.2%)
patients. Twelve of the 17 retrievable filters were retrieved
were in “poor” condition. The effective rate was 82% and
within 10 days of the procedure, whereas the other five
the patency rate was 50%. A detailed assessment is
filters were kept inside because the thrombus lot was
The initial effective rate between the three groups
Of the clinical evaluations of patients belonging to group
revealed no significant difference (p = 0.573). However,
2 (n = 52) performed before discharge, 20 (38.5%) were in
the difference in the initial patency rates between groups
“excellent” condition, 26 (50.0%) were in “good”
were found to be statistically significant (p = 0.001).
condition, five (9.6%) were in “moderate” condition, and
Moreover, the initial patency rates of group 1 (94.9% vs.
one (1.9%) patient was in “poor” condition. The effective
64.7%, p = 0.001) or group 2 (88.5% vs. 64.7%, p =
rate was 98% and the patency rate was 89%. Moreover,
0.008) was greater than the patency rate recorded in group
29 of the 52 (55.8%) patients belonging to group 2 were
3. No significant difference was found for the initial
followed-up. At six months after being discharged, nine
patency rate between group 1 and group 2 (94.9% vs.
(31.0%) patients were in “excellent” condition, 15
88.5%, p = 0.487). Consistently, the results from the six
(51.7%) were in “good” condition, four (13.8%) were in
month follow-up period were similar, with no significant
“moderate” condition and one (3.4%) patient was in
difference in the effective rate between the three groups (p
“poor” condition. The effective rate was 97% and the
= 0.093). Further, a more favorable patency was observed
patency rate was 83%. The clinical evaluation of the
in group 1 (92.6% vs. 50.0%, p = 0.001) and group 2
patients belonging to group 3 (n = 34) before discharge
(82.8% vs. 50.0%, p = 0.013).
found that eight (23.5%) patients were in “excellent”, 14
No complications (i.e. bleeding and hematoma, stent
(41.2%) were in “good” condition, 10 (29.4%) were in
migration, acute thrombosis) occurred during the stenting
“moderate” condition and two (5.9%) were in “poor”
procedure. Moreover, no cases of pulmonary embolism
condition. The effective rate was 94% and the patency rate
(PE) were recorded for all 125 patients (in hospital) and
was 65%. Of the 34 patients belonging to group 3, 22
the 78 patients from the procedure to the 6-month follow-
(64.7%) possessed follow-up data. The six month follow-
up period. We observed one case of inferior vena cava
up indicated that six (27.3%) patients were in “excellent”
obstruction from a patient with an inferior vena cava filter
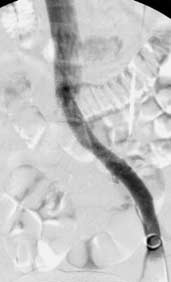
Fig. 1. Treatment of iliac vein compres- sion syndrome without deep vein thrombosis. A. Venography showing compressed left common iliac vein (black arrow) and contralateral venous drainage via pelvic venous collaterals (white arrow). B. Venography after stenting showing widely patent left common iliac vein. Lou et al.
6-month post-treatment angiogram results). However, we
Of the 12 patients with a confirmed IVCS during a
restored the inferior vena cava blood flow following
preoperative examination for the stripping or endovascular
aspiration and a mechanical thrombectomy. In two IVCS
closure of the great saphenous vein symptoms were
patients with recurrent DVT present (3 and 6 months after
relieved in four cases within 3-6 months. The other eight
discharge follow-up evaluation showing the in-stent
cases experienced no remarkable improvement. We
obstruction), blood flow was successfully restored in one
performed five laser and radiofrequency closures in the
case by PTA and not in the other due to the inability to
great saphenous. For the follow-up period, all 12 patients
pass the catheter and wire beyond the obstruction.
