La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Painmanagementservices.net
Name: ____________________________________ Age: _________ Today’s Date: _________________________ Name of the Doctor you are seeing today: _____________________________________________________________ Primary Care Doctor’s Name: _______________________________________________________________________
Phone number or FAX: __________________________________________ The name of the doctor who referred you to us: ________________________________________________________
Phone number or FAX: __________________________________________ Have you ever been seen at another pain clinic? If so,
___________________________________________________________
___________________________________________________________
Vital Signs:
About how much do you weigh? ___________ pounds.
Allergies to Medicines: ____________________________ ____________________________ ____________________________ ____________________________ ____________________________ ____________________________ Medications ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ ___________________ Are you on any BLOOD THINNERS? If YES, please name: __________________________________________ History of Present Illness 1. When did the pain first begin? ______Year ______ Months _____ Weeks ago. 2. How did the pain come on at first? Gradually? Suddenly? Explosively? 3. Where on your body does the pain start? _____________________________________________________________ 4. Where does the pain seem to travel? ________________________________________________________________ 5. What caused the pain? ____________________________________________________________________________ 6. Which words best describe your pain? (check all of the following that applies):
7. Which of the following best describes the quality of the pain? (check the one that applies)
8. Which words best describe the timing of the pain? (circle all that applies):
9. As time goes on, is this pain getting:
10. Which of the following symptoms is this pain associated with (check all that applies):
11. Which of the following make the pain worse? (check all that applies):
12. Which factors seem to relieve the pain? (check all that applies):
13. Which of the following previous treatments have you tried? (check all that applies):
14. Have you ever had any previous Physical Therapy? If so, When:
_____________________________________________________________________________________
____________________________________________________________________________________
15. Which of the following types of medications have you used to relieve your pain? (check all that pertains):
narcotics (like percocet, ultram, vicodin, codeine)
tricyclic antidepressants (like elavil, imipramine)
muscle relaxants (like valium, flexeril, baclofen)
NSAID (like motrin, celebrex, vioxx, naprosyn)
anticonvulsants (like neurontin, tegretol)
16. Have you had RECENT imaging studies such as MRI, CT or x-rays? I so, When:
________________________________________________________________________
________________________________________________________________________
Location of your pain: Please use the figures below to shade in the area where you have pain. If your pain moves around, put an “X” where it starts and draw an arrow to where it spreads. Past Medical History: 17. In your past, have you ever had any of the following health problems? (check all that apply or write in). Cardiovascular:
Other _________________________________________________________________________
Other _________________________________________________________________________
Other _________________________________________________________________________
Other: ________________________________________________________________________
Other _________________________________________________________________________
Other _________________________________________________________________________
Other _________________________________________________________________________
Other ________________________________________________________________________.
Other _________________________________________________________________________
Other: ________________________________________________________________________
Other _________________________________________________________________________
Other _________________________________________________________________________
Past Surgical History: 18. Have you had any surgeries in the past? Please list (even if they seem unrelated to your pain problem). ____________________________ Family History: 19. How is the general health of your family? Please write in any serious health problems or diseases. Also, please indicate if any of your family has ever had similar pain problems as you.
Brother_________________________________
Father _________________________________
Social History:Tell us a little about yourself.
Marital status: Married. Divorced. Widowed. Single. How many children have you had? ___________ children. Who do you live with at home? _________________________________________________________________ How far did you get in your education? ___________________ level. Describe your occupation status:
Employed. What work do you do? __________________________________________________ Retired. What occupation did you have? ______________________________________________ Unemployed. Disabled
Habits? Please check or write in all that applies: Tobacco
No alcohol. Social consumption of alcohol
____beverages/day containing alcohol Review of Systems: 20. Are you experiencing any of the following symptoms with regularity that is different than what you listed before? If so, please circle. General: Respiratory: Neurologic: Gastrointestinal: Cardiac: Psychiatric: Endocrine: Hematological: Oswestery Questionnaire
Could you please complete this questionnaire. It is designed to give us information as to how your pain has affected your ability to manage in everyday life. Please answer every section. Mark one box only in each section that most closely describes you today. Section 1: Pain intensity Section 6: Standing
0. I can stand as long as I want without extra pain
1. I can stand as long as I want but it gives me extra pain
2. Pain prevents me from standing more than 1 hour
3. The pain is fairly severe at the moment
3. Pain prevents me from standing more than a half of an
5. The pain is the worst imaginable at the moment
4. Pain prevents me from standing more than 10minutes
5. Pain prevents me from standing at all
Section 2: Personal care (washing, dressing etc.)
0. I can look after myself normally without causing extra
Section 7: Sleeping
1. I can look after myself normally but it is very painful
1. My sleep is occasionally disturbed by pain
2. It is painful to look after myself and I am slow and
2. Because of pain, I have less than 6 hours of sleep
3. Because of pain, I have less than 4 hours of sleep
3. I need some help but manage most of my personal care
4. Because of pain, I have less than 2 hours of sleep
4. I need help everyday in most aspects of my personal care
5. Pain prevents me from sleeping at all
5. I do not get dressed, wash with difficulty and stay in bed
Section 8: Sex life Section 3: Lifting
0. My sex life is normal and causes me no extra pain
0. I can lift heavy weights without extra pain
1. My sex life is normal but causes some extra pain
1. I can lift heavy weights but it gives extra pain
2. My sex life is nearly normal but is very painful
2. Pain prevents me from lifting heavy weights off the floor
3. My sex life is severely restricted by pain
but I can manage if they are conveniently positioned; for
4. My sex life is nearly absent because of pain
3. Pain prevents me from lifting heavy objects but I can
manage light to medium weights if they are conveniently
Section 9: Social life
0. My social life is normal and causes me no extra pain
1. My social life is normal but increases the degree of
5. I cannot lift or carry anything at all
2. Pain has no significant effect on my social life apart
Section 4: Walking
from limiting my more energetic interests., e.g. sports
0. Pain does not prevent me walking any distance
1. Pain prevents me walking more than 1 mile
3. Pain has restricted my social life and I do not go out
2. Pain prevents me walking more than a quarter mile
3. Pain prevents me walking more than 100 yards
4. Pain has restricted social life to my house
4. I can only walk using a stick or crutches
5. I have no social life because of pain
5. I am in bed most of the time and have to crawl to the
Section 10: Traveling Section 5: Sitting
1. I can travel anywhere but it gives extra pain
0. I can sit in any chair as long as I like
2. Pain is bad but I manage journeys over 2 hours.
1. I can sit in my favorite chair as long as I like
3. Pain restricts me to journeys of less than 1 hour
2. Pain prevents me from sitting more than 1 hour
4. Pain restricts me to short necessary journeys less than
3. Pain prevents me from sitting more than a half of an hour
4. Pain prevents me from sitting more than 10minutes
5. Pain prevents me from traveling except to receive
Oswestrey Score: __________________
Curriculum Vitae del Dr. Stefano Lauretti Data di aggionamento: 26 marzo 2008 1. Profilo Dirigente Medico I Livel o Urologia II. Ospedale CTO, Roma Direttore Unità Organizzativa di Andrologia e Day SurgeryResponsabile Protocolli di Ricerca Clinica, UOC Urologia IIConsigliere Società Italiana di Andrologia, Macroregione LAMS Lazio Abruzzo Molise SardegnaMembro Commissione Interdiscipli

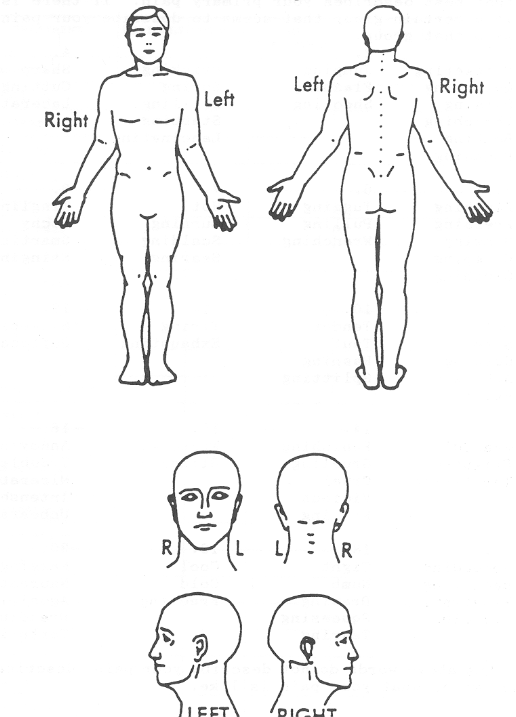 Location of your pain:
Location of your pain: