La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Jogc-may-06.vp
GYNAECOLOGY GYNAECOLOGY Use of Misoprostol Before Hysteroscopy: A Systematic Review Joan M. G. Crane, MD, FRCSC, Sarah Healey, MD, FRCSC Department of Obstetrics and Gynecology, Memorial University of Newfoundland, St John’s NL Abstract Résumé Objective: To evaluate the effectiveness of administering misoprostol Objectif : Évaluer l’efficacité de l’administration de misoprostol avant
prior to hysteroscopy in achieving cervical dilatation and reducing
une hystéroscopie en vue d’obtenir une dilatation cervicale et de
complications including cervical laceration.
réduire les complications (y compris les lacérations cervicales). Data Sources: Computerized searches of MEDLINE, PubMed and Sources de données : Des recherches informatisées ont été menées
EMBASE were conducted using the key words “hysteroscopy” and
dans MEDLINE, PubMed et EMBASE au moyen des mots clés
“misoprostol.” References from identified publications were
hysteroscopy et misoprostol. Les références des publications
manually searched and cross-referenced to identify additional
identifiées ont fait l’objet d’une recherche manuelle et ont été
recoupées en vue d’identifier des articles pertinents additionnels. Study Selection: We included randomized clinical trials that
compared women undergoing hysteroscopy who received
Sélection des études : Nous avons inclus les essais cliniques
misoprostol before the procedure with those who received placebo.
randomisés qui comparaient les femmes subissant une
Studies were excluded if there was no control group, if placebo
hystéroscopie qui recevaient du misoprostol avant l’intervention à
was not used, if women were not randomized, or if only the
celles qui recevaient un placebo. Les études étaient exclues si
abstract was available. Ten of 19 articles identified met the criteria
elles ne comptaient pas de groupes témoins, si elles ne faisaient
pas appel à un placebo, si leurs participantes n’étaient pasrandomisées ou si seul leur résumé était disponible. Dix des
Data Extraction and Synthesis: The two co-authors separately
19 articles identifiés ont satisfait aux critères de l’analyse
abstracted data. Any differences in data abstraction were resolved
through discussion, and a consensus was reached. QUORUMguidelines for meta-analyses and systematic reviews of
Extraction et synthèse des données : Les deux co-auteurs ont
randomized controlled trials were followed.
procédé séparément au résumé des données. Toutes les
In premenopausal women, misoprostol before hysteroscopy
différences quant au résumé des données ont été résolues au
resulted in a reduced need for further cervical dilatation (relative
moyen de discussions; ainsi, un consensus a pu être atteint. Les
risk [RR] = 0.61; 95% confidence interval [CI] = 0.51, 0.73), a lower
lignes directrices QUORUM visant les méta-analyses et les
rate of cervical laceration (RR 0.22; 95% CI 0.09, 0.56) and
analyses systématiques d’essais comparatifs randomisés ont été
increased cervical dilatation (weighted mean difference 2.64; 95%
CI 1.73, 3.54). In premenopausal women, misoprostol also resulted
Chez les femmes préménopausées, l’administration de
in a higher rate of side effects, including vaginal bleeding (RR
misoprostol avant l’hystéroscopie a entraîné une diminution de la
11.09; 95% CI 3.08, 40.00), cramping (RR 7.98; 95% CI 3.38,
nécessité de poursuivre la dilatation cervicale (risque relatif [RR] =
18.84), and elevated temperature (RR 5.24; 95% CI 1.37, 20.09).
0,61; intervalle de confiance [IC] à 95 % = 0,51, 0,73), un taux
For every four premenopausal women who received misoprostol
moindre de lacération cervicale (RR : 0,22; IC à 95 % : 0,09, 0,56)
prior to hysteroscopy, one woman avoided the need for further
et une dilatation cervicale accrue (différence moyenne pondérée :
cervical dilatation. For every 12 premenopausal women receiving
2,64; IC à 95 % : 1,73, 3,54). Chez les femmes préménopausées,
misoprostol, one cervical laceration was avoided.
l’administration de misoprostol a également entraîné un taux accru
Conclusion: In premenopausal women, misoprostol appears to be
d’effets indésirables, y compris les saignements vaginaux (RR :
promising as a cervical ripening agent prior to hysteroscopy,
11,09; IC à 95 % : 3,08, 40,00), les crampes (RR : 7,98; IC à
although further research is needed to identify the ideal dose,
95 % : 3,38, 18,84) et une hausse de la température (RR : 5,24; IC
route, and timing. Further research in postmenopausal women or
à 95 % : 1,37, 20,09). Pour chaque groupe de quatre femmes
those receiving GnRH agonists is also needed, to determine
préménopausées ayant reçu du misoprostol avant une
whether misoprostol is effective in cervical ripening in this
hystéroscopie, une femme a pu éviter d’avoir besoin d’une
dilatation cervicale accrue. Pour chaque groupe de 12 femmespréménopausées ayant reçu du misoprostol, un cas de lacérationcervicale a pu être évité. Conclusion : Chez les femmes préménopausées, le misoprostol Key Words: Misoprostol, hysteroscopy, meta-analysis
semble prometteur en tant qu’agent de maturation du col avantune hystéroscopie. Cependant, de plus amples recherches
s’avèrent requises pour en identifier la dose, la voie
d’administration et la posologie idéales. De plus amplesrecherches chez les femmes postménopausées ou chez les
femmes recevant des agonistes de la gonadolibérine s’avèrent
MAY JOGC MAI 2006 l GYNAECOLOGY
également requises, et ce, afin de déterminer l’efficacité du
outcomes. Any differences in data abstraction were
misoprostol pour la maturation cervicale chez cette population.
resolved through discussion, and a consensus was reached.
J Obstet Gynaecol Can 2006;28(5):373–379
QUORUM guidelines for meta-analyses and systematic
INTRODUCTION
reviews of randomized controlled trials were followed.8 Sta-tistical analyses were conducted using the computer pro-
Hysteroscopy is a common gynaecologic procedure gram Review Manager 4.27 (Cochrane Collaboration,
used to investigate and treat menstrual disorders,
Oxford, UK). Heterogeneity among trials for each outcome
postmenopausal bleeding, infertility, and recurrent
was evaluated by chi-square analysis. A random effects
pregnancy loss.1,2 The procedure requires that the cervical
model was used if there was significant heterogeneity (P <
canal be dilated enough to allow passage of the
0.10). For categorical data the relative risk of each outcome
hysteroscope. Complications of hysteroscopy include cervi-
for each study was calculated, and a summary relative risk
cal laceration, uterine perforation, and creation of a false
and 95% CI were calculated. For continuous data a
passage during the attempt to dilate the cervix, which may
weighted mean difference and 95% CI were calculated. A P
value of less than 0.05 was considered significant. Analyses
Misoprostol, a prostaglandin E1 analogue used in the pre-
were planned in advance for (1) premenopausal women,
vention and treatment of gastric ulcers induced by
(2) postmenopausal women and premenopausal women
non-steroidal anti-inflammatory drugs (NSAIDs), has been
receiving GnRH agonists, and (3) both groups of women
increasingly used in obstetrics and gynaecology as a cervical
combined. The number of women needed to treat to avoid
ripening agent.5–7 The purpose of this meta-analysis was to
the need for cervical dilatation prior to hysteroscopy was
evaluate the effectiveness of misoprostol prior to
hysteroscopy in achieving preprocedural cervical dilatation
premenopausal nulliparous women and of premenopausal
and reducing the need for mechanical dilatation with its
women undergoing operative hysteroscopy.
