La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Untitled-
Indian J. Anaesth. 2003; 47 (5) : 367-372
ACUTE RENAL FAILURE Dr. Rebecca Jacob Introduction
reliable indicator of underlying renal function than the
Acute renal failure (ARF) is seen commonly in the
BUN levels. (Values higher than 2 mgdl-1day-1 may be
perioperative period and in the ICU.1 It is associated with
a high morbidity and mortality (oliguric 50-80% and non
Creatinine Clearance. Normal creatinine clearance
oliguric 10-40%).2 It is therefore imperative to either
is 120 mlmin-1. A crude estimation of the creatinine
prevent its occurrence or recognize its presence and treat
clearance may be obtained by the following formula.
it as soon and as efficiently as possible. Definition of renal dysfunction and it’s diagnosis1,2
CrCl (ml/min) = ———————————— 72 x serum Cr (mg/dl)
Urinary output
Traditionally oliguria is defined as a urine output of
This equation is simply the ratio of the expected
less than 0.5 mlkg-1hr-1 or 400 mlday-1. Anuria is defined
amount of muscle breakdown (taking age and weight into
as less than 50 ml per day (check that the Foley’s catheter
account) to the breakdown product present in the serum
is not blocked). However, a reduction in the urine output
multiplied by a ‘fudge factor’ of 72. Women being smaller
need not necessarily mean renal failure. It may just be an
the resulting value is multiplied by 0.85 for females.
external sign of an underlying process such as hypotension
However in acute renal failure with rapidly failing kidneys
and hypovolemia which needs correction. Restoration of
this formula may overestimate creatinine clearance and a
blood pressure and blood volume may increase the urine
more accurate estimation is required. This may be done
output showing that the kidney is in perfect condition.
by collecting urine over a period of time, usually 24 hoursbut in the ICU situation even 2 hours has been shown to
Urinalysis. The presence of blood may suggest the
yield accurate results and may be more practical ads well
presence of an embolic phenomenon and a large number
of casts acute tubular necrosis. Also look for protein andmyoglobin. However, ‘dirty’ results on urinalysis are
CrCl (ml/min) = ——————————————————
Blood Urea Nitrogen (BUN) is the breakdown
product of protein and in the presence of acute renal failure
Urine sodium and osmolality. When perfusion of
it typically rises by about 10 -15 mgdl-1day-1. However it
the kidneys is reduced, sodium reabsorption increases
must be remembered that the BUN level varies directly
and excretion decreases and a urine sodium of less than
with protein intake and increases in the presence of
20 meqL-1 results (urine osmolality >400 mosmolkg-1).
gastrointestinal bleeding, sepsis and corticosteroid
This may occur in hypovolemia due to dehydration
administration (and falls in starvation, malnutrition, muscle
or haemorrhage, or from decreased forward flow as is
wasting and liver disease). Thus interpretation of BUN
seen in patients with cardiac failure. Urinary sodium
values must rely more on the change over time rather than
concentrations of less than 10 meqL-1 may be seen in
on absolute values taking into account concomitant
patients with hepatorenal syndrome or very severe hypo
conditions such as those mentioned above as well as other
When there is an acute injury to the kidney, as in
acute tubular necrosis, sodium reabsorption is impaired and
Creatinine is the breakdown product of muscle and
there is an increase in sodium excretion resulting in urinary
its level rises by 1 to 2 mgdl-1day-1 in acute renal failure.
sodium levels of greater than 20 meqL-1 or even greater
Its absolute value and change over time is a much more
than 40 meqL-1 (urine osmolality <400 mosmolkg-1).
Note that the above numbers are meaningless if
diuretics have been given, Occasionally a combination of
Correspond to :
factors like hypovolemia in addition to chronic renal failure
INDIAN JOURNAL OF ANAESTHESIA, OCTOBER 2003
may make the interpretation of urinary sodium levels
Renal or intrarenal renal failure classically falls
difficult. In these cases fractional excretion of sodium
into 3 categories: Tubular failure (including acute tubular
may help determine whether the cause is renal or prerenal.
necrosis), interstitial nephritis and glomerulonephritis and
vasculitis. However, it is probably more helpful to classifyintrarenal failure according to the causes of renal damage
Fe Na = —————————————— x 100
Post renal
This occurs when there is an obstruction to renal
A fractional excretion of sodium of less than 1%
flow anywhere distal to the pelvis. Obstruction is always
occurs in prerenal failure (hypovolemia and cardiac failure)
the most likely diagnosis when there is anuria.
and that of more than 2% in renal failure (e.g. acutetubular necrosis)
For this to occur both ureters, or the urethra should
be obstructed. It is commonly seen in patients with
Abdominal ultrasound can help differentiate chronic
retroperitoneal or pelvic pathology and abdominal
causes (small kidneys hypertension and chronic renal
ultrasound is a good diagnostic tool. Do remember to
failure, normal or large kidneys diabetes and amyloidosis)
check the patency of the Foleys catheter.
and obstructive causes (large dilated pelvis and ureters). Itcan also estimate renal perfusion using Doppler ultrasound. Table - 24 : Causes of oliguria Nuclear scans are useful in case of suspected
Pre renal Post Renal Causes1 (Table 1) Pre renal
Hypoperfusion due to any cause makes the kidney
concentrate urine, decreases the urine output and causes
the BUN and creatinine to rise. The BUN level usually,
but not always, rises out of proportion to the creatinine
level and a ratio of 20:1 is achieved. Therefore prerenal
failure is most often not a failure at all but a normal
response on the part of the kidney to an inadequate
perfusion. Common causes include hypovolemia, congestive
cardiac failure and extreme vasodilation. Treating the
precipitating cause may rapidly and completely reverse the
rise in BUN and creatinine levels. Genuine renal injury
may only occur if there is a superimposed insult like
GlomerulonephritisInterstitial nephritisPolyarteritis
Table - 13 : Investigations to help differentiate pre renal and renal causes of renal failure Perioperative considerations Investigation Pre renal
It is important to understand the pathogenesis ofrenal failure. Though the kidneys receive 25% of the
cardiac output, they only get 10% of the total body oxygenuptake. Renal autoregulation does take care of the GFR
over a wide range of blood pressures and glomerular ultra
filtration is a balance between vasodilators andvasoconstrictors. However, of the blood that the kidneys
receive the glomeruli receive 90-95% while the medullaonly receives 5-10%. Oxygen extraction on the other hand
is much greater in the medulla due to active water and salt
reabsorption. Thus the medulla is more prone to hypoxic
Table - 3 : Risk Factors Patient factors Perioperative factors
The occurrence of perioperative renal failure depends
upon the surgery, preoperative and intraoperative
haemodynamics and renal conditions (diabetic patients have
a 10 fold greater risk of renal deterioration in the presence
of hypovolemia). All intravenous and volatile induction
agents affect renal function by decreasing cardiac output
and blood pressure. Extradural block (or high spinal) up
to the level of T4 reduces sympathetic tone to the kidneys,
resulting in a decrease in RBF and GFR. Mechanical
ventilation with positive pressure also decreases renal blood
flow. Major surgery with extensive third space losses can
lead to hypovolemia and renal hypoperfusion.
Thus the progression of renal failure may take one
of three paths as seen in Fig. 1. Exclusion of pre renal
and post renal causes make intrinsic renal failure the most
likely cause. This is often associated with an increased
Physical examination and preparation for surgery Fig - 14 :Pathogenesis of Acute Renal Failure
Check the adequacy of hydration, cardiac output
and blood pressure. Also look at the daily intake and
Pre renal Azotemia Intrinsic Acute Post renal Renal Failure Azotemia
Use a large bore cannula for intravenous fluid
resuscitation and administer oxygen. Essential preliminary
monitoring includes an electrocardiogram, noninvasive
blood pressure monitoring and pulse oximetry. Invasivearterial monitoring and central venous pressure monitoring
should be then considered. Echocardiography and
pulmonary artery wedge pressure monitoring are helpful,
Shift to the ICU for monitoring and preoperative
Prevention of further deterioration of renal functionand maintenance of adequate renal output (1-2 ml per kg– non oliguric renal failure) 2
Preoperative rehydration is essential especially in
those patients who are significantly dehydrated e.g. thosewith large bowel obstruction or sepsis. Aim to measure
and maintain the CVP at 10-15 cms. H O. The response
to a fluid bolus (250-500 ml of normal saline) over 10–15
minutes may help to differentiate between hypovolemia
per se and acute tubular necrosis, while more invasivemonitoring is got ready (CVP, Pulmonary artery
Risk factors for developing renal failure
catheterization and echocardiography may be required.)
successful prevention of perioperative ARF depends on
Some authors suggest that we aim to maintain a mean
the identification of patients who are at risk for developing
arterial blood pressure of at least 50 mmHg, which is the
lower limit for renal autoregulation.1 But most authorssuggest maintaining a higher blood pressure – a mean
INDIAN JOURNAL OF ANAESTHESIA, OCTOBER 2003
of >70 mmHg in normal patients and >85 mmHg in
Reduce the administration of acid (commonly
hypertensive patients2 using ionotropes if necessary.
administered in the form of 0.9% sodium chloridesolution which has a pH of 5), potassium, magnesium
If intra abdominal pressure is raised more than
and phosphates in maintenance IV and enteral feeds.
20 mmHg (normal 0-17 mmHg) anuria can resultfrom direct compression on the renal pelves.5 This isseen in 30% of emergency laparotomies and is verycommon after massive intra abdominal bleeding suchas leaking abdominal aortic aneurysms, intestinaldistension, paralytic ileus and ascitis. Improvementin renal function only occurs after decompression. The probable mechanisms for a decrease in cardiacoutput and thus the GFR in these cases are as follows:reduced venous return, compression of the renal veinwith reflex renal artery vasoconstriction, elevationof renal tubular pressure with a decrease in thefiltration gradient and an increase in rennin,aldosterone and ADH production.
Intra abdominal pressure may be measured via the
bladder. Instill 50 ml saline into the bladder via a Foley’scatheter, clamp it off and measure the manometric pressureof the fluid within the bladder via a needle inserted intothe catheter lumen
Raised intra abdominal pressure may also give rise
to a false high CVP leading to under filling of the patient.
- On first recognition of deteriorating renal function
immediately eliminate or appropriately reduce the dose ofnephrotoxic drugs like gentamicin and vancomycin (measurelevels where possible) and change amphotericin tofluconazole if possible.
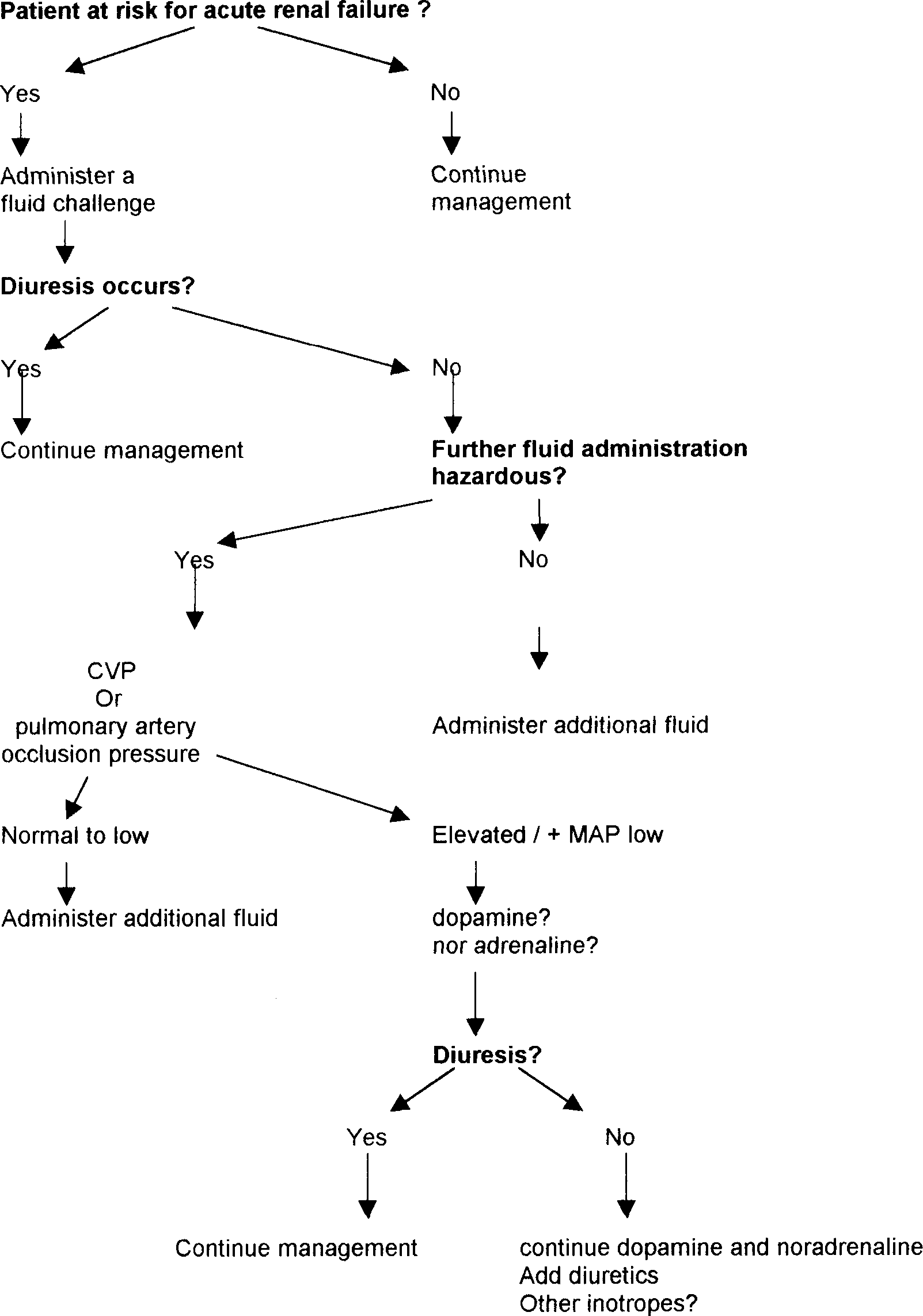
Fig. 2 : Treatment algorithm for management of acute oliguria during the
Table - 45 : Nephrotoxins and nephrotoxic drugs, which could precipitate renal failure .
Start enteral feeds as early as possible and maximize
Nephrotoxic drugs Nephrotoxins
enteral nutrition, as there is now evidence thatoutcomes are better in patients on enteral rather than
Other management issues Use of diuretics Assoc. with crystal production
The rationale for their use rests on the assumption
that they decrease oxygen consumption in the tubular cells
by inhibiting trans cellular sodium transport and thus
prevents ischemic cell injury. In addition, loop diuretics
may vasodilate cortical vessels and improve oxygenation.
If the blood pressure is normal and hypovolemia is
Finally augmentation of tubular blood flow may reduce
not an issue drastically cut down on the IV fluid
intratubular obstruction and back leak of filtrate thus rapidly
therapy, thereby preventing a fluid overload.
accelerating resolution of ARF.6 However, in patients withestablished ARF several studies have shown no benefit of
The use of dopamine and diuretics remains
It is believed that the outcome of non-oliguric renal
failure is better than oliguric renal failure. However, in a
recent retrospective survey of critically ill patients with
stroke volume. However, adrenaline has detrimental effects
ARF diuretic use was associated with an increased risk of
on splanchnic blood flow and causes transient decreases in
death and non recovery of renal function.9 The authors
suggested that the adverse outcome was due to either direct
Dobutaminemay be used to improve cardiac output.
deleterious effects of diuretics or indirect effects owing to
However, it causes peripheral vasodilatation and is usually
a delay in the recognition of the severity of ARF and
institution of dialysis support.9,10 Other authors believe that
The use of Fenoldopam is also controversial
diuretics may also prove harmful as frusemide can causeinterstitial nephritis and hearing loss.1
Calcium channel blockers.5 During ischaemia,
calcium channels open resulting in vasospasm. It is believed
Therefore, diuretics should be used cautiously in
that calcium channel blockers exert direct vascular effect
critically ill patients and no patient should be given
with preservation of renal autoregulation and enhanced
furosemide unless they are adequately filled and the
recovery of RBF, GFR and natriuresis among other effects.
systemic arterial pressure is adequate as an already damaged
However it must be remembered that calcium channel
kidney may be profoundly injured by a relatively mild
blockers in high doses may compromise the haemodynamic
decrease in perfusion pressure.6 Frusemide has been given
in a bolus of 20 – 40mg. In patients with established renal
Specific pharmacological treatments6 have been
insufficiency (raised serum creatinine) and sustained oliguria
used in cases of acute renal failure associated with sepsis.
this treatment should be withdrawn.6 However, in
Examples of these include Anti-TNF-± therapy, inhibition
responders 250 mg may be given as an infusion over an
of platelet-activating factor, inhibition of nitric oxide
hour2 as infusions are more effective and less toxic than
synthase, endothelin antagonism, inhibition of arachidonic
bolus doses.10 Mannitol 0.5 to 1gkg-1 may also be given2
acid metabolism, natriuretic peptides, inhibition of leukocyte
Use of Dopamine
adhesion, inhibition of coagulation and growth factors –
Low dose dopamine (1 to 3 ¼gkg-1 per min)
the details of whose use is beyond the scope of this article
increases diuresis and natriuresis in healthy experimental
Emergency management of raised serum potassium2
animals and humans. These effects are not seen uniformly
Treatment should be initiated if the serum potassium
in the critically ill.11,12,13 However after extensively
is > 6.5 mmol.L or ECG changes are present. Intervention
reviewing the data available the same authors came to the
is important as cardiac compromise may occur.
conclusion that the use of dopamine in renoprotectivedoses should be abandoned as there was no evidence
Table - 5 : Treatment of hyperkalemia.
supporting its effectiveness in preventing ARF and it shouldnot be used as a panacea for oliguria. In addition, dopamine
Treatment Mechanism Duration
can precipitate serious cardiovascular and metabolic
of action of effect of action
complications such as depression of the respiratory
drive, triggering of tachyarrhythmias, causing myocardial
ischemia, accelerating intestinal ischemia, depression
of anterior pituitary hormones and decreased T-cell
Noradrenaline
It markedly improves mean arterial pressure and
glomerular filtration. This is especially seen in high output-
low resistance septic shock. Urine flow reappears with
restoration of systemic haemodynamics and renal function
improves without the use of low dose dopamine or
frusemide. This fact supports the hypothesis that renal
ischaemia observed during hyperdynamic septic shock isnot worsened by nor adrenaline infusion and even suggests
that this drug may effectively optimize renal blood flow
AdrenalineIn patients who fail to respond to fluid
administration and other vasopressor adrenaline can increase
arterial pressure primarily by increasing cardiac index and
INDIAN JOURNAL OF ANAESTHESIA, OCTOBER 2003
Other complications of renal failure include severe
metabolized by the liver the excretion of their active
metabolic acidosis which is dealt with by dialysis
metabolites are by the kidney and thus a reduction in doseis often necessary. Dialysis
Dialysis may be emergent or elective. The
indications for dialysis are volume overload, hyperkalemia,
Acute renal failure is a common and in many cases
severe acidosis, and uremia (with a change in mentation,
it is a preventable and/or eminently treatable problem seen
pericarditis, pleuritis or bleeding). Emergency dialysis is
in the operation theaters and intensive care units and the
rarely required in hospitalized patients .In the ICU set up
physician treating the critically ill patient should be well
BUN and creatinine clearance is assessed daily and dialysis
versed in the diagnosis and management of renal failure.
is usually started when the BUN level exceeds 100 mgdl-1or the creatinine clearance is less than15 mlmin-1. (these
References
figures are arbitrary and vary from center to center).
1. Leibowitz AB, Approach to renal failure.In Apostolakos MJ
and Papadakos PJ(eds.)The Intensive Care ManualTata
There are four contemporary modes of dialysis:
Peritoneal Dialysis (PD, not usually considered in
2. Purday J, Acute renal failure in Allman KG and Wilson IH
the post operative general surgical patient with
Eds. Oxford Handbook of Anaesthesia. Oxford UniversityPress: 2001; 116-118.
abdominal pathology or respiratory compromise).
3. Stoelting RK, Dierdorf SF Eds, Renal diseases IN Anaesthesia
Hemodialysis (HD, difficult to do especially in the
and Co-Existing Diseases, Stoelting & Dierdorf Eds. ,Churchill
hypotensive post operative or septic patient, requiring
Livinstone Elsevier IndiaPubl.4th Ed 2002; 356-360.
4. Nightingale P & Edward DJ Critical Care In Wylie and
Continuous Arterio Venous Hemofiltration (CAVH,
Churchill Davidsons A Practice of Anaesthesia6th Ed. CohenPJ, Healy TEJ Eds. Edward Arnold Publ. London 1995;
relies on an adequate pressure head, has no external
apparatus to control flow or provide warning andrequires the insertion of a wide bore catheter into an
5. Reddy VG. Prevention of Postoperative Acute Renal Failure
– A Review. Journal of Post graduate Medicine, 2002; 48;
artery which may result in bleeding, an aneurysm,
6. De Vries. AS, Prevention and treatment of acute renal failure
It has been largely replaced by Continuous Veno
in sepsis. J Am Soc Nephrol 2003; 14: 792-805.
Venous Hemofiltration CVVH, is a slow method of
7. Brown CB, Ogg CS, Cameron JS: High dose frusemide in
solute and fluid removal, results in a largely
acute renal failure: a controlled trial Clin. Nephrol 1981; 15:
haemodynamically stable milieu and can remove a
large quantity of cytokines which may reduce the
8. Shilliday IR, Quinn KJ, Allison ME: Loop diuretics in the
incidence or progression of multi-organ failure. The
management of acute renal failure: a prospective double blind,
newer machines have improved safety features such
placebo-controlled randomized study. Nephrol Dial Transplant
as an air detector and a pressure monitor. They do
however require one on one nursing and frequent,
9. Mehta RL, Pascual MT, Soroko S, Chertow GM: PICARD
4-6 hourly, potassium assessment. They are capable
Study group: Diuretics, mortality and nonrecovery of renal
of removing upto 10 litres of fluid at one sitting and
function in acute renal failure JAMA 2002; 288: 2547-2553.
is often helpful in weaning from mechanical
10. Martin SJ, Danziger LH: Continuous infusion of loop diuretics
in the critically ill: A review of literature: Critical CareMedicine 1994; 22: 1323-1329. Prescribing common drugs in renal failure1
11. Denton MD, Chertow GM, Brady HR : “Renal dose’’
All medications prescribed for these patients should
dopamine for the treatment of acute renal failure: Scientific
be reviewed and dose adjusted to accommodate the
rationale, experimental studies and clinical trials. Kidney Int
decreasing renal function and the effects of dialysis. Failure
to do this may result in drug toxicity or further damage to
12. Burton CJ, Tomson CR; Can the use of low-dose dopamine
for the treatment of acute renal failure be justified? PostgradMed J 1999; 75: 269-274.
Drugs most commonly used in the ICU, which will
require adjustment, include penicillins, carbipenems,
13. Marik PE Low dose dopamine: a systematic review Int. Care
cephalosporins, vancomycin, aminoglycosides, amphotericin,digoxin, and some muscle relaxants. Anaesthetists should
14. Vincent JL Haemodynamic support in septic shock Int Care
remember that though opioids and benzodiazepines are
DISCHARGE DIAGNOSES: 1. Right upper lobe pneumonia. 2. Right hilar lymph node borderline size at 1.5 cm. 3. Obesity. 4. Hypertension. 5. History of hypothyroidism. 6. Gastroesophageal reflux disease. 7. History of dyslipidemia, died1 controlled. 8. Allergic rhinitis. CONSULTANTS: Pulmonology HOSPITAL COURSE: This is a 66-year-old female who presented to the emergency department with subjective fe
HIV Research Network – Adult Cohort Variable List CY2010 **FINAL** VARIABLE DESCRIPTION FORMAT FIELD GUIDELINES VARIABLE NAME HIV RESEARCH NETWORK CY2010 ADULT VARIABLE LIST PLEASE NOTE: 1. Variables that were new in CY2009 remain highlighted in blue . 2. Variables that are new or have changed in CY2010 are shaded in orange . 3. Variables that are no longer a
 INDIAN JOURNAL OF ANAESTHESIA, OCTOBER 2003
of >70 mmHg in normal patients and >85 mmHg in
Reduce the administration of acid (commonly
hypertensive patients2 using ionotropes if necessary.
INDIAN JOURNAL OF ANAESTHESIA, OCTOBER 2003
of >70 mmHg in normal patients and >85 mmHg in
Reduce the administration of acid (commonly
hypertensive patients2 using ionotropes if necessary.