La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Cd alert
Monthly Newsletter of National Centre for Disease Control, Directorate General of Health Services, Government of India May - July 2009 Vol. 13 : No. 1 SCRUB TYPHUS & OTHER RICKETTSIOSES
it lacks lipopolysaccharide and peptidoglycan
RICKETTSIAL DISEASES
and does not have an outer slime layer. It is
These are the diseases caused by rickettsiae
endowed with a major surface protein (56kDa)
which are small, gram negative bacilli adapted
and some minor surface protein (110, 80, 46,
to obligate intracellular parasitism, and
considerable differences in virulence and
organisms are primarily parasites of arthropods
antigen composition among individual strains
such as lice, fleas, ticks and mites, in which
they are found in the alimentary canal. In
vertebrates, including humans, they infect the
vascular endothelium and reticuloendothelial
GLOBAL SCENARIO
cells. Commonly known rickettsial disease isScrub Typhus.
Geographic distribution of the disease occurswithin an area of about 13 million km2 including-
The family Rickettsiaeceae currently comprises
Afghanistan and Pakistan to the west; Russia
of three genera – Rickettsia, Orientia and
to the north; Korea and Japan to the northeast;
Indonesia, Papua New Guinea, and northern
of the family, Coxiella burnetii, which causes
first observed in Japan where it was found to
trench fever have been excluded because the
be transmitted by mites. The disease was,
former is not primarily arthropod borne and
therefore, called tsutsugamushi (from tsutsuga
the latter is not an obligate intracellular parasite,
being capable of growing in cell-free media,
insect or mite). This is found only in areas
besides being different in genetic properties.
with a suitable climate, plenty of moisture and
Scrub typhus will be dealt in detail.
scrub vegetation. Recently, rickettsioses has
SCRUB TYPHUS
been an emerging disease along the ThaiMyanmar border. There are reports of
CAUSATIVE AGENT
emergence of scrub typhus in Maldive Islandsand Micronesia.
Scrub typhus (Chigger borne typhus,Tsutsugamushi fever) is caused by Orientia
INDIAN SCENARIO
tsutsugamushi. Orientia is a small (0.3 to 0.5by 0.8 to 1.5 µm), gram negative bacterium of
In India, scrub typhus has been reported from
the family Rickettsiaceae. It differs from the
Rajasthan, Jammu & Kashmir and Vellore. In
other members in its genetic make up and in
addition, few cases have been tested positive
the composition of its cell wall structure since
for IgM antibodies for scrub typus from Sikkim,
Darjeeling, Nagaland & Manipur (unpublished
morning, chiggers can be collected from the
data). In a study conducted from July through
body of the sentinel animals. The mites can
be preserved in 70% alcohol till they reach
cases of acute febrile illness of unknown origin,
laboratory for identification. Chigger index
O.tsutsugamushi was identified as causative
(average number of chiggers infesting a single
agent by microimmunofluorescence and PCR.
host) of > 0.69 (critical value) is an indicator
In an entomolgic study in Himachal Pradesh,
for implementation of vector control measures.
vector species Leptotombidium deliense andGahrliepia spp. were recorded. Habitats favorable for disease transmission
Scrub typhus, originally found in scrub jungles,
DISEASE TRANSMISSION
Leptotrombidium deliense. The vector mites
mountain deserts and equatorial rain forests.
inhabit sharply demarcated areas in the soil
Incubation Period
where the microecosystem is favourable (miteislands). Human beings are infected when they
trespass into these mite islands and are bittenby the mite larvae (chiggers). The mite feeds
CLINICAL PICTURE
on the serum of warm blooded animals onlyonce during its cycle of development, and adult
A Papule develops at the site of inoculation.
mites do not feed on man. The microbes are
The papule ulcerates and eventually heals
transmitted transovarially in mites. Scrub
mammals, particularly field mice and rodents.
(>40ºC [104ºF]) with relative bradycardia,
The L.deliense group of vector mites are widely
distributed all over the country coexisting
Approximately one week later, a spotted and
hosts, the chiggers attach in clusters on the
tragus of the ear, the belly and on the thighs.
the trunk and then on the extremities and
The Leptotrombidium mites, on the rat host,
may appear orange or pink. The typical vector
L.deliense is generally found associated with
(30 to 65% of cases), meningoencephalitis
secondary vegetation after clearance of forestareas. This species is generally abundant on
grasses and herbs where bushes are scarce.
