La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Favorable effect of very early diseasemodifying antirheumatic drug treatment on radiographic progression in early inflammatory arthritis: data from the tude et suivi des polyarthrites indiffrencies rcentes (study and followup of early undifferentiated polyarthritis)
Vol. 63, No. 7, July 2011, pp 1804–1811
2011, American College of Rheumatology
Disease-Modifying Antirheumatic Drug Treatment on
Radiographic Progression in Early Inflammatory Arthritis
Etude et Suivi des Polyarthrites Indiff´
(Study and Followup of Early Undifferentiated Polyarthritis)
C. Lukas,1 B. Combe,1 P. Ravaud,2 J. Sibilia,3 R. Landew´
Objective. While there is consensus that treat- Undifferentiated Polyarthritis]) cohort were followed ment with disease-modifying antirheumatic drugs up, and radiographic progression after 12 months was (DMARDs) should be started early in patients with assessed. Propensity scores, reflecting the indication to inflammatory arthritis, confirmation that radiographic start a DMARD, were obtained by modeling the start of progression is inhibited with early treatment start is DMARD therapy by disease-specific and demographic scarce. This study was undertaken to compare radio- variables obtained at baseline, using logistic regression graphic progression in patients treated with a DMARD analysis. The influence of very early versus delayed very early in the course of their disease (within 3 months DMARD start on radiographic progression was evalu- of diagnosis) and those who began DMARD treatment ated by generalized linear regression, with and without adjustment for propensity scores. Methods. Patients included in the French obser- Results. Six hundred sixty-one patients were an- vational ESPOIR (´ Etude et Suivi des Polyarthrites alyzed. In an unadjusted analysis, patients starting Indiff´ erenci´ ecentes [Study and Followup of Early DMARD therapy within 3 months of diagnosis did not show a significant difference in radiographic progres-
The ESPOIR cohort study was supported by Merck Sharp and
sion score as compared to those starting DMARD
Dohme (unrestricted grant for the first 5 years), the French Society ofRheumatology, Abbott, and Wyeth. The biologic database was sup-
therapy later (1.2 units versus 1.6 units; P ؍ 0.37).
ported in part by grants from INSERM. Adjustment for the propensity score revealed a statisti-
1C. Lukas, MD, B. Combe, MD, PhD: Lapeyronie Hospital,
cally significant difference in mean progression (0.8
Montpellier, France; 2P. Ravaud, MD, PhD: Bichat Hospital, Paris,France; 3J. Sibilia, MD, PhD: Hautepierre Hospital, Strasbourg,
units versus 1.7 units; P ؍ 0.033). Analysis by propen-
´, MD, PhD: University Hospital Maastricht,
sity score quintile showed a trend suggesting that early
Maastricht, The Netherlands; 5D. van der Heijde, MD, PhD: Leiden
treatment was especially beneficial for patients in the
University Medical Center, Leiden, The Netherlands.
Dr. Ravaud has received consulting fees, speaking fees,
fourth and fifth quintiles (worse prognosis).
and/or honoraria from Schering-Plough, Roche, and Pfizer (less than
Conclusion. Our findings indicate that among
$10,000 each). Dr. Sibilia has received consulting fees, speaking fees,and/or honoraria from Pfizer, Abbott, Roche, Merck, UCB, Schering-
patients with inflammatory arthritis in daily clinical
Plough, and Actelion (less than $10,000 each). Dr. van der Heijde has
practice, early initiation of DMARD therapy reduces
received consulting fees, speaking fees, and/or honoraria from Abbott,
12-month radiographic progression. This strengthens
Amgen, AstraZeneca, Bristol-Myers Squibb, Centocor, Chugai, EliLilly, GlaxoSmithKline, Merck, Novartis, Otsuka, Pfizer, Roche,
the current recommendations for very early initiation of
Sanofi-Aventis, Schering-Plough, UCB, and Wyeth (less than $10,000
specific therapy in patients with early arthritis.