were free of the symptoms associated with DVT. Leg
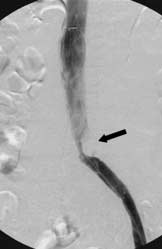
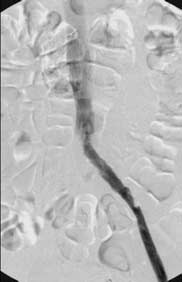
Fig. 2. Treatment of iliac vein compres- sion syndrome with deep vein thrombo- sis. A. Venography showing thrombosis (fresh thrombus and 8 days after onset) and occlusion of left iliofemoral vein as well as contralateral venous drainage via pelvic venous collaterals. B. Venography after thrombectomy and stenting showing patent left femoral vein and in-stent stenosis due to iliac vein compression (black arrow). C. Venography after intra-stent percuta- neous transluminal angioplasty showing widely patent left common iliac vein. D. Venography one year after retrieval of filter showing remaining patent inferior vena cava and left iliofemoral vein. Endovascular Treatment for Iliac Vein Compression Syndrome
swelling was diminished after PTA and stenting in nine
and Neglen (9) proposed that the development is probably
cases in which IVCS was found by venography because of
a slow, progressive condition. Fluid balance in the limb is
aggravation of symptoms after great saphenous vein
on the edge during orthostasis; however, many patients
surgery. The remaining 18 cases with isolated IVCS
remain asymptomatic until the progressive hemodynamic
showed an improvement in symptoms in 16 cases.
deterioration across a certain critical threshold includingsurgery as well as pregnancy and prolonged immobiliza-
DISCUSSION
tion had been mentioned as contributory factors contribut-ing to patients with asymptomatic lesions and should be
Iliac vein compression is a frequent anatomic variant.
educated and followed-up on closely for the early identifi-
The right common iliac artery crosses over the left
cation of acute occlusion. From the accounts above, we
common iliac vein and then reaches the outside of right
emphasize that the evaluation of the iliac vein in the
iliac vein, where it continues to the right external iliac
patients presenting with unilateral lower extremity edema
artery, which is parallel to the right external iliac vein,
and/or varicose veins, especially in the preoperative
behind the left iliac vein there are sacral promontory or the
examination of the great saphenous stripping and early
fifth lumbar vertebra. The causes of IVCS include the
recognition of iliac vein compression, which may prevent a
combination of compression and vibratory pressure in the
right iliac artery on the iliac vein, which results in the
The successful treatment of IVCS would involve a
pinching of the iliac vein between the artery and the pelvic
combination of several interventional techniques to
bone. The two walls of the vein rub against each other,
remove as much of the iliofemoral vein thrombosis as
which lead to irritation of the endothelium. Moreover, this
possible. Thus, deep vein blood flow can be restored and
irritation led to the proliferation of the endothelium,
the course can be shortened. Also, it can prevent or reduce
synechiae or spurs and the formation of a partition in the
the valve dysfunction of the popliteal and calf vein, as well
lumen. Further, it may cause chronic symptoms of left-side
as reduce the incidence of post thrombosis syndrome. A
venous hypertension including edema, leg heaviness, skin
clot Buster thrombectomy device and SRS work well with
discoloration, pain, varicose veins or ulceration. In
the acute thrombus present in iliofemoral vein (10-14).
addition, it may frequently lead to thrombosis when the
SRS is also effective in dealing with subacute iliofemoral
stenosis of the iliac vein is greater than 50%. IVCS and
thrombosis. An endovascular mechanical thrombectomy,
subsequent thrombosis occurs more commonly on the left
combined with guiding catheter suction, can substitute
side. In our study, IVCS occurred 4.6 times more
most of the surgical embolectomy. However, neither the
frequently on the left side than the right side, whereas
Clot Buster thrombectomy device nor the SRS can be used
IVCS with thrombosis occurred 4.7 times more frequently
to deal with DVT bellow popliteal vein, which needs
on the left side than the right, This difference in frequency
embolectomy from posterior tibial vein incision.
suggests that the results are consistent with the published
The use of an inferior vena cava filter to prevent fatal
PEs is still controversial, Decousus et al. (15) published the
It is difficult to find isolated iliac vein compression
only randomized study for vena cava filters in 1998. The
without thrombosis in a clinical setting, but it does not
results indicated that a significant decrease in the incidence
indicate the low incidence of iliac vein compression.
of PE compared with anticoagulation alone (1.1% vs.
Recent imaging reports have demonstrated that at least a
4.8%, p = 0.03) at 8 to 12 days of follow-up. After two
25% compression of the left iliac vein at the arterial
years, this difference was no longer statistically significant
crossover point may be present in 66% of the asympto-
(3.4% vs. 6.3%, p = 0.16). In contrast, vena caval filters
matic patient population (8). This correlates with nearly a
were associated with significantly more recurrent DVT
50% reduction in the total cross-sectional areas of the vein.
than anticoagulation alone (20.8% vs. 11.6%, p = 0.02). If
Previous reports have suggested that this anatomic variant
there are large amounts of fresh thrombus in the
may predispose the formation of deep venous thrombosis.
iliofemoral vein before PTA, an inferior vena cava filter
Virchow’s Triad describes an increased risk of venous
should be inserted to prevent of thrombus shedding, which
thrombosis with stasis, hypercoagulability and vessel
may lead to a fatal PE (16-18). There are many different
intimal injury, the first of which is present with any venous
types of inferior vena cava filters; the retrievable filter may
obstruction disease including IVCS. There is evidence to
be the best choice for acute thrombosis since it can be
suggest that intimal injury may also take place in the form
retrieved after thrombolysis or a thrombectomy to prevent
of a spur when the compression occurs over time. These
will increase the risk for the development of DVT. Raju
Recent reports have shown that stenting of the iliac vein
Lou et al.
obstruction and venous spur is feasible and safe, and may
thrombosis caused by May-Thurner syndrome. J Vasc Interv
improve the long-term outcome of patients after a
3. Bulger CM, Jacobs C, Patel NH. Epidemiology of acute deep
thrombectomy or thrombolysis of left-side acute DVT (19-
vein thrombosis. Tech Vasc Interv Radiol 2004;7:50-54
23). In this series, both the initial and six month patency
4. Juhan C, Miltgen G, Barthe′le′my P, Ayuso D. Treatment of ilio-
rates in IVCS patients, without thrombus or with fresh
femoral venous thromboses with surgical thrombectomy. Bull
thrombus, had significantly greater patency rates than
IVCS patients with non-fresh thrombus. This demonstrates
thrombectomy for iliofemoral vein thrombosis-10-year results
that the early recognition and management of iliac vein
of a prospective randomized study. Eur J Vasc Endovasc Surg
compression would achieve a more favorable outcome. In
addition, we mentioned that some patients did not experi-
6. Grossman C, McPherson S. Safety and efficacy of catheter-
ence complete symptomatic relief, even though the patient
directed thrombolysis for iliofemoral venous thrombosis. AJR
achieved complete patency for the iliofemoral vein. We
7. Mewissen MW, Seabrook GR, Meissner MH, Cynamon J,
believe that this may be attributed to an increase in venous
Labropoulos N, Haughton SH. Caterter-directed thrombolysis
reflux after iliofemoral stenting (24, 25). Delis et al. (24)
for lower extremity deep venous thrombosis: report of a
reported successful patency results after stenting, despite
national multicenter registry. Radiology 1999;211:39-49
the deterioration of reflux and improved venous claudica-
8. Kibbe MR, Ujiki M, Goodwin AL, Eskandari M, Yao J,
tion associated with successful stent recanalization in the
Matsumura J. Iliac vein compression in an asymptomatic patientpopulation. J Vasc Surg 2004;39:937-943
limbs, which normalizes venous outflow, enhances the calf
9. Raju S, Neglen P. High prevalence of nonthrombotic iliac vein
muscle pump function and leads to a significant improve-
lesions in chronic venous disease: a permissive role in
ment in clinical outcome. We suggest that the enhanced
pathogenicity. J Vasc Surg 2006;44:136-144
postoperative stocking is pivotal in preventing disease
10. Sharafuddin MJ, Gu X, Han YM, Urness M, Gunther R,
progression and outcome improvement.
Amplatz K. Injury potential to venous valves from the Amplatzthrombectomy device. J Vasc Interv Radiol 1999;10:64-69
The limitations of this study involve its retrospective
11. Delomez M, Beregi JP, Willoteaux S, Bauchart JJ, Janne d’Othe′e
nature, the limited number of isolated iliac vein compres-
B, Asseman P, et al. Mechanical thrombectomy in patients with
sion patients evaluated, and the relatively short follow-up
deep venous thrombosis. Cardiovasc Intervent Radiol
period. These lower the relevance among iliac vein
compression, incidence of deep venous thrombosis due to
12. Vedantham S, Vesely TM, Parti N, Darcy M, Hovsepian DM,
Picus D. Lower extremity venous thrombolysis with adjunctive
iliac vein compression, and the success of early treatment
mechanical thrombectomy. J Vasc Interv Radiol 2002;13:1001-
in relation to the longer-term outcome. Thus, we need to
perform a prospective control study with a large sample
13. Frisoli JK, Sze D. Mechanical thrombectomy for the treatment
of lower extremity deep vein thrombosis. Tech Vasc Interv
In conclusion, the data obtained from the evaluated
14. Sharafuddin MJ, Sun S, Hoballah JJ, Youness FM, Sharp WJ,
patients suggest that endovascular treatment for IVCS,
Roh BS. Endovascular management of venous thrombotic and
with or without thrombosis, is safe and effective. This
occlusive disease of the lower extremities. J Vasc Interv Radiol
study shows a superior patency rate in IVCS patients
without thrombosis and with fresh thrombosis when
15. Decousus H, Leizorovicz A, Parent F, Page Y, Tardy B, Girard
compared to IVCS patients with non-fresh thrombosis. We
P, et al. A clinical trial of vena caval filters in the prevention ofpulmonary embolism in patients with proximal deep-vein
suggest the reconstruction of the evaluation for the
thrombosis. N Engl J Med 1998;338:409-415
occurrence of iliac vein compression in patients with unilat-
16. Yamagami T, Kato T, Iida S, Hirota T, Nishimura T. Gunther
eral lower extremity edema and preoperative examina-
tulip inferior vena cava filter placement for deep venous
tions indicating the presence of varicose veins. Early
thrombosis of the lower extremity. Cardiovasc Intervent Radiol
recognition and endovascular treatment of iliac vein
17. Rosenthal D, Wellons ED, Lai KM, Bikk A, Henderson VJ.
compression could prevent a DVT and an improvement in
Retrievable inferior vena cava filters: initial clinical results. Ann
18. Kalva SP, Wicky S, Waltman AC, Athanasoulis CA. TrapEase
References
vena cava filter: experience in 751 patients. J Endovasc Ther
1. O’Sullivan GJ, Semba CP, Bittner CA, Kee ST, Razavi MK, Sze
DY, et al. Endovascular management of iliac vein compression
19. Kim JY, Choi D, Guk Ko Y, Park S, Jang Y, Lee do Y.
(May-Thurner) syndrome. J Vasc Interv Radiol 2000;11:823-
Percutaneous treatment of deep vein thrombosis in May-
Thurner syndrome. Cardiovasc Intervent Radiol 2006;4:571-
2. Patel NH, Stookey KR, Ketcham DB, Cragg AH. Endovascular
management of acute extensive iliofemoral deep venous
20. Kwak HS, Han YM, Lee YS, Jin GY, Chung GH. Stents in
Endovascular Treatment for Iliac Vein Compression Syndrome
common iliac vein obstruction with acute ipsilateral deep
Subintimal angioplasty in the treatment of chronic lower limb
venous thrombosis: early and late results. J Vasc Interv Radiol
ischemia. Korean J Radiol 2006;7:131-138
24. Delis KT, Bountouroglou D, Mansfield AO. Venous claudication
21. Blum A, Roche E. Endovascular management of acute deep vein
in iliofemoral thrombosis: long-term effects on venous hemody-
thrombosis. Am J Med 2005;118:S31-S36
namics, clinical status, and quality of life. Ann Surg
22. Liang HL, Pan HB, Lin YH, Chen CY, Chung HM, Wu TH, et
al. Metallic stent placement in hemodialysis graft patients after
25. Neglen P, Thrasher TL, Raju S. Venous outflow obstruction: an
insufficient balloon dilation. Korean J Radiol 2006;7:118-124
underestimated contributor to chronic venous disease. J Vasc
23. Cho SK, Do YS, Shin SW, Park KB, Kim DI, Kim YW, et al.
Ortho-McNeil Neurologics Voluntarily Recalls Two Lots of TOPAMAX ® Titusville, N.J., April 14, 2011 – Ortho-McNeil Neurologics Division of Ortho-McNeil-Janssen Pharmaceuticals, Inc., today announced it is voluntarily recalling two lots of TOPAMAX® (topiramate) 100mg Tablets. These two lots were shipped between 10/19/2010 and 12/28/2010 and distributed in the U.S. and Puerto Rico. Whi
INFORMATION LEAFLET: TRANSURETHRAL RESECTION OF THE PROSTATE (TURP) TURP or transurethral resection of the prostate is an operation that people undergo to relieve the symptoms caused by an enlarged prostate. The symptom complex is known as lower urinary tract symptoms and typical y comprises of people having nocturia (getting up often at night), frequency (passing water too frequently),
 Lou et al.
Lou et al.







 Lou et al.
Lou et al.
 Endovascular Treatment for Iliac Vein Compression Syndrome
Endovascular Treatment for Iliac Vein Compression Syndrome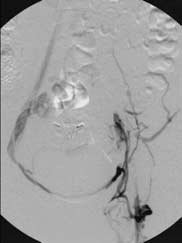
 Lou et al.
Lou et al.