Sentinel animals can also be used for collection
of trombiculid mites from the field. These
myocarditis, the mortality rate may reach
animals are generally white laboratory mice or
rats kept in small cages containing food andwater and placed in the field overnight to attract
DIAGNOSIS
chiggers. Chiggers can also be collected fromfield directly on human beings, by walking in
Routine laboratory tests are unlikely to be
the field after wearing stockings. The following
diagnostic for any rickettsial diseases. Common clinical manifestations of the Rickettsial Diseases Scrub Typhus axillary eschar Maculopapular rash on back of a case of scub typhus Laboratory diagnosis
early lymphopenia with late lymphocytosis.
Scrub typhus may be diagnosed in the laboratory
finding. Thrombocytopenia is observed in more
Collection, storage & transportation of specimen
all pertinent information to laboratory whichwill help in better interpretation of the
The collection, transportation and storage of
specimens are extremely vital steps in laboratorydiagnosis and hence, must be undertaken with
Isolation of the organism
As rickettsiae are highly infectious and have
Specimen
caused several serious and fatal infectionsamong laboratory workers, it comes under Risk
Group 3 organisms. Isolation should be done in
laboratories equipped with appropriate safety
provisions preferably Biosafety level-3 labora-tory following strict biosafety precautions.
Rickettsia may be isolated in male guinea pigs
Blood collection in tubes and vials
or mice; yolk sac of chick embryos; vero cellline or MRC 5 cell lines from patients in early
Aseptically collect 4-5 ml of venous blood.
phase of the disease. Egg and animal inocula-
tion methods have been replaced by faster and
centrifuge at 2000 rpm to separate serum.
more sensitive cell cultures. Rickettsiae growwell in 3-5 days on Vero cell and MRC 5 cell
Collect the serum in sterile dry vial.
coverslip cultures and can be identified by im-munofluorescence using group and strain spe-
Fix the cap with adhesive tape, wax or other
sealing material to prevent leakage duringtransport. Serological diagnosis
Diagnosis of the etiology of rickettsial diseases
indelible ink, or a typewritten self adhesive
can be accomplished most easily and rapidly
label to identify the container. The name of
by demonstrating a significant increase in anti-
the patient, identification number and date of
bodies in the serum of the patient during the
collection must be indicated on the label.
course of infection and convalescence. Severalserological tests are currently available for the
Do’s/Don’ts while collecting specimen:
diagnosis of rickettsial diseases like Weil-Felix
Test (WFT), Indirect Immunoflourescence (IIF),Enzyme linked Immunosorbent assay (ELISA)
etc. Although many techniques have been used
successfully for rickettsial sero diagnosis, rela-tively few are used regularly by most laborato-
ries. BSL-3 Lab is not required for performing
laboratory at 2-8ºC (ice box) as soon as
Weil-Felix Test (commonly used test)
Don’t freeze whole blood as haemolysismay interfere with serology test results.
The Weil-Felix test is helpful in establishingpresumptive diagnosis in diseases caused by
In case the delay is inevitable, keep the
members of typhus and spotted fever groups of
specimen at + 4ºC in a refrigerator.
Rickettsiae. The interpretation of Weil-Felix test
Molecular diagnosis – PCR Table 1 : Weil-Felix Test
For PCR, blood sample is collected in tubescontaining EDTA or sodium citrate. However,
blood clot, whole blood or serum can also beused for the detection of O.tsutsugamushi,
R.rickettsii, R. typhi and R.prowazekii organismsby PCR test.
Facilities for laboratory diagnosis of Rickettsial
diseases are available at National Centre forDisease Control, Delhi where samples can be
TREATMENT
Prompt institution of effective antibiotic therapy
against rickettsiae is the single most effectivemeasure for preventing morbidity and mortality
due to rickettsial diseases. Anti rickettsial therapyimproves the outcome of all rickettsioses, with
The sensitivity and specificity of the Weil-Felix
test is reported to be low as compared to the
complicated cases of RMSF, epidemic typhus
specific serological tests for detection of IgM
and scrub typhus where the illness is no longer
antibodies. However, comparative evaluation of
susceptible to intervention. If the illness is severe,
Weil-Felix test and IgM ELISA for diagnosis of
the cardiac, pulmonary, renal, and central
Scrub Typhus carriedout at NCDC, showed that
Weil Felix test is equally sensitive with specific-
additional measures instituted to prevent
Indirect Immunofluorescent antibody (IFA)
Tetracyclines and chloramphenicol remain the
only proven therapy for the rickettsial diseases. Doxycycline in a dose of 100 mg twice daily for
IFA is used as a reference technique; however,
availability and cost are major constraints and
times a day PO for 7-15 days (for children 150
is not available in most of the laboratories.
mg/kg/day for 5 days) is recommended. Enzyme linked Immunosorbent Assay
Tetracyclines may cause discoloration of teeth,
hypoplasia of the enamel, and depression ofskeletal growth in children; the extent of
ELISA techniques, particularly immunoglobulin
discolouration is directly related to the number
M (IgM) capture assays, are probably the most
of courses of tetracycline therapy received.
sensitive tests available for rickettsial diagnosis,
Therefore, tetracycline should not be used for
and the presence of IgM antibodies, indicate
children under 8 years of age and for pregnant
recent infection with rickettsial diseases. In
cases of infecton with O.tsutsugamushi, asignificant IgM antibody titer is observed at the
PREVENTION AND CONTROL
end of the first week, whereas IgG antibodies
The mite vectors of scrub typhus are especially
appear at the end of the second week.
amenable to control because they are often
found in distinct areas (Typhus Island).
infection but not the pubic louse. The licebecome infected by feeding on rickettsiaemic
patients. The rickettsiae multiply in the gut of
the lice and appear in the faeces in 3-5 days.
insecticides, reducing rodent populations,
Lice succumb to the infection within 2-4 weeks,
remaining infective till they die. They can transmit
the infection after about a week of being infected.
Persons who cannot avoid infested terrain
Transmission
should wear protective clothing, impregnatetheir clothing and bedding with a mitecide (e.g.
Lice may be transferred from person to person.
benzyl benzoate) and apply a mite repellent,
Being sensitive to temperature changes in the
host, they leave the febrile patient or the cooling
carcass and parasitise other persons. Lice
defecate while feeding. Infection is transmittedwhen the contaminated louse faces is rubbed
by scratching. Occasionally, infection may also
decreased the incidence of clinical illnesses
be transmitted by aerosols of dried louse faces
through inhalation or through the conjunctiva. Incubation period: 5 - 15 days.
been developed till now, mainly due toserotypic heterogeneity of the organism. Clinical Presentation OTHER RICKETTSIAE INFECTIONS
The disease starts with fever and chills. EPIDEMIC TYPHUS
A characteristic rash appears on the fourthor fifth day, starting on the trunk and spreading
Epidemic typhus (Louseborne typhus, Classical
over the limbs but sparing the face, palms
typhus, Gaol fever) has been one of the great
scourges of mankind, occurring in devastating
epidemics during times of war and famine. The
disease has been reported from all parts of the
world but has been particularly common in
of consciousness in the disease. The case
Russia and Eastern Europe. During 1917-1922,
fatality may reach 40% and increases with
there were some 25 million cases in Russia,
with about three million deaths. In recent times,the main foci have been Eastern Europe, Africa,
In some who recover from the disease, the
South America and Asia. In India, the endemic
rickettsiae may remain latent in the lymphoid
tissues or organs for years. Such latent infectionmay, at times, be reactivated leading to
The causative agent of epidemic typhus is
recrudescent typhus or Brill Zinsser disease.
R.prowazekii, named after von Prowazek.
Brill noticed a mild, sporadic, typhus-like disease
Humans are the only natural vertebrate hosts.
Natural infection in flying squirrels has been
reported from South- eastern USA. The human
R.prowazekii from such cases and proved that
body louse, Pediculus humanus corporis, is the
vector. The head louse may also transmit the
ENDEMIC TY\PHUS
Endemic typhus (Murine typhus) is a milderdisease than epidemic typhus. It is caused byR.typhi which is maintained in nature as a mildinfection of rats, transmitted by the rat flea,Xenopsylla cheopis. The rickettsia multiplies inthe gut of the flea and is shed in its faeces. Theflea is unaffected but remains infectious for therest of its natural span of life. Humans acquirethe disease usually through the bite of infectedfleas, when their saliva or faeces is rubbed in orthrough aerosols of dried faeces. Ingestion of
Eschar of tick bite over the left side of the abdomen
food recently contaminated with infected rat urineor flea faeces may also cause infection. Human
a case of endemic typhus or with a culture of
infection is a dead end. Man to man transmission
R.typhi, they develop fever and a characteristic
does not occur. In India, endemic typhus has
scrotal inflammation. The scrotum becomes
been reported from Pune, Lucknow,
enlarged and the testes cannot be pushed back
Mysore, Kolkata, Golkunda, Karnal, Rewari and Kashmir.
adhesions between the layers of the tunicavaginalis. This is known as the Neil-Mooser or
Clinical presentation
the tunica reaction. The Neil-Mooser reaction is
SPOTTED FEVER GROUP
They are all transmitted by ticks, except R.akari,
headache, fever and rash. This is seen only
which is mite borne. Rickettsiae of this group
possess a common soluble antigen and multiplyin the nucleus as well as in the cytoplasm of
Rash develops in 54% of patients some time
host cells. Many species have been recognized
Nausea, vomiting, diarrhoea and abdominalpain suggest gastrointestinal diseases while
Organism
cough and abnormal chest radiographsuggests pneumonia or bronchitis.
renal insufficiency and respiratory failureare seen in approximately 10% of cases,
R.typhi and R.prowazekii are closely similar but
may be differentiated by biological andimmunological tests. When male guinea pigs
are inoculated intraperiotoneally with blood from
The rickettsiae are transmitted transovarially in
ticks, which therefore act as both vectors and
reservoirs. The infection may be transmitted to
vertebrate hosts by any of the larval stages or
by adult ticks. Ticks are not harmed by the
sanguineus is the most important vector and is
rickettsiae and remain infected for life. The
generally found infesting dogs all over.
transmission to human beings is primarily by
Hyalomma ticks may also transmit the infection.
bite, as the rickettsiae also invade thesalivary glands of the ticks. All rickettsiae of this
The incubation period ranges from 2 to 7 days.
group pass through natural cycles in domestic
In >50% of the patients, a primary lesion with
central necrosis (eschar) appears at the site ofthe tick bite. The lesion is covered with a brownish
ROCKY MOUNTAIN SPOTTED FEVER
black scab (tachy noire) and may ulcerate. Recall of a tick bite cannot always be elicited
Rocky Mountain Spotted Fever (RMSF) is the
from the patient. Regional lymphandenitis is
most serious type of spotted fever and is the
common. The fever lasts for 1 to 2 weeks and
first to have been described. It is prevalent in
many parts of North and South America and is
myalgias and a generalized maculopapular rash
which develops between the third and fifth days
of illness or which may not appear. It disappears
TICK TYPHUS (INDIAN TICK TYPHUS)
at the time of defervescence. Alterations incytokine profiles, hypercoagulability and deep
Tick typhus, in several parts of Europe, Africa
venous thrombosis may occur. In severe cases
and Asia is caused by R.conori, strains of which
– particularly in elderly patients and those with
isolated from the Mediterranean region, Kenya,
diabetes mellitus, alcoholism or heart failure –
South Africa and India are indistinguishable. The
meningoencephalitis with coma and seizures
species is named after Conor, who provided the
and/or disseminated vasculitis of internal organs
first description of the Mediterranean disease.
(e.g. in the heart, lungs, kidneys, liver and
Tick typhus was first observed in India in the
pancreas) are observed. The mortality rate is 1
foothills of the Himalayas. Subsequently, the
to 5% but is higher among patients with severe
disease was reported from many parts of the
.about CD Alert CDAlert is a monthly newsletter of the National Centre for Disease Control (NCDC) (formerly known as NICD), Directorate
General of Health Services, to disseminate information on various aspects of communicable diseases to medical fraternity
and health administrators. The newsletter may be reproduced, in part or whole, for educational purposes.
Dr. Shiv Lal, Dr. R. L. Ichhpujani, Dr. Shashi Khare, Dr. A. K. Harit
Dr. D. Bhattacharya, Dr. Veena Mittal, Dr. Naveen Gupta, Dr. A.C. Dhariwal, Dr. Arti Bahl
Director, National Centre for Disease Control, 22 Shamnath Marg, Delhi 110 054
Tel: 011-23971272, 23971060 Fax : 011-23922677
E-mail: dirnicd@bol.net.in and dirnicd@gmail.com Website: www.nicd.nic.in
Financial assistance by WHO/USAID is duly acknowledged.
Printed at IMAGE, 6, Gandhi Market, New Delhi-110 002, Phones : 23238226, 9811116841
DAVID L. PEARLE, M.D. DAVID L. PEARLE, M.D. PERSONAL INFORMATION HOME ADDRESS: (202) 444-8833 / (877) 303-1461 Facsimile EDUCATION 1964 M.D., Harvard Medical School, Boston, Massachusetts TRAINING/ PROFESSIONAL POSITIONS 1968-1969 Internship in Medicine, New York Hospital Residency in Medicine, New York Hospital Commissioned Officer, Public Health Servic
Substance P and Irritable Bowel: Abstracts 1. World J Gastroenterol. 2009 Nov 7;15(41):5211-7. Effect of electro-acupuncture on substance P, its receptor and corticotropin-releasing hormone in rats with irritable bowel syndrome. Ma XP, Tan LY, Yang Y, Wu HG, Jiang B, Liu HR, Yang L. Shanghai Institute of Acupuncture-Moxibustion and Meridian, Shanghai 200030, China. AIM: To investigate the effect
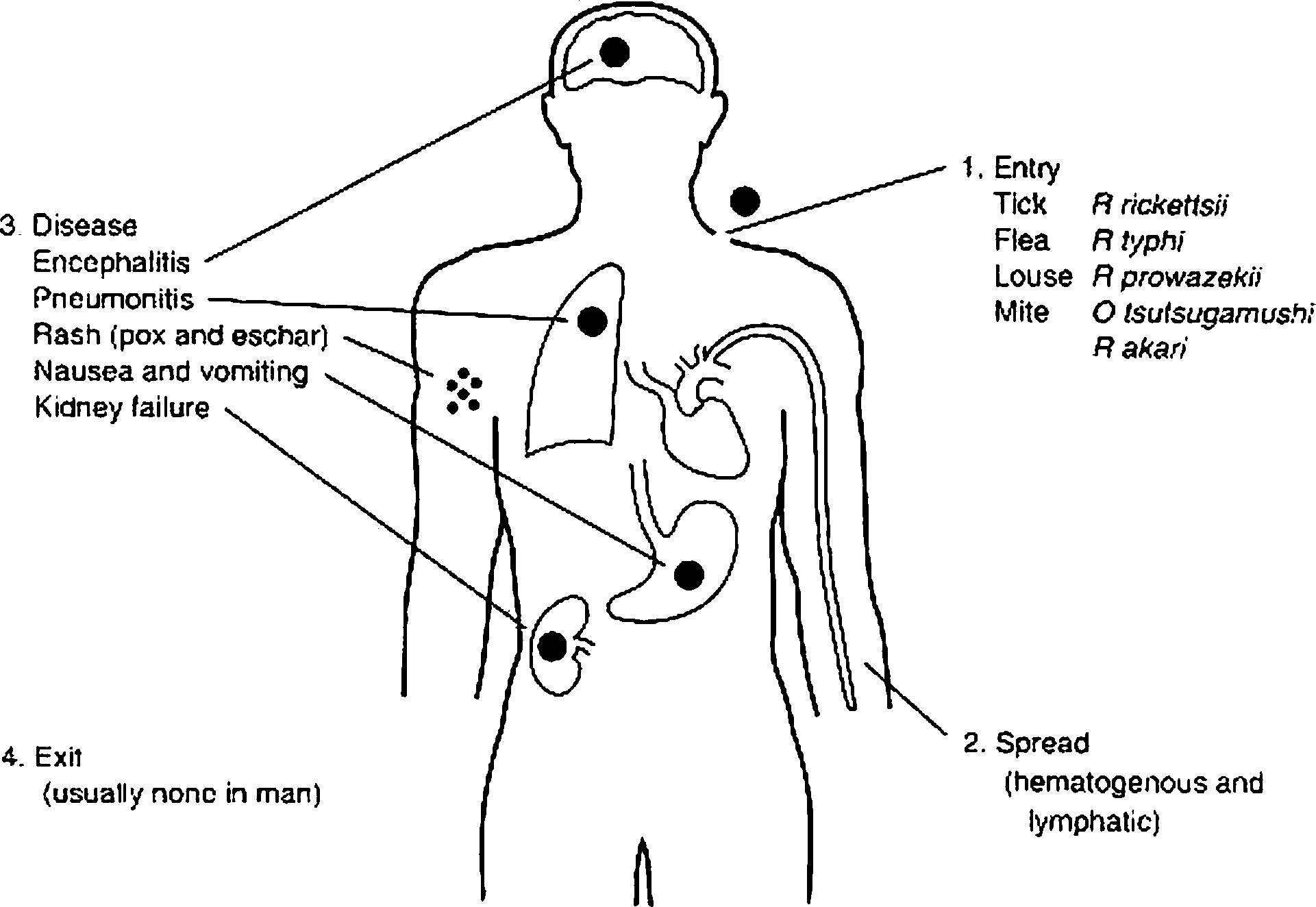

 Common clinical manifestations of the Rickettsial Diseases
Common clinical manifestations of the Rickettsial Diseases ENDEMIC TY\PHUS
ENDEMIC TY\PHUS