Address correspondence to C. Lukas, MD, Department of
Rheumatology, Lapeyronie Hospital, 371 Avenue du Doyen Gaston
A more intensive treatment approach to the
Giraud, 34295 Montpellier Cedex 5, France. E-mail: c-lukas@chu-
management of early inflammatory arthritis has been
adopted recently, with the general consensus being that
Submitted for publication October 6, 2010; accepted in re-
a disease-modifying antirheumatic drug (DMARD) with
RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
proven structural efficacy should be started as soon as
Undifferentiated Polyarthritis]) cohort, there has been
possible in a patient likely to develop persistent and
variation in the decision to start DMARD therapy and
erosive arthritis (1–4). If classic rheumatoid arthritis
the amount of time since onset at which rheumatologists
(RA) with unfavorable prognostic factors is found at
have first prescribed DMARD therapy. This may theo-
presentation, such a recommendation is obvious, but if a
retically lead to differences in outcome in these patients,
patient is referred very early, a diagnosis and prognostic
which could be clinically meaningful. In the present
profile often cannot be made. While robust and consis-
study we evaluated the impact of the time lag between
tent data have demonstrated both clinical and radio-
arthritis onset (first patient-reported swollen joint) and
graphic superiority of intensive treatment (e.g., combi-
DMARD initiation on 1-year radiographic progression,
nation DMARD therapy), data on impact of the delay
adjusting for the spurious effects of confounding by
between disease onset and DMARD initiation remain
inconclusive. Evidence that earlier treatment initiationresults in better radiographic outcome in patients withRA is still sparse. Clinical trials have thus far mainly
PATIENTS AND METHODS
included patients who fulfill criteria for RA, and these
The ESPOIR cohort. The ESPOIR cohort (14,15) is a
studies show that in early RA, intensive therapy is more
French prospective observational study of adults ages 18–70
efficacious than conventional treatment (5–8). Such
years recruited from multiple regions across France under the
studies do not, however, prove that an early treatment
auspices of the French Society of Rheumatology. To beenrolled in the ESPOIR cohort, patients had to present with
inflammatory arthritis lasting 6 weeks to 6 months and involv-
The data suggesting benefit of early treatment
ing Ͼ2 joints, and the arthritis had to have been diagnosed by
initiation often suffer from confounding by indication:
the referring physician as RA or RA-like (i.e., a high suspicion
physicians base their treatment decisions on the activity
of RA). Patients had to have never undergone treatment with
and thus severity of the disease. Confounding by indica-
a DMARD or steroids before enrollment. Patients were excludedif the referring physician had judged that they had a clearly
tion may lead to a decreased treatment contrast (9,10).
defined inflammatory rheumatic disease other than RA.
In the study by van der Heide et al, for example, earlier
Patients were recruited from general practitioners and
treatment of patients with recently diagnosed RA re-
rheumatologists in 14 regions across France. Data were col-
sulted in improved clinical outcomes after 12 months of
lected by the regional university rheumatology department,
followup whereas no radiographic benefit could be
which was not involved with patient treatment. Patients wereroutinely treated and followed up by private rheumatologists in
observed, probably because of the tendency of the
the geographic area, and in rare cases by general practitioners
investigators to use more intensive additional treatment
with a special interest in rheumatology.
in patients with more severe or persistently active dis-
The results of each test performed for study purposes
ease (11). The ideal experiment to investigate whether
were periodically communicated to the practitioner taking care
an early DMARD start is better than a delayed one is a
of the patient. All patients were followed up by the sameinvestigator once every 6 months during the first 2 years and
pragmatic randomized controlled trial in which patients
once every year thereafter. Data on medical history, socioeco-
are randomized to an arm with an immediate DMARD
nomic and demographic characteristics, and clinical, biologic,
start versus an arm with a delayed DMARD start.
radiographic, and genetic parameters were also collected. One
However, such a study seems unethical in light of current
biologic resource center (Paris-Bichat) was responsible for
centralizing and managing laboratory data collection.
The first patients were enrolled in the ESPOIR cohort
Another concern is that no one can precisely
in December 2002, and recruitment concluded in March 2005.
define how early is early enough. A current view, also
A total of 813 patients were included.
reflected in new treatment recommendations (1), ex-
Radiographic evaluation. Baseline and 1-year radio-
ploits the window-of-opportunity principle for guidance,
graphs of the hands, wrists, and feet were read and assessed
and many believe that 3 months should be the maximum
using the Sharp/van der Heijde score (SHS) (16). The readerswere blinded with regard to patient identity and patient
delay from diagnosis to the initiation of DMARD treat-
characteristics and treatment, but the time order was known, to
ment (12). However, these suggestions are based on
improve sensitivity to change. In order to evaluate the repro-
expert opinion rather than on scientific data, or were
ducibility of the radiographic scoring, radiographs from 30
formulated before methotrexate was commonly used as
patients representing the entire range of status and change
scores observed during the first reading were selected andscored again by the same reader. Intraclass correlation coeffi-
Among patients with early inflammatory arthritis
cients were calculated for status (baseline and 1 year) as well as
for change scores, and the smallest detectable change was
computed using standard methodology (17). Propensity analysis. Principles. It is reasonable to
adjustment for propensity scores; and 2) this gain would be
assume that in convenience cohorts without a fixed treatment
greatest in patients with more severe disease (quintiles with
protocol, such as the ESPOIR cohort, the most important
determinant of an immediate DMARD start is the physician’s
Statistical analysis. Radiographic progression in pa-
opinion of the severity and activity of the disease as well as the
tients who were versus those who were not treated within the
individual prognosis. Severity and activity of the disease may
first 3 months was compared by Mann-Whitney U test. The
confound the relationship between time to DMARD initiation
effect of an early DMARD start on radiographic progression
and radiographic progression (confounding by indication).
was evaluated using a generalized linear model in which
However, the physician’s interpretation of disease severity and
change in 1-year SHS was modeled by treatment start (early
activity is by definition unquantifiable, since it encompasses a
versus late) as well as propensity score.
number of intangible and often unmeasured factors.
Patients were divided into propensity quintiles based
The theory underlying propensity modeling assumes
on their individual propensity scores. By definition, the pro-
that the likelihood of (in this case) a DMARD start, and thus
portion of patients starting DMARD treatment early should
severity of RA in the opinion of the physician, can be
increase per quintile because of the physician’s perception of
approximated by taking into consideration all measured vari-
increasing prognostic severity and disease activity. Subse-
ables at baseline that the physician may or may not implicitly
quently, in an exploratory analysis, radiographic progression
use to base his or her decision to initiate DMARD treatment
was analyzed by quintile according to early DMARD start (yes
(18). By adjusting the relationship between the time to
versus no). Because the limited number of patients per pro-
DMARD start and radiographic progression for individual
pensity quintile likely precludes meaningful statistical compar-
propensity scores, one can partially adjust for confounding by
ison, we refrained from statistically comparing within sub-
groups and report the results as a trend.
For each patient, propensity to start DMARD treat-
ment within the 6 months after the first reported synovitis wasestimated by logistic regression analysis, modeling all available
variables at baseline that, in the opinion of the investigators,
Patient characteristics. Of the 813 patients in the
could have influenced the decision by the treating physician toprescribe the DMARD. DMARD starts taken into account
ESPOIR cohort, 661 had complete data and were in-
were starts with DMARDs of proven efficacy in radiographic
cluded in the present analyses and the remaining 152
progression, i.e., methotrexate, leflunomide, sulfasalazine, and
could not be analyzed. The main reason for exclusion of
tumor necrosis factor (TNF) blockers (or combinations of
patients from analysis was missing radiographs at base-
line (n ϭ 82) and/or at 1 year (n ϭ 141). Baseline
This logistic regression analysis resulted in a propen-
sity score for each patient for starting treatment within 6
characteristics in the group of 661 patients who were
months, which was the time frame within which most patientsprescribed treatment had actually started this treatment. Ac-cording to propensity modeling theory, in patients with similar
Baseline characteristics of the ESPOIR cohort patients
propensities (e.g., in the same quintile), the treatment decision
included in the present analysis and those not included in the present
actually observed at the individual level can be regarded as
independent of disease severity, apart from residual confound-ing. Propensity score. The logistic model used the following
variables to estimate the probability of being treated with
methotrexate, leflunomide, sulfasalazine, and/or anti-TNF
within 6 months after first reported synovitis: center, age,
28-joint Disease Activity Score (DAS28) (19), sex, C-reactive
protein (CRP) level, erosions present (yes/no), comorbidity
present (yes/no), rheumatoid factor (RF) present (yes/no),
anti–cyclic citrullinated peptide 2 (anti–CCP-2) antibodies
present (yes/no), time to first visit to a rheumatologist (Ͻ12
weeks versus Ͼ12 weeks), symmetric arthritis present (yes/no),
involvement of hand joints (yes/no), and involvement of Ͼ3
joint groups (yes/no). Contributory variables were selected by
stepwise forward selection, with P ϭ 0.3 as a limit for includinga potential variable. Baseline was defined as the time point of
* ESPOIR ϭ ´Etude et Suivi des Polyarthrites Indiff´erenci´ees R´ecentes
first reported synovitis. To ascertain this, patients were asked
(Study and Followup of Early Undifferentiated Polyarthritis);
when they had first noticed any swelling in a joint that was
DAS28 ϭ 28-joint Disease Activity Score; SHS ϭ Sharp/van derHeijde score; NA ϭ not available; CRP ϭ C-reactive protein; RF ϭ
(according to the rheumatologist) currently swollen.
rheumatoid factor; anti–CCP-2 ϭ anti–cyclic citrullinated peptide 2;
Hypotheses. The following hypotheses were tested: 1)
ACR ϭ American College of Rheumatology; EULAR ϭ European
an earlier DMARD start—defined as Ͻ3 months from the
League Against Rheumatism; RA ϭ rheumatoid arthritis.
time of arthritis onset (i.e., first swollen joint)—would lead to
less radiographic progression than a later DMARD start after
RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
analyzed and the group of 152 patients who were
Baseline characteristics of the patients who were and those
who were not treated with disease-modifying antirheumatic drugswithin 3 months after the onset of synovitis*
Overall, 527 (79.7%) of the 661 analyzed patients
were started on DMARD therapy within 1 year follow-
ing symptom onset. Methotrexate was the most com-
monly prescribed first DMARD (336 of 527 [64%]),either as monotherapy (307 of 527 [58%]) or in combi-
nation with other DMARDs (hydroxychloroquine, sul-
fasalazine, leflunomide, or TNF-blocking drugs) (29 of
527 [5.5%]). Sulfasalazine was chosen in 66 patients
(13%), and leflunomide in 31 patients (6%). DMARDs
not taken into account in our analysis (mainly hydroxy-
chloroquine monotherapy) were prescribed in 90 pa-
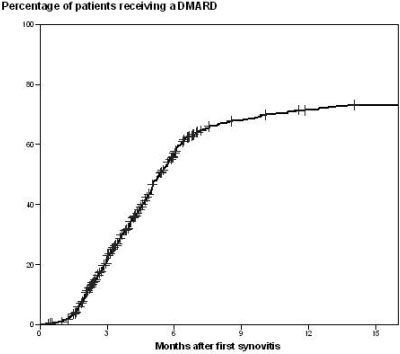
Time to DMARD initiation was very hetero-
geneous, as shown in Figure 1. The proportion ofpatients starting DMARD therapy increased rapidly
treatment among patients starting DMARDs later may
over the first 6 months and leveled off thereafter. Of the
have worked against such a bias. Combination therapy
437 patients who started a DMARD of interest for the
was rarely chosen, which makes it unlikely that differ-
present study, 140 (32%) did so within the first 3 months
ences in the usage of combination therapy had an ef-
after symptom onset, and 205 (47%) within 6 months.
Baseline characteristics of the patients who began treat-
Radiographic progression. The mean Ϯ SD total
ment within 3 months and those who did not begin
SHS at baseline was 5.8 Ϯ 7.8 (range 0–56), with a
treatment within 3 months are reported in Table 2. An
median score of 3 and an interquartile range (IQR) of
imbalance in the type of DMARD treatment used may
1–7.5. The rather high baseline values in some patients
theoretically have had an impact on radiographic pro-
appear surprising, but they are seen more frequently in
gression. However, we did not identify such an imbal-
cohorts of patients with short symptom duration. There
ance. The somewhat higher frequency of TNF blockade
may be several reasons for this: early subclinical jointinflammation that is not recognized by the patient,inaccurate symptom recall, and associated osteoarthritisthat may cause damage resembling erosions and jointspace narrowing in RA. The median radiographic pro-gression at 1 year was 0 (IQR 0–1) and the mean Ϯ SDchange was 1.5 Ϯ 4.3 units (range 0–36). Most patients(72%) did not show any radiographic progression over 1year, but 8% had severe progression (Ն5 units). Theerosion score at baseline was 2.8 Ϯ 4.7 (range 0–40). Change in the erosion score at 1 year was observed in179 patients (27.1%). The mean change in the erosionscore was 1.2 Ϯ 3.5 units (range 0–37). When patientswere grouped according to whether they did or did notbegin DMARD treatment within 3 months of symptomonset, the difference in crude mean radiographic pro-gression was not significant (1.2 Ϯ 3.4 units [range 0–19]in patients starting DMARDs within 3 months and 1.6 Ϯ4.5 units [range 0–37] in patients starting DMARDslater [P ϭ 0.37]).
Intraclass correlation coefficients were Ͼ0.99 for
both radiographic status scores and radiographic change
Figure 1. Percentage of patients starting disease-modifying antirheu-
scores. The smallest detectable change was calculated at
matic drug (DMARD) treatment, by amount of time since the onset ofsynovitis. Figure 2. Percentage of patients starting disease-modifying antirheumatic drug treatment within 3 months of synovitis onset, by propensity score quintile (Q) (higher quintiles reflect greater disease severity). Findings of the propensity analysis. In the final Findings of sensitivity analysis. Additional ana-
logistic model, the investigation center, DAS28 score,
lyses, conducted in order to test the robustness and
time to first rheumatologist visit, RF positivity, involve-
validity of the approach, yielded similar conclusions. The
ment of Ͼ3 joint groups, CRP level, and anti-CCP
conclusions were unchanged when corticosteroid use
antibody positivity remained as contributory factors
was one of the factors included in the propensity model
(listed in decreasing order of contribution). Age, sex,
or when only specific DMARDs were used to define
presence of erosions, comorbidity, symmetric arthritis,
early treatment start. Taking as a minimum the use of at
and involvement of hand joints were not contributory in
least 7.5 mg/day prednisone equivalent for Ͼ3 months in
the model. Subsequently, in order to investigate whether
the first year of disease, the estimated marginal means
the perceived disease activity and severity were influenc-
for the change in radiographic progression score were
ing the crude differences in radiographic progression
similar to those obtained in the original propensity
rate, the propensity score was included as a covariate in
analysis (0.6 SHS units versus 1.8 SHS units in patients
the linear regression analysis. The estimated marginal
who did versus those who did not start DMARD treat-
means were 0.8 units (SEM 0.37) in patients starting
ment within 3 months; P ϭ 0.008). When the propensity
DMARDs within 3 months and 1.7 units (SEM 0.19) in
score was based on the start of only methotrexate and/or
patients starting DMARDs later (P ϭ 0.033), thus
anti-TNF, and not the other DMARDs of interest,
confirming the difference found in the crude analysis.
within 6 months, radiographic progression was also
(SEM is reported here because it is the estimation
lower in patients who had started treatment within 3
provided in a generalized linear model.) Subsequently,
months versus those who had started later (0.9 SHS units
patients were divided into propensity quintiles (Figure
versus 1.6 SHS units), although the difference was not
2). As expected, the proportion of patients starting
statistically significant (P ϭ 0.11). Other approaches to
DMARDs early increased by increasing quintile (in-
determining the propensity score (such as the inclusion
creasing prognostic severity), although only 37.6% of
of the baseline SHS score instead of the presence or
patients in the highest quintile (worst prognosis) started
absence of erosions) also resulted in similar conclusions.
DMARD treatment within 3 months of the onset ofsynovitis. DISCUSSION
Figure 3 shows probability plots of individual
radiographic progression scores by DMARD treatment
The results of this study add to the sparse evi-
start (early versus delayed) in the individual quintiles. In
dence that starting DMARD treatment very early in
the first 3 quintiles (better prognosis) there were no
patients with inflammatory arthritis is favorable with
important differences in radiographic progression be-
regard to radiographic progression. A trend appears to
tween those who started DMARDs within 3 months and
suggest that especially patients with a relatively unfavor-
those who started DMARDs beyond 3 months. A trend
able prognosis benefit from early initiation of treatment.
suggesting benefit of early treatment, especially in pa-
This observation must be interpreted with caution in
tients in the the fourth and fifth quintiles (worse prog-
view of the limited sample size and short followup
period in the present study. However, it is in accordance
RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
with observations stemming from post hoc analyses fromclinical trials comparing intensive and less intensivetreatment, which have shown that patients with the worstprognostic profile especially benefit from intensive treat-ment, while those with relatively mild disease do wellwith less intensive therapy (20,21). Our observationscould be interpreted to suggest that the prognosticprofile is important not only in the choice betweenintensive and less intensive treatment strategies, but alsoin the choice between a very early start and a delayedone. Unfortunately, the propensity score cannot betranslated directly into prognostic variables.
Previous studies have also investigated the impact
of early versus delayed treatment start in patients withearly inflammatory arthritis. Lard et al prospectivelyfollowed up patients referred to an early arthritis clinicwho first received symptomatic treatment and subse-quently received sulfasalazine or hydroxychloroquine(13). They compared radiographic progression in thesepatients versus radiographic progression in patientsstarting DMARD therapy within 15 days after referral,and found that progression was significantly lower in thegroup that received early DMARD treatment. Suchstudies have led to a paradigm shift in the treatmentstrategy for RA, resulting in a recommendation of earlyaggressive treatment rather than a pyramid-like ap-proach in which the initiation of effective DMARDs ispostponed. Important limitations of such studies are thatthe drugs investigated did not include methotrexate (thecurrent anchor drug in early RA), in the majority ofpatients the lag time between symptom onset and treat-ment initiation was beyond current recommendations,and different periods in history—covering differenttreatment paradigms—were compared.
Bukhari et al were the first to report on radio-
graphic progression in an early arthritis cohort in whichthere was no formal treatment protocol (22). Usingpropensity modeling, they convincingly argued that ra-diographic progression at 5 years remained worse inpatients for whom treatment had been delayed by Ͼ6months. In their work, however, the propensity modelwas based on the start of any DMARD, includingcorticosteroids, over the entire 5-year followup periodand the probability of receiving treatment was evaluatedbased on data collected at baseline only, while clinicalstatus does not necessarily remain stable over such along period of time.
The strength of our approach is mainly that the
Figure 3. Probability plots of individual radiographic progression
propensity score we have designed includes a prognostic
scores, by treatment category (disease-modifying antirheumatic drug
profile that is based both on data at first evaluation and
[DMARD] treatment started within 3 months of synovitis onset
on data during the first 6 months of followup. Of note,
[triangles] or not started within 3 months of synovitis onset [dia-monds]) and by propensity score quintile.
the patients were closely monitored since they were
included in the ESPOIR cohort, but treatment decisions
Analysis and interpretation of data. Lukas, Combe, Ravaud, Sibilia,
were left entirely to the discretion of the local physi-
cian(s), and can thus be regarded as a reflection ofcurrent daily clinical practice. ROLE OF THE STUDY SPONSORS
One may expect that the observed differences in
Merck Sharp and Dohme, Abbott, and Wyeth provided an
prognostic factors at first evaluation are an appropriate
unrestricted grant for logistical support of the ESPOIR cohort. Studydesign, data collection, data analysis, and writing of the manuscript
reflection of the heterogeneity rheumatologists encoun-
were done independently, and submission of the manuscript was not
ter among patients referred with early inflammatory
arthritis. The methodologic approach we have usedenables comparisons of therapeutic interventions that
REFERENCES
could not be made under conditions of a clinical trial
1. Combe B, Landewe R, Lukas C, Bolosiu HD, Breedveld F,
that does not incorporate judgments of severity but
Dougados M, et al. EULAR recommendations for the manage-
rather allocates patients irrespective of prognostic pro-
ment of early arthritis: report of a task force of the European
Standing Committee for International Clinical Studies IncludingTherapeutics (ESCISIT). Ann Rheum Dis 2007;66:34–45.
However, the propensity model also has limita-
2. Emery P, Breedveld FC, Dougados M, Kalden JR, Schiff MH,
tions. There are several potentially important variables
Smolen JS. Early referral recommendation for newly diagnosed
that were not assessed but might be be taken into
rheumatoid arthritis: evidence based development of a clinicalguide. Ann Rheum Dis 2002;61:290–7.
account by the rheumatologist during the clinical evalu-
3. Saag KG, Teng GG, Patkar NM, Anuntiyo J, Finney C, Curtis JR, et
ation (intangible factors). Obviously, it is impossible to
al. American College of Rheumatology 2008 recommendations for
adjust for such unmeasured characteristics, and the
the use of nonbiologic and biologic disease-modifying antirheumaticdrugs in rheumatoid arthritis. Arthritis Rheum 2008;59:762–84.
possibility of residual and/or unmeasured confounding
4. Smolen JS, Landewe R, Breedveld FC, Dougados M, Emery P,
Gaujoux-Viala C, et al. EULAR recommendations for the man-
In conclusion, our study showed that patients
agement of rheumatoid arthritis with synthetic and biologicaldisease-modifying antirheumatic drugs. Ann Rheum Dis 2010;69:
with early inflammatory arthritis who began DMARD
treatment early had improved radiographic outcome
5. Boers M, Verhoeven AC, Markusse HM, van de Laar MA,
Westhovens R, van Denderen JC, et al. Randomised comparison
after adjustment for propensity score. These findings
of combined step-down prednisolone, methotrexate and sul-
corroborate the recommendation of very early treat-
phasalazine with sulphasalazine alone in early rheumatoid arthri-
ment initiation in patients with early inflammatory ar-
6. Kuriya B, Arkema EV, Bykerk VP, Keystone EC. Efficacy of
thritis, in order to improve long-term prognosis.
initial methotrexate monotherapy versus combination therapy witha biological agent in early rheumatoid arthritis: a meta-analysis ofclinical and radiographic remission. Ann Rheum Dis 2010;69:
ACKNOWLEDGMENTS
7. Landewe RB, Boers M, Verhoeven AC, Westhovens R, van de
We wish to thank Nathalie Rincheval for expert mon-
Laar MA, Markusse HM, et al. COBRA combination therapy in
itoring and data management, and all of the investigators at the
patients with early rheumatoid arthritis: long-term structural ben-
university hospitals who recruited and followed up patients (F.
efits of a brief intervention. Arthritis Rheum 2002;46:347–56.
Berenbaum [Paris–Saint Antoine], M. C. Boissier [Paris–
8. Mottonen T, Hannonen P, Leirisalo-Repo M, Nissila M, Kauti-
Bobigny], A. Cantagrel [Toulouse], M. Dougados [Paris–
ainen H, Korpela M, et al, FIN-RACo trial group. Comparison ofcombination therapy with single-drug therapy in early rheumatoid
Cochin], P. Fardelonne, P. Boumier [Amiens], B. Fautrel and
arthritis: a randomised trial. Lancet 1999;353:1568–73.
9. Egsmose C, Lund B, Borg G, Pettersson H, Berg E, Brodin U, et
al. Patients with rheumatoid arthritis benefit from early 2nd line
Vittecoq [Rouen], X. Mariette [Paris–Bice
therapy: 5 year followup of a prospective double blind placebo
[Paris–Bichat], A. Saraux [Brest], and T. Schaeverbeke [Bor-
controlled study. J Rheumatol 1995;22:2208–13.
10. Nell VP, Machold KP, Eberl G, Stamm TA, Uffmann M, Smolen
JS. Benefit of very early referral and very early therapy withdisease-modifying anti-rheumatic drugs in patients with early
AUTHOR CONTRIBUTIONS
rheumatoid arthritis. Rheumatology (Oxford) 2004;43:906–14.
11. Van der Heide A, Jacobs JW, Bijlsma JW, Heurkens AH, van
All authors were involved in drafting the article or revising it
Booma-Frankfort C, van der Veen MJ, et al. The effectiveness of
critically for important intellectual content, and all authors approved
early treatment with “second-line” antirheumatic drugs: a random-
the final version to be published. Dr. Lukas had full access to all of the
ized, controlled trial. Ann Intern Med 1996;124:699–707.
data in the study and takes responsibility for the integrity of the data
12. Finckh A, Liang MH, van Herckenrode CM, de Pablo P. Long-
and the accuracy of the data analysis.
term impact of early treatment on radiographic progression in
Study conception and design. Lukas, Combe, Ravaud, Sibilia,
rheumatoid arthritis: a meta-analysis. Arthritis Rheum 2006;55:
Acquisition of data. Combe, Ravaud, Sibilia.
13. Lard LR, Visser H, Speyer I, van der Horst-Bruinsma IE, Zwin-
RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
derman AH, Breedveld FC, et al. Early versus delayed treatment
Keystone E, et al, for the Active-Controlled Study of Patients
in patients with recent-onset rheumatoid arthritis: comparison of
Receiving Infliximab for the Treatment of Rheumatoid Arthritis
two cohorts who received different treatment strategies. Am J
of Early Onset (ASPIRE) study group. Predictors of joint damage
in patients with early rheumatoid arthritis treated with high-dose
14. Combe B. The French early arthritis registry. Clin Exp Rheumatol
methotrexate with or without concomitant infliximab: results from
the ASPIRE trial. Arthritis Rheum 2006;54:702–10.
15. Combe B, Benessiano J, Berenbaum F, Cantagrel A, Daures JP,
21. Verschueren P, Esselens G, Westhovens R. Daily practice effec-
Dougados M, et al. The ESPOIR cohort: a ten-year follow-up of
tiveness of a step-down treatment in comparison with a tight
early arthritis in France. Methodology and baseline characteristics
step-up for early rheumatoid arthritis. Rheumatology (Oxford)
of the 813 included patients. Joint Bone Spine 2007;74;440–5.
16. Van der Heijde D. How to read radiographs according to the
22. Bukhari MA, Wiles NJ, Lunt M, Harrison BJ, Scott DG, Symmons
Sharp/van der Heijde method. J Rheumatol 2000;27:261–3.
17. Bruynesten K, Boers M, Kostense P, van der Linden S, van der
DP, et al. Influence of disease-modifying therapy on radiographic
Heijde D. Deciding on progression of joint damage in paired films
outcome in inflammatory polyarthritis at five years: results from a
of individual patients: smallest detectable difference or change.
large observational inception study. Arthritis Rheum 2003;48:
18. Little RJ, Rubin DB. Causal effects in clinical and epidemiological
23. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham
studies via potential outcomes: concepts and analytical ap-
CO III, et al. 2010 rheumatoid arthritis classification criteria: an
proaches. Annu Rev Public Health 2000;21:121–45.
American College of Rheumatology/European League Against
19. Prevoo ML, van ‘t Hof MA, Kuper HH, van Leeuwen MA, van de
Rheumatism collaborative initiative. Arthritis Rheum 2010;62:
Putte LB, van Riel PL. Modified disease activity scores that
include twenty-eight–joint counts: development and validation in a
24. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF,
prospective longitudinal study of patients with rheumatoid arthri-
Cooper NS, et al. The American Rheumatism Association 1987
tis. Arthritis Rheum 1995;38:44–8.
revised criteria for the classification of rheumatoid arthritis.
20. Smolen J, van der Heijde DM, St.Clair EW, Emery P, Bathon JM,
CGHS RATES 2011 BHOPAL NAME OF INVESTIGATION / TREATMENT PROCEDURE Rec Non NABH Hospitals Hospitals OPD Procedures 4 Suturing of wounds with local anesthesia5 Aspiration Plural Effusion - Diagnostic 6 Aspiration Plural Effusion - Therapeutic 23 Health Chec k up{ see Annexure (IV-a )for details} Opthalmology 30 Subconjunctival/subtenon’s injections in one eyes31 Subconjunct
The Journal of Political Philosophy: Volume 10, Number 2, 2002, pp. 153±174THEORIES of deliberative democracy consist of a set of principles thatare intended to establish fair terms of political cooperation in ademocratic society. Some theorists believe that the principles should refer onlyto the process of making political decisions in government or civil society.1The principles of deliberat
 RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
analyzed and the group of 152 patients who were
Baseline characteristics of the patients who were and those
who were not treated with disease-modifying antirheumatic drugswithin 3 months after the onset of synovitis*
Overall, 527 (79.7%) of the 661 analyzed patients
were started on DMARD therapy within 1 year follow-
ing symptom onset. Methotrexate was the most com-
monly prescribed first DMARD (336 of 527 [64%]),either as monotherapy (307 of 527 [58%]) or in combi-
nation with other DMARDs (hydroxychloroquine, sul-
fasalazine, leflunomide, or TNF-blocking drugs) (29 of
527 [5.5%]). Sulfasalazine was chosen in 66 patients
(13%), and leflunomide in 31 patients (6%). DMARDs
not taken into account in our analysis (mainly hydroxy-
chloroquine monotherapy) were prescribed in 90 pa-
Time to DMARD initiation was very hetero-
geneous, as shown in Figure 1. The proportion ofpatients starting DMARD therapy increased rapidly
treatment among patients starting DMARDs later may
over the first 6 months and leveled off thereafter. Of the
have worked against such a bias. Combination therapy
437 patients who started a DMARD of interest for the
was rarely chosen, which makes it unlikely that differ-
present study, 140 (32%) did so within the first 3 months
ences in the usage of combination therapy had an ef-
after symptom onset, and 205 (47%) within 6 months.
RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
analyzed and the group of 152 patients who were
Baseline characteristics of the patients who were and those
who were not treated with disease-modifying antirheumatic drugswithin 3 months after the onset of synovitis*
Overall, 527 (79.7%) of the 661 analyzed patients
were started on DMARD therapy within 1 year follow-
ing symptom onset. Methotrexate was the most com-
monly prescribed first DMARD (336 of 527 [64%]),either as monotherapy (307 of 527 [58%]) or in combi-
nation with other DMARDs (hydroxychloroquine, sul-
fasalazine, leflunomide, or TNF-blocking drugs) (29 of
527 [5.5%]). Sulfasalazine was chosen in 66 patients
(13%), and leflunomide in 31 patients (6%). DMARDs
not taken into account in our analysis (mainly hydroxy-
chloroquine monotherapy) were prescribed in 90 pa-
Time to DMARD initiation was very hetero-
geneous, as shown in Figure 1. The proportion ofpatients starting DMARD therapy increased rapidly
treatment among patients starting DMARDs later may
over the first 6 months and leveled off thereafter. Of the
have worked against such a bias. Combination therapy
437 patients who started a DMARD of interest for the
was rarely chosen, which makes it unlikely that differ-
present study, 140 (32%) did so within the first 3 months
ences in the usage of combination therapy had an ef-
after symptom onset, and 205 (47%) within 6 months.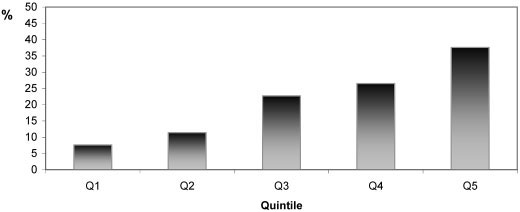 Figure 2. Percentage of patients starting disease-modifying antirheumatic drug treatment
Figure 2. Percentage of patients starting disease-modifying antirheumatic drug treatment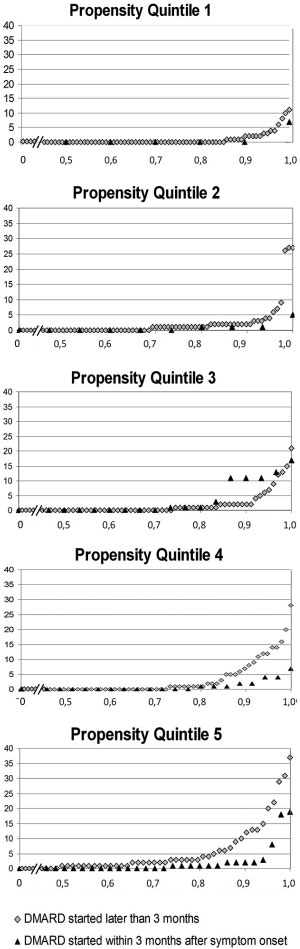 RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
with observations stemming from post hoc analyses fromclinical trials comparing intensive and less intensivetreatment, which have shown that patients with the worstprognostic profile especially benefit from intensive treat-ment, while those with relatively mild disease do wellwith less intensive therapy (20,21). Our observationscould be interpreted to suggest that the prognosticprofile is important not only in the choice betweenintensive and less intensive treatment strategies, but alsoin the choice between a very early start and a delayedone. Unfortunately, the propensity score cannot betranslated directly into prognostic variables.
RADIOGRAPHIC BENEFIT FROM VERY EARLY DMARD START
with observations stemming from post hoc analyses fromclinical trials comparing intensive and less intensivetreatment, which have shown that patients with the worstprognostic profile especially benefit from intensive treat-ment, while those with relatively mild disease do wellwith less intensive therapy (20,21). Our observationscould be interpreted to suggest that the prognosticprofile is important not only in the choice betweenintensive and less intensive treatment strategies, but alsoin the choice between a very early start and a delayedone. Unfortunately, the propensity score cannot betranslated directly into prognostic variables.