La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Labs.idi.harvard.edu
Treatment of Human Immunodeficiency Virus Infection with Hydroxyurea, Didanosine, and a Protease Inhibitor before Seroconversion Is Associated with Normalized Immune Parameters and Limited Viral Reservoir Franco Lori,1,2 Heiko Jessen,3 Judy Lieberman,4
1Research Institute for Genetic and Human Therapy, Washington, DC;Diana Finzi,6 Eric Rosenberg,5 Carmine Tinelli,2
2Istituto di Ricovero e Cura a Carattere Scientifico PoliclinicoBruce Walker,5 Robert F. Siliciano,6 S. Matteo, Pavia, Italy; 3Jessen Praxis, Berlin, Germany; 4Centerfor Blood Research and 5Partners AIDS Research Center andand Julianna Lisziewicz1,2 Infectious Disease Division, Massachusetts General Hospital, andHarvard Medical School, Boston, Massachusetts; 6Department ofMedicine, Johns Hopkins University School of Medicine, Baltimore,Current treatments for human immunodeficiency virus (HIV) require uninterrupted drug administration because they are unable to reconstitute the immune response and do not affect the viral reservoir. Ten patients were treated during acute HIV infection before complete Western blot (WB) seroconversion with the combination of hydroxyurea, didanosine, and indinavir. This treatment was associated with the normalization of some immune parameters and functions. No loss of naive CD4 T lymphocytes was observed, and recovery of up to 35% of naive CD8 T lymphocytes occurred in several weeks. A vigorous HIV-specific T helper response (stimulation index 18) was observed in 7 of 8 patients treated before complete WB seroconversion but in only 1 of 5 controls treated after seroconversion. In addition, a limited latent viral reservoir (!0.02–0.5 infectious units/106 cells) was documented in quiescent pe- ripheral blood lymphocytes after treatment initiated before complete WB seroconversion.
When treatment of human immunodeficiency virus (HIV)
initiated during acute infection appears to normalize CD4/CD8
infection should be initiated remains an important unresolved
ratios [2] and HIV-specific T helper responses [1]. Early after
question. Reasons to delay treatment include the likelihood of
infection, renewal of CD4 T lymphocytes is still achievable [3]
increased long-term toxicity, higher cost, and earlier develop-
and T cell receptor damage can be fixed [4]. It is not exactly
ment of drug resistance, thus narrowing the chances of later
clear, however, when during acute infection the treatment must
treatment options. Reasons to start treatment early are mainly
be started in order to normalize these parameters.
theoretical and rely on the possibility that therapeutic inter-
The spread of HIV throughout the body occurs in the first
vention might limit damage to the immune system and confine
few weeks [5]. As early as 10 days after the onset of the first
symptoms of primary HIV infection (PHI), a reservoir of rep-
The immune system is impaired by HIV infection. CD4 T
lication-competent virus, consisting of latent proviral DNA in
lymphocytes are depleted, the CD4/CD8 ratio is decreased, and
quiescent T lymphocytes, becomes established [5, 6]. This res-
HIV-specific T helper cell responses are lost soon after acute
ervoir does not significantly decrease after years of HAART
infection [1]. Highly active antiretroviral treatment (HAART)
[6–8]. It remains to be shown whether very early treatment afteracute infection might restrict the initial spread of virus andlimit the expansion of the pool of latently infected cells.
Received 11 January 1999; revised 12 July 1999; electronically published
Because latently infected resting T lymphocytes represent a
major viral reservoir [6–8] and because infection of macro-
Presented in part: 12th World AIDS Conference, 28 June–3 July 1998,
phages may be important in initial stages of infection following
All patients provided signed informed consent before the start of treat-
sexual, parenteral, and vertical transmission [9–12], drugs af-
ment. The protocol was approved by institutional review boards of the
fecting these compartments are good candidates for early treat-
authors’ institutions. Human experimentation guidelines of the US De-partment of Health and Human Services and of the authors’ institutions
ment of HIV infection. Hydroxyurea and didanosine are par-
were followed in the conduct of clinical research, as were the principles
ticularly effective antiretroviral drugs in quiescent lymphocytes
outlined in the Declaration of Helsinki (1990).
Grant support: ISS (grant 30.A.0.32); Bristol-Myers Squibb.
and macrophages [13, 14]. However, viral replication is very
Reprints or correspondence: Dr. Franco Lori, RIGHT, Medical-Dental
high in activated proliferating lymphocytes early after infection.
Bldg. SW307, 3900 Reservoir Rd., N.W., Washington, DC 20007 (RIGHT
Therefore, potent antiretroviral drugs, such as protease inhib-
itors, that inhibit the production of infectious virions should
The Journal of Infectious Diseases 1999; 180:1827–32
add substantially to the effective treatment of early HIV in-
1999 by the Infectious Diseases Society of America. All rights reserved.
fection. In this study, we evaluated a drug regimen of hydroxy-
urea, didanosine, and indinavir as an early treatment for HIV
control antigen at a concentration of 1.5 mg/mL, which is equal to
the baculovirus antigen concentration in the recombinant p24 pro-tein. The stimulation index was calculated as the mean counts perminute (cpm) of incorporated [3H]thymidine from cells stimulatedwith p24, divided by the mean cpm from cells stimulated with
Statistical analysis was performed by the
All patients with a documented history of HIV in-
Mann-Whitney nonparametric U test (two tailed). P values are
fection of р1 year were consecutively enrolled, independent of virus
load, CD4 cell count, CD4/CD8 ratio, age, and sex. To be eligiblefor the study, each patient needed to have at least 2 independentconsecutive assays (at different time points) that were positive for
the HIV in the plasma. All patients had presented with signs orclinical symptoms typical of PHI, most commonly a flu-like syn-
Early HIV suppression leads to normalization of immunologic
drome with fever and sore throat. At the time of enrollment, pa-
Ten patients were treated with hydroxyurea, dida-
tients were distinguished on the basis of Western blot (WB) analysis.
nosine, and indinavir before complete WB seroconversion. The
Complete seroconversion was defined as strong WB positivity for
effects of this treatment on virus load have been described pre-
antibodies against у4 of the following viral proteins: gp160, gp120,
viously in this cohort [2]. In brief, plasma viremia (1550,000
p65, p55, gp41, p32, p24, and p18. As a result of this screening,10 patients were enrolled before complete seroconversion and 5
copies/mL before treatment) became undetectable (!50 copies/
patients (controls) after complete seroconversion (but within 1 year
mL) in all patients. In the present study, we analyzed the effect
of infection). Enrolled patients were naive to antiretroviral drugs.
of this early treatment on immunologic parameters. After
All 15 patients received didanosine (200 mg twice/day) and indi-
46 ע 21 weeks of therapy, the changes in CD4 and CD8 cell
navir (800 mg 3 times/day); patients weighing !60 kg were also
count and CD4/CD8 ratio were ϩ154, Ϫ544, and ϩ0.46, re-
given hydroxyurea (300 mg 3 times/day), whereas those weighing
spectively. A longitudinal analysis of the changes of naive CD4,
160 kg were given hydroxyurea (400 mg 3 times/day). Plasma vi-
naive CD8, and activated CD8 T lymphocytes was performed
remia was measured by ultrasensitive polymerase chain reaction
(figure 1A). An increase of naive CD8 and a decline of activated
(sensitivity, 50 equivalent/mL; Roche, Nutley, NJ). CD4 and CD8
CD8 T lymphocytes was observed 4 weeks after treatment,
T lymphocyte counts/mm3 were done by standard techniques.
whereas the proportion of naive CD4 T lymphocytes remained
For detection of naive T lymphocytes, pe-
lated by ficoll-hypaque density centrifugation from heparinized
WB analysis was followed longitudinally in these patients.
blood, were suspended in 100 mL of FACS buffer (PBS with 2%
In most, a complete seroconversion eventually developed, even
fetal calf serum) before the addition of 4 mL of CD45RA–
though HIV was below the level of detection in the plasma.
fluorescein isothiocynate (FITC) (monoclonal antibody [MAb]
The progression of the seroconversion, however, was very slow.
ALB11; Immunotech, Hamburg, Germany), 4 mL of 1 : 10 dilution
In some patients, complete seroconversion was evident only 11
of CD62L-phycoerythrin (PE) (MAb SCFI28T17G6; Coulter, Hi-
year after initiation of treatment. In 1 case, in which only p24
aleah, FL), and 4 mL of either CD8-Cy5 or CD4-Cy5 (MAb 13B8.2;
immunoreactivity was detected at the initiation of treatment,
Immunotech). For detection of activated (CD38ϩDRϩ) CD8 T lym-
no major changes in WB antibodies have yet been observed
phocytes, 4 mL of CD38-PE (MAb T16; Immunotech), 4 mL of
HLA-DR–FITC (MAb 357; Immunotech), and 4 mL of CD8-Cy5
Eight of 10 patients in this cohort were tested for HIV-specific
or 4 mL of IgG-FITC, -PE, and -Cy5–conjugated isotype-matched
T helper responses (figure 1B). With one exception (patient 7;
controls (Immunotech) were used. Flow cytometry analysiswas done on a tightly gated lymphocyte population, by use of
figure 1B), all patients tested before complete WB seroconver-
FACscalibur (Becton Dickinson, San Jose, CA).
sion had a vigorous CD4 T cell proliferative response to p24,
with stimulation indices of 8.3–46.1. These results were com-
resuspension of PBMC in RPMI 1640 medium containing 10%
pared with those of a control group of patients who also were
human AB serum, HEPES buffer, L-glutamine, and penicillin-strep-
enrolled on the basis of a recent diagnosis of PHI (see Methods)
tomycin. Assays were performed on 23 February 1998, except for
but who presented with complete WB seroconversion. Only 1
patient 1, whose assay was done on 24 June 1998. Cells (105/well)
(patient C3; figure 1B) of 5 control subjects had a robust CD4
were cultured in 6 replicate wells of 96-well U-bottomed plates in
T cell proliferative response to p24. Owing to the lack of base-
the presence of HIV recombinant p24 protein at a final concen-
line (before treatment) samples, we could not establish whether
tration of 5 mg/mL. Six days later, the cells were pulsed with
the early treatment rapidly restored or prevented the loss of a
[3H]thymidine at 1.0 mCi per well, and uptake was measured 6 h
CD4 T cell proliferative response. Vigorous T helper responses,
later by scintillation counter (Topcount; Packard Instruments, Mer-iden, CT). The HIV p24 protein (Protein Science, Meriden, CT) is
however, were detected as early as 34 days after treatment
a recombinant protein derived from the gag gene of HIV (NY-5
strain) produced in a baculovirus expression system with proved
Early treatment limits the establishment of HIV reservoirs.
90%–95% purity. A mixture of baculovirus proteins was used as a
We examined whether very early treatment might confine the
Figure 1. A, Longitudinal follow-up of CD4 naive, CD8 naive, and CD8 activated T lymphocytes. Samples were collected at baseline and at
regular intervals for 24 weeks after treatment. CD4 naive (% of total CD4 cells), CD4ϩCD62LϩCD45RAϩ; CD8 naive (% of total CD8 cells),CD8ϩCD62LϩCD45RAϩ; CD8 activated (% of total CD8 cells), CD8ϩCD38ϩDRϩ. B, Human immunodeficiency virus (HIV)–specific T helperproliferative responses in HIV-infected patients treated with hydroxyurea, didanosine, and indinavir before (patients 1–10) and after (patientsC1–C5) complete Western blot seroconversion.
size of the HIV reservoir by quantitating the number of latently
dard assay; table 1). A second attempt with an ultrasensitive
infected CD4 T lymphocytes in 6 of 10 patients who agreed to
assay analyzing a much higher number of cells (
donate the necessary amount of blood for this analysis (∼200
table 1) was necessary to recover replication-competent HIV.
mL). A previously described assay [6], able to detect latently
With this more sensitive assay, virus was recovered from the
infected CD4 T lymphocytes in 18 of 18 chronically infected
blood of 5 of 6 patients studied, although at relatively low levels.
patients on HAART, failed to detect replication-competent HIV
In 1 case (patient 10; table 1), no HIV could be isolated, even
in 3 of 4 patients treated before complete seroconversion (stan-
37 ϫ 10 cells were analyzed. Rates of latent HIV in rest-
Latent human immunodeficiency virus after early treatment.
Cells from patients 2, 9, and 10 were tested by both standard and ultrasensitive assay. ND, not done;
a These patients also received delavirdine, 400 mg, 3 times/day.
ing peripheral blood CD4 T cells of our patients were compared
activated CD8 T lymphocytes, antibodies increase slowly, and
with values measured [6] in 18 chronically infected patients who
had been aviremic on HAART for up to 2.5 years (average,
Our data showed that the percentages of naive T lymphocytes
1.36 latent HIV/106 cells). The frequency of latently infected
either never deteriorated or were rapidly restored. These results
CD4 T lymphocytes in our early treated patients was much
contrast with a previous report showing that the recovery of
lower (average, 0.3 latent HIV/106 cells), and the difference was
naive CD4 and CD8 populations was significant only after 12
months in patients receiving HAART in late stages of chronic
Although these results confirm recent studies [5, 6] that early
HIV infection [15]. HIV infection is characterized by a pro-
treatment does not prevent the establishment of latent cellular
gressive loss of naive CD4 and CD8 T lymphocytes, possibly
reservoirs for HIV, our data show that treatment before sero-
because of a limited renewal/production by the bone marrow
conversion with hydroxyurea, didanosine, and indinavir is as-
or thymus [16–19]. If antiretroviral treatment reverts the loss
sociated with an unusually low frequency of latently infected
of naive cells, it is conceivable that the time required to replenish
cells. We could not discriminate the relative contribution of
the naive T lymphocyte pool will become progressively longer
treatment timing from the role of the particular combination
during the progression of the infection. Our findings provide
of drugs used in our experiments. However, not all patients
evidence that the earliest treatment leads to the fastest recovery
treated early had the lowest levels of latent HIV. For example,
of the naive cell repertoire. Furthermore, early treatment might
in patient 4 (table 1), HIV was detectable by use of a standard
be the only chance to limit the establishment and expansion of
assay with a frequency of latently infected cells of 0.5 infectious
latent HIV reservoirs. In contrast to the lack of decay of viral
units/106 cells. Similar frequencies were found in chronically
reservoir observed after treatment of chronic HIV infection [20],
the small size of the latent viral reservoir observed in our pa-tients might be due to a limited expansion or to a more rapiddecay after early treatment. Discussion
Our results provide a more precise timing for the optimal
recovery of HIV-specific T helper response previously described
Our results suggest that early treatment may have a major
during the treatment of acute infection [1]. In fact, treatment
effect on the outcome of HIV infection. Within a few months
before complete WB seroconversion provided the highest
of infection, the majority of untreated patients have reached a
chance of normalization of these responses. Starting HAART
state of equilibrium characterized by high plasma viremia with
during chronic progressive infection is usually associated with
extensive HIV reservoir, reduced CD4 cell counts, decreased
the failure to normalize HIV T helper responses [15, 21, 22].
numbers of naive CD4 and CD8 T lymphocytes, and increased
A notable exception is represented by a group of patients
activated CD8 T lymphocytes, high antibody levels, and an
treated during chronic progressive infection with the combi-
absence of T helper response. We have shown that if treatment
nation of only 2 drugs, hydroxyurea and didanosine [23].
is initiated early, the scenario might be different: Viremia be-
This study was not designed to assess the specific contri-
comes undetectable in the plasma, the HIV reservoir is circum-
bution of the combination of hydroxyurea, didanosine, and
scribed in some patients, CD4 cells and naive CD4 and CD8
indinavir. The use of hydroxyurea, a cytostatic and potentially
T lymphocyte percentages normalize with modest increases of
immunosuppressive drug, during the course of an infection
causing immunodeficiency has raised theoretical concerns, par-
early HIV-1 infection: effect of highly active antiretroviral therapy. Nat
ticularly in view of the lack of CD4 cell increase after treatment
Med 1998; 4:794–801.
4. Lori F, Jessen H, Lieberman J, Clerici M, Tinelli C, Lisziewicz J. Immune
with hydroxyurea plus didanosine or didanosine and stavudine,
restoration by combination of a cytostatic drug (hydroxyurea) and anti-
shown in previous trials [24, 25]. In the present study, however,
HIV drugs (didanosine and indinavir). AIDS Res Hum Retroviruses
no signs of immunosuppression were detected. All the immune
1999; 15:619–24.
parameters tested showed improvement, and there was a clear
5. Chun TW, Engel D, Berrey MM, Shea T, Corey L, Fauci AS. Early estab-
increase in CD4 T lymphocytes. Paradoxically, the cytostatic
lishment of a pool of latently infected, resting CD4(ϩ) T cells during
primary HIV-1 infection. Proc Natl Acad Sci USA 1998; 95:8869–73.
effects of hydroxyurea on CD4 T lymphocytes might be ad-
6. Finzi D, Hermankova M, Pierson T, et al. Identification of a reservoir for
vantageous, since resting cells do not support HIV replication
HIV-1 in patients on highly active antiretroviral therapy. Science 1997;
[26–28]. If immunostimulation (primarily represented by CD8
T lymphocyte proliferation [29]) and consequent T cell–
7. Chun TW, Stuyver L, Mizell SB, et al. Presence of an inducible HIV-1 latent
mediated immunopathology play a major role in the immu-
reservoir during highly active antiretroviral therapy. Proc Natl Acad Sci
nopathogenesis of HIV infection [30, 31], cytostatic treatment
USA 1997; 94:13193–7.
8. Wong JK, Hezareh M, Gunthard HF, et al. Recovery of replication-com-
petent HIV despite prolonged suppression of plasma viremia. Science
In conclusion, this study represents a first step toward ad-
1997; 278:1291–5.
dressing the important question of when to initiate HIV infec-
9. Zhu T, Mo H, Wang N, et al. Genotypic and phenotypic characterization
tion treatment, and controlled studies are required in order to
of HIV-1 patients with primary infection. Science 1993; 261:1179–81.
provide a conclusive answer. Treatment before complete sero-
10. van’t Wout AB, Kootstra NA, Mulder-Kampinga GA, et al. Macrophage-
tropic variants initiate human immunodeficiency virus type 1 infection
conversion, however, appears desirable because, although re-
after sexual, parenteral, and vertical transmission. J Clin Invest 1994; 94:
covery of immune functions and normalization of some im-
mune parameters have been demonstrated when treatment is
11. Reinhardt PP, Reinhardt B, Lathey JL, Spector SA. Human cord blood
initiated during chronic HIV infection, recovery was incomplete
mononuclear cells are preferentially infected by non–syncytium-inducing,
and did not occur in all patients [15, 21, 22]. Our data suggest
macrophage-tropic human immunodeficiency virus type 1 isolates. J Clin
that the time before complete seroconversion might provide an
Microbiol 1995; 33:292–7.
12. Cameron PU, Lowe MG, Sotzik F, Coughlan AF, Crowe SM, Shortman K.
important window for therapeutic intervention to prevent ir-
The interaction of macrophage and non-macrophage tropic isolates of
reversible immune damage. Limiting the number of resting in-
HIV-1 with thymic and tonsillar dendritic cells in vitro. J Exp Med
fected cells very early after infection might also have implica-
1996; 183:1851–6.
tions in the control of HIV replication. Of interest, only
13. Perno CF, Yarchoan R, Cooney DA, et al. Replication of human immu-
examples of complete virus suppression without rebound after
nodeficiency virus in monocytes: granulocyte/macrophage colony-stimu-
lating factor (GM-CSF) potentiates viral production yet enhances the
drug withdrawal have been reported in patients treated early
antiviral effect mediated by 3-azido-2 3 -dideoxythymidine (AZT) and
after infection [2, 32, 33]. Early treatment may therefore be the
other dideoxynucleoside congeners of thymidine. J Exp Med 1989; 169:
key to developing functional immunosurveillance to control
virus production without permanent drug therapy. However,
14. Lori F, Malykh A, Cara A, et al. Hydroxyurea as an inhibitor of human
the immunologic correlates that predict control of viremia after
immunodeficiency virus type 1 replication. Science 1994; 266:801–5.
discontinuation of therapy and the relative contribution of the
15. Autran B, Carcelain G, Li TS, et al. Positive effects of combined antiretroviral
therapy on CD4ϩ T cell homeostasis and function in advanced HIV dis-
elements required to induce such control need to be analyzed
ease. Science 1997; 277:112–6.
in randomized, controlled clinical studies.
16. Hellerstein M, Hanley MB, Cesar D, et al. Directly measured kinetics of
circulating T lymphocytes in normal and HIV-1–infected humans. Nat
Acknowledgments
Med 1999; 5:83–9.
17. Douek DC, McFarland RD, Keiser PH, et al. Changes in thymic function
We thank Reinhold Schroeder and Michael Geldermann for organ-
with age and during the treatment of HIV infection. Nature 1998; 396:
izing sample collection, Linda Trimble and Heidi Sprang for assistance
18. Pantaleo G. Unraveling the strands of HIV’s web. Nat Med 1999; 5:27–8.
in immunologic and virologic analysis, and Sylva Petrocchi for editorial
19. Roederer M. Getting to the HAART of T cell dynamics. Nat Med 1998; 4:
assistance. We also thank Michael Stevens for helpful discussion.
20. Finzi D, Blankson J, Siliciano JD, et al. Latent infection of CD4ϩ T cells
provides a mechanism for lifelong persistence of HIV-1, even in patients
on effective combination therapy. Nat Med 1999; 5:512–7. References
21. Plana M, Garcia F, Gallart T, Miro JM, Gatell JM. Lack of T-cell prolif-
1. Rosenberg ES, Billingsley JM, Caliendo AM, et al. Vigorous HIV-1–specific
erative response to HIV-1 antigens after 1 year of highly active antiretro-
CD4ϩ T cell responses associated with control of viremia. Science 1997;
viral treatment in early HIV-1 disease: Immunology Study Group of Span-
ish EARTH-1 Study. Lancet 1998; 352:1194–5.
2. Lisziewicz J, Jessen H, Finzi D, Siliciano RF, Lori F. HIV-1 suppression by
22. Pitcher CJ, Quittner C, Peterson DM, et al. HIV-1–specific CD4ϩ T cells are
early treatment with hydroxyurea, didanosine, and a protease inhibitor.
detectable in most individuals with active HIV-1 infection, but decline
Lancet 1998; 352:199–200.
with prolonged viral suppression. Nat Med 1999; 5:518–25.
3. Fleury S, de Boer RJ, Rizzardi GP, et al. Limited CD4ϩ T-cell renewal in
23. Lori F, Rosenberg E, Lieberman J, et al. Hydroxyurea and didanosine long-
term treatment prevents HIV breakthrough and normalizes immune pa-
phocytes as an inducible virus reservoir in HIV-1 infection. Science
rameters. AIDS Res Hum Retroviruses 1999; 15:1333–8. 1991; 254:423–7.
24. Lori F, Malykh AG, Foli A, et al. Combination of a drug targeting the cell
29. Wolthers KC, Bea G, Wisman A, et al. T cell telomere length in HIV-1
with a drug targeting the virus controls human immunodeficiency virus
infection: no evidence for increased CD4ϩ T cell turnover. Science
type 1 resistance. AIDS Res Hum Retroviruses 1997; 13:1403–9. 1996; 274:1543–7.
25. Rutschmann OT, Opravil M, Iten A, et al. A placebo-controlled trial of
30. Zinkernagel RM, Hengartner H. HIV: games that viruses play. Nature
didanosine plus stavudine, with and without hydroxyurea, for HIV in-
1991; 354:433–4.
fection: the Swiss HIV Cohort Study. AIDS 1998; 12:F71–7.
31. Zinkernagel RM, Hengartner H. Virally induced immunosuppression. Curr
26. Zagury D, Bernard J, Leonard R, et al. Long-term cultures of HTLV-
Opin Immunol 1992; 4:408–12.
III–infected T cells: a model of cytopathology of T-cell depletion in AIDS.
32. Vila J, Nugier F, Bargues G, et al. Absence of viral rebound after treatment
Science 1986; 231:850–3.
27. Zack JA, Arrigo SJ, Weitsman SR, Go AS, Haislip A, Chen IS. HIV-1 entry
of HIV-infected patients with didanosine and hydroxycarbamide. Lancet
into quiescent primary lymphocytes: molecular analysis reveals a labile,
1997; 350:635–6.
latent viral structure. Cell 1990; 61:213–22.
33. Lisziewicz J, Rosenberg E, Lieberman J, et al. Control of HIV despite the
28. Bukrinsky MI, Stanwick TL, Dempsey MP, Stevenson M. Quiescent T lym-
discontinuation of antiretroviral therapy. N Engl J Med 1999; 340:1683–4.
Differential Permethrin Susceptibility of Head Lice Sampled in the United States and Borneo Richard J. Pollack, PhD; Anthony Kiszewski, DSc; Philip Armstrong, DSc; Christine Hahn, MD; Nathan Wolfe, DSc;Hasan Abdul Rahman, MD; Kayla Laserson, DSc; Sam R. Telford III, DSc; Andrew Spielman, ScD Background: Pediculiasis is treated aggressively in the of the Sabahan children were so exposed. U
GRANT APPLICATION Fiscal Year Number B-19 Applicant Department of Ophthalmology Meeting Date Description of Request Department of Ophthalmology Research Fund Amount Requested $ 150,000 Contact Person Purpose: To provide research funds for Department of Ophthalmology Faculty. Please see attached. How will item be identified as being purchased by Lio
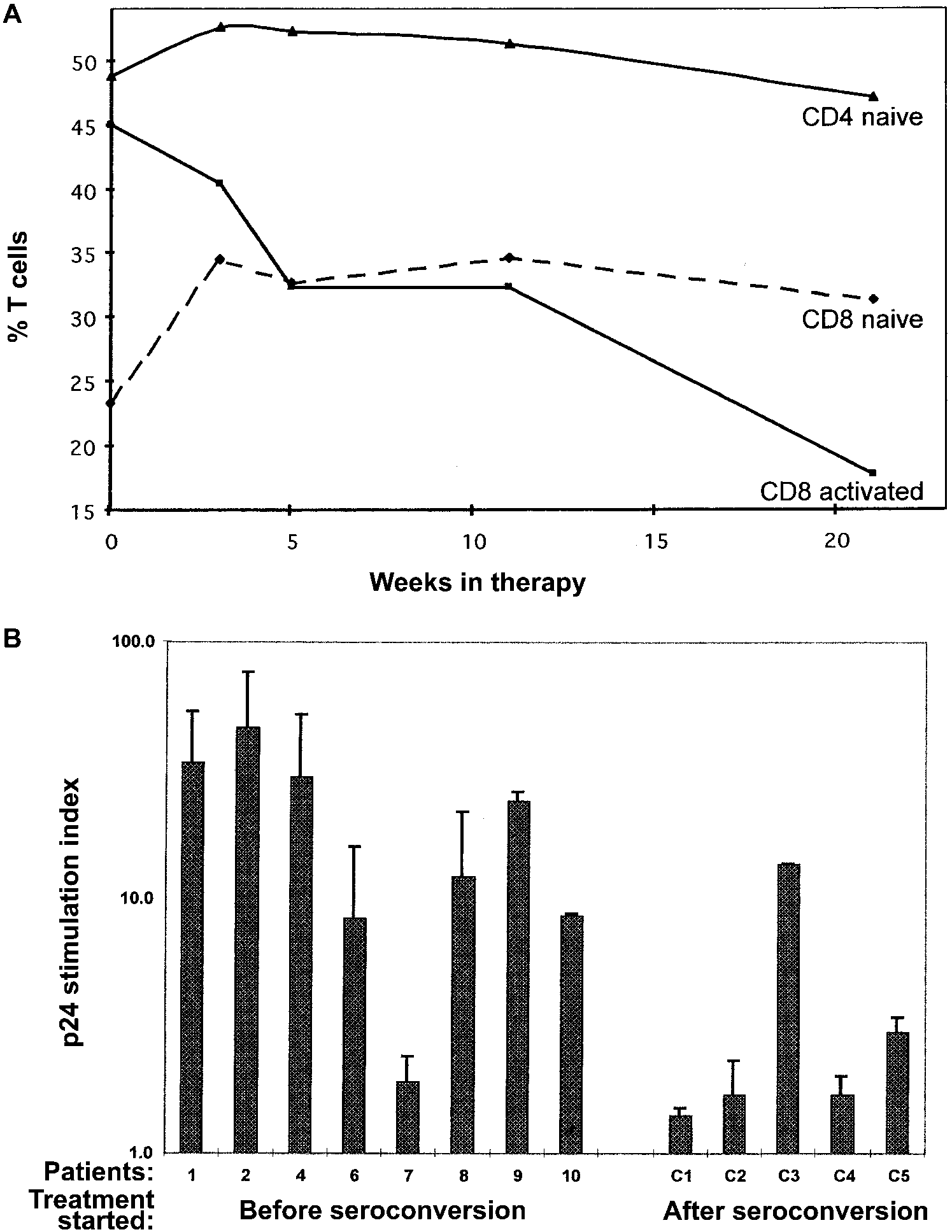 Figure 1.
Figure 1.