Sample size of the meta-analysis for the primary outcome ofneed for cervical dilatation prior to hysteroscopy was based
on a reduction in the primary outcome from 50% to 33%,with a two-tailed á = 0.05 and â = 0.20, requiring 143
We performed searches of MEDLINE, PubMed, andEMBASE using the keywords “hysteroscopy” and
“misoprostol” to identify studies involving human subjects
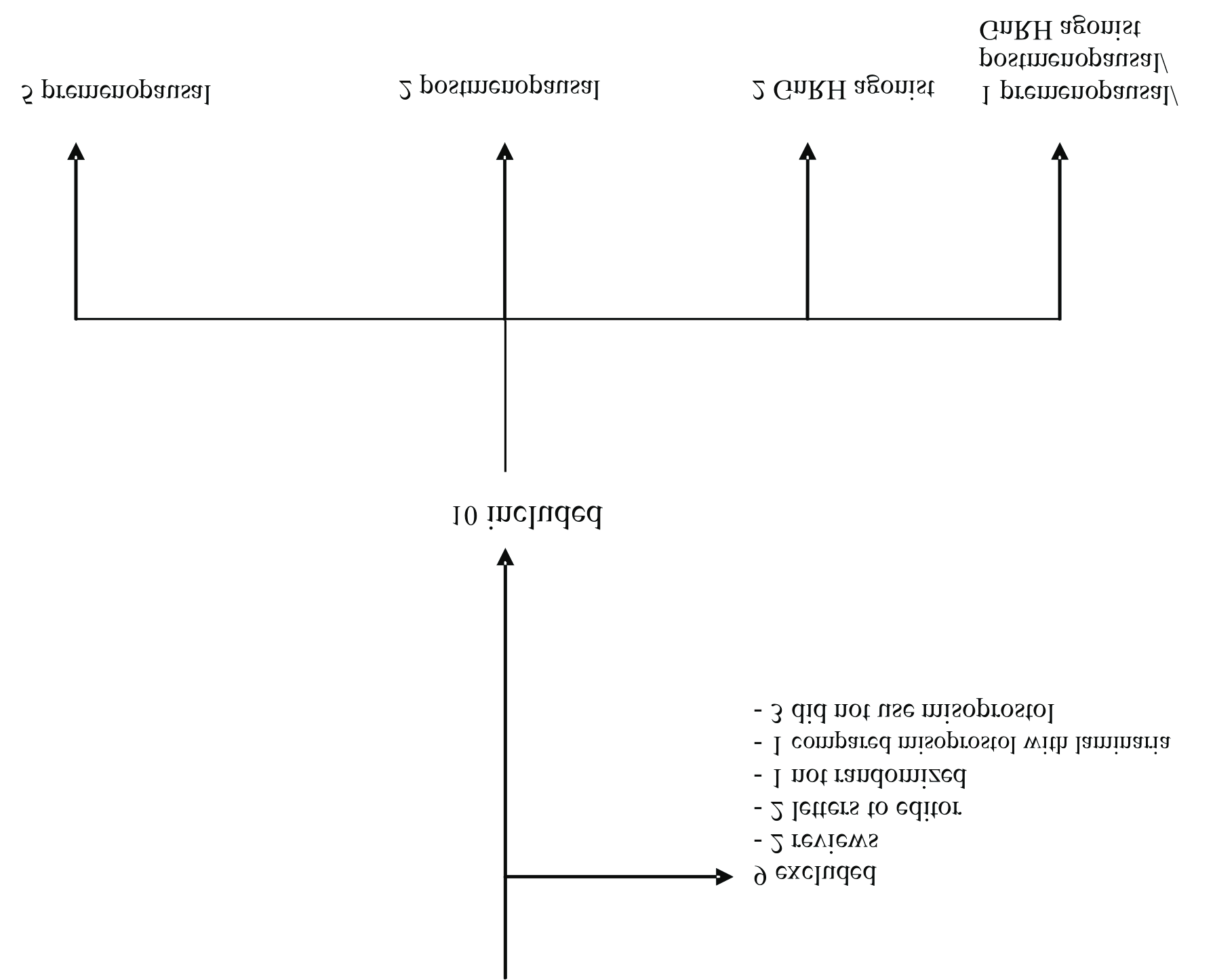
Of the 19 studies2–5,10–24 identified from the literature
published in English between January 1980 and April 2005.
search, ten10–19 were included in the meta-analysis (Figure).
References from these publications were searched manually
Nine studies were excluded: two were reviews,5,23 two were
and cross-referenced to identify additional relevant articles.
letters to the editor commenting on previous randomized
Because of lack of details regarding study methods and
clinical trials,21,22 one study was not randomized,20 one
results, abstracts and unpublished works were not included.
study compared misoprostol with laminaria,24 and three
Study Selection
studies did not use misoprostol.2–4 One author was con-
Studies considered eligible were randomized clinical trials
tacted to clarify information presented in the published
that compared the effects of misoprostol and placebo given
before the procedure in women undergoing hysteroscopy.
Table 1 summarizes the ten randomized clinical trials
Studies were ineligible if there was no control group, if pla-
included in the meta-analysis. Five of the studies included
cebo was not used, if treatment was not randomized, or if
only the abstract was published. The primary outcome was
postmenopausal women or those receiving GnRH
the need for further mechanical cervical dilatation. Second-
agonists,15–17,19 and one study included both groups of
ary outcomes were complications (particularly cervical
laceration and uterine perforation), side effects (nausea,
diarrhea, vaginal bleeding, cramping, and elevated tempera-
scopy,11,13–15,18,19 and one study evaluated both.12
ture), and the continuous measure of cervical dilatation.
Table 2 summarizes the outcomes of misoprostol adminis-
If an abstract described a study that did not meet eligibility
tration before hysteroscopy for all women, revealing a sig-
criteria, it was not reviewed further. Papers for all other
nificant reduction in the need for further dilatation prior to
abstracts were reviewed in detail. The two co-authors sepa-
hysteroscopy and a lower rate of cervical laceration. There
rately abstracted the data for the primary and secondary
were higher rates of side effects with misoprostol, including
lMAY JOGC MAI 2006
Use of Misoprostol Before Hysteroscopy: A Systematic Review
Studies included in the meta-analysis
nausea, diarrhea, cramping, and fever. The use of
Further post hoc subgroup analyses were performed evalu-
misoprostol appears to be beneficial in premenopausal
women (Table 3), who had significant reductions in rates of
menopausal women undergoing operative hysteroscopy. As
cervical laceration and need for dilatation, and there was
only one study evaluated diagnostic hysteroscopy in
greater preprocedural cervical dilatation (weighted mean
premenopausal women,10 we did not have adequate sample
difference = 2.6; 95% CI 1.7, 3.5, P < 0.0001, random
size to comment further on this particular subgroup.
effects model) in this group. These reductions were not evi-
Among premenopausal nulliparous women, the use ofmisoprostol reduced the need for further cervical dila-
dent when postmenopausal women or those receiving
tion12,13 (RR = 0.70; 95% CI = 0.59, 0.82, P = 0.007) and the
GnRH agonists were studied (Table 4). In this group of
occurrence of cervical laceration10,12,13 (RR = 0.14;
women there was no significant difference in cervical
95% CI = 0.03,0.74, P = 0.02). The mean cervical dilatation
dilatation with the use of misoprostol (weighted mean dif-
was also greater in the misoprostol group (weighted mean
ference = 0.1; 95% CI 0.4, 0.6, P = 0.62, random effects
difference 3.36; 95% CI = 3.12, 3.59, fixed effects model).
model). For every four premenopausal women receiving
Among premenopausal women undergoing operative lapa-
misoprostol prior to hysteroscopy, one woman avoided the
roscopy, the use of misoprostol reduced the need for cervi-
need for further cervical dilatation.9 For every 12
cal dilatation11,13 (RR = 0.68; 95% CI = 0.58,80, P = 0.001)
premenopausal women receiving misoprostol, one cervical
and the occurrence of cervical laceration11,13,14 (RR = 0.22;
95% CI = 0.08, 0.60, P = 0.003), and resulted in an
MAY JOGC MAI 2006 l GYNAECOLOGY Table 1. Studies of misoprostol prior to hysteroscopy
increased mean cervical dilatation13 (weighted mean differ-
determined a priori the sample size required to detect a 33%
ence = 3.50; 95% CI = 3.21, 3.79, fixed effects model). As
reduction in the need for further cervical dilation (from
only one study presented data specific for premenopausal
50% to 33%). We found that misoprostol in premenopausal
nulliparous women undergoing operative hysteroscopy,13
women was an effective cervical ripening agent because it
we are unable to comment further on this subgroup.
reduced the need for further cervical dilatation and loweredthe rate of cervical laceration. There were higher rates of
When further subgroup analyses assessing the types of
complications in women who used misoprostol, including
hysteroscopy (operative or diagnostic) were performed for
vaginal bleeding, cramping, and elevated temperature, but
postmenopausal women or those receiving GnRH agonists,
these side effects were transient. We found subgroups of
no benefits with misoprostol were seen.
premenopausal women in whom misoprostol was of bene-fit: women undergoing operative hysteroscopy and women
DISCUSSION
who were nulliparous. This is not surprising, as operative
Studies of misoprostol suggest that it is very effective in ini-
hysteroscopy requires greater preprocedural dilation, and
tiating uterine contractions and inducing labour in the sec-
nulliparous women are more likely to have a narrow cervical
ond and third trimesters of pregnancy.6,7,25,26 It has also
been shown to be useful in cervical ripening before surgical
It is important to address the shortcomings of this
abortion, making the procedure easier to perform by
meta-analysis. A variety of protocols with different doses,
increasing cervical dilatation and ease of dilatation.5,25–30
routes, and frequencies of administration were used in the
Previous studies of misoprostol as a cervical ripening agent
studies included in the meta-analysis. The population of
before hysteroscopy found conflicting results depending on
women evaluated also varied. Some studies evaluated
the population studied. The small sample sizes of the indi-
premenopausal women,10–14 others evaluated post-
vidual studies meant that they lacked the statistical power to
demonstrate significant differences in some of the out-
agonists,15,19 and others studied a combination of these
comes evaluated, such as cervical laceration and the need
groups.18 Hysteroscopes of different sizes also were used,
and some studies evaluated misoprostol before operative
lMAY JOGC MAI 2006
Use of Misoprostol Before Hysteroscopy: A Systematic Review
Table 2. Outcomes of misoprostol prior to hysteroscopy (all women)
CI: Confidence interval. * Random effects model; ** Fixed effects model
Table 3. Outcomes of misoprostol administration prior to hysteroscopy in premenopausal women Table 4. Outcomes of misoprostol prior to hysteroscopy in postmenopausal women or those receiving GnRH agonists
CI: Confidence interval. * Fixed effects model
MAY JOGC MAI 2006 l GYNAECOLOGY
hysteroscopy and others before diagnostic hysteroscopy.
nulliparous women or those undergoing operative
Despite these heterogeneous groups, a significant differ-
hysteroscopy, because it reduces the need for further
ence was found in the primary outcome in the
mechanical cervical dilatation and reduces the rate of cervi-
premenopausal group. This meta-analysis suggests that in
cal laceration. Further research is needed to identify the
premenopausal women (and, in particular, nulliparous
ideal dose, route, and timing of misoprostol prior to the
women or those undergoing operative hysteroscopy),
procedure and to determine if misoprostol is effective in
misoprostol administration before hysteroscopy improves
cervical ripening in postmenopausal women or those
preprocedural cervical dilatation and reduces cervical lacer-
ation. Because of variations in protocols, however, we arenot able to determine the ideal dosing regimen. Other
REFERENCES
shortcomings of the studies included in this meta-analysis
1. Baggish MS. Operative hysteroscopy. In: Rock JA, Thompson JD, editors.
are also evident. The studies did not provide further details
TeLinde’s operative gynecology. Philadelphia: Lippincott – RavenPublishers;1997, p. 415–42.
on specific dilators used, or the cause of cervical lacerations(i.e., the tenaculum or the dilators). The hysteroscopies
2. Bradley LD. Complications in hysteroscopy: prevention, treatment and legal
risk. Curr Opin Obstet Gynecol 2002;14:409–15.
were performed in a variety of settings, ranging from outpa-
3. Loffer FD. Complications of hysteroscopy - their cause, prevention and
tient offices without analgesia to operating rooms with use
correction. J Am Assoc Gynecol Larparosc 1995;3:11–26.
of general anaesthesia. Studies in premenopausal women
4. Vilos GA, Vilos EC, King JH. Experience with 800 hysteroscopic
did not specify the timing of hysteroscopy in relation to the
endometrial ablations. J Am Assoc Gynecol Laparosc 1996;4:33–8.
menstrual cycle. The rate of serious complications such as
5. Goldberg AB, Carusi DA, Meckstroth KR. Misoprostol in gynecology.
uterine perforation or creation of a false passage was low
Curr Womens Health Rep 2003;3:475–83.
(1.9% in the control group) and so one would need a very
6. Alfirevic Z. Oral misoprostol for induction of labour (Cochrane review). In
large sample size (n = 2515 per group) to detect a 50%
the Cochrane Library Issue 4, 2004. Chichester, UK: John Wiley & Sons,Ltd.
reduction (2% to 1%) in this outcome. However, the need
7. Hofmeyr GJ, Gulmezoglu AM. Vaginal misoprostol for cervical ripening
for further cervical dilatation and cervical laceration may be
and induction of labour (Cochrane review). In: The Cochrane Library, Issue
4, 2004. Chichester, UK: John Wiley & Sons, Ltd.
8. Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving
the quality of meta-analyses of randomized controlled trials: the QUORUMstatement. Quality of reporting of meta-analyses. Lancet
The benefit of using misoprostol in postmenopausal
women or in those receiving GnRH agonists is less clear. In
9. Sackett DL, Richardson WS, Rosenberg W, Haynes RB. Evidence-based
this group of women, only one study suggested benefit,18
medicine – how to practice and teach EBM. New York: Churchill
and when these studies were combined in this meta-analysis
there was no evident benefit. Unfortunately, data from the
10. Ngai SW, Chan YM, Liu KL, Ho PC. Oral misoprostol for cervical priming
only study suggesting benefit were not presented in a way
in non-pregnant women. Hum Reprod 1997;12:2373–5.
that allowed incorporation as a dichotomous outcome in
11. Atay V, Duru NK, Pabuccu R, Ergun A, Tokac G, Aydin BA. Vaginal
the meta-analysis.18 It is possible that the dosing protocol of
misoprostol for cervical dilatation before operative office hysteroscopy. Gynecol Endoscopy 1997;6:47–9.
the study that suggested improvement in cervical dilatation(400 ìg by mouth, given at 24 hours and 12 hours prior to
12. Preutthipan S, Herabutya Y. A randomized controlled trial of vaginal
misoprostol for cervical priming before hysteroscopy. Obstet Gynecol
hysteroscopy) may provide the appropriate timing and dose
to allow cervical ripening in these women. The overall lack
13. Preutthipan S, Herabutya Y. Vaginal misoprostol for cervical priming before
of benefit seen in hypoestrogenic women suggests that
operative hysteroscopy: a randomized controlled trial. Obstet Gynecol
either estrogen or progesterone plays an important role in
prostaglandin-induced cervical ripening. When further sub-
14. Fernandez H, Alby JD, Tournoux C, Cheuveaud-Lambling A, DeTayrae R,
group analyses were performed (postmenopausal women
Frydman R, et al. Vaginal misoprostol for cervical ripening before operative
hysteroscopy in premenopausal women: a double-blind, placebo-controlledtrial with three dose regimes. Hum Reprod 2004; 9:1618–21.
hysteroscopy only), no subgroup of postmenopausalwomen was found to benefit, although with small sample
15. Cooper KG, Pinion SB, Bhattacharya S, Parkin DE. The effects of the
gonadotropin releasing hormone analogue (goseralin) and prostaglandin E
sizes we did not have adequate statistical power to evaluate
(misoprostol) on cervical resistance prior to transcervical resection of the
the outcomes of interest in these subgroups.
endometrium. Br J Obstet Gynaecol 1996;103:375–8.
16. Ngai SW, Chan YM, Ho PC. The use of misoprostol prior to hysteroscopy
CONCLUSION
in postmenopausal women. Hum Reprod 2001;16:1486–8.
17. Fung TM, Lam MH, Wong SF, Ho LC. A randomized placebo-controlled
Misoprostol has promise for use as a cervical ripening agent
trial of vaginal misoprostol for cervical priming before hysteroscopy in
before hysteroscopy in premenopausal women, particularly
postmenopausal women. BJOG 2002;109:561–5.
lMAY JOGC MAI 2006
Use of Misoprostol Before Hysteroscopy: A Systematic Review
18. Thomas JA, Leyland N, Durand N, Windrim RC. The use of oral
25. Goldberg AB, Greenberg MB, Darney PD. Misoprostol and pregnancy.
misoprostol as a cervical ripening agent in operative hysteroscopy:
a double-blind, placebo-controlled trial. Am J Obstet Gynecol
26. Blanchard K, Clark S, Winikoff B, Gaines G, Kaoni G, Shannon C.
Misoprostol for women’s health: a review. Obstet Gynaecol
19. Bisharah M, Al-Fozan H, Tulandi T. A randomized trial of sublingual
misoprostol for cervical priming before hysteroscopy. J Am Assoc Gynecol
27. Fong YF, Singh K, Prasad RN. A comparative study using two dose
regimens (200 ug or 400 ug) of vaginal misoprostol for pre-operative
20. Darwish A. Modified hysteroscopic myomectomy of large submucous
cervical dilatation in first trimester nulliparae. Br J Obstet Gynaecol
fibroids. Gynecol Obstet Invest 2003;56:192–6.
21. Sharma S, El-Rafaey H. The use of misoprostol as a cervical ripening agent
28. Singh K, Fong YF, Prasad RN, Dong F. Randomized trial to determine
in operative hysteroscopy. Am J Obstet Gynecol 2003;18:297–8.
optimal dose of vaginal misoprostol for preabortion cervical priming.
22. Scott P, Magos A. Vaginal misoprostol for cervical priming before operative
hysteroscopy: a randomized controlled trial. Obset Gynecol 2001;97:640–1.
29. MacIsaac L, Grossman D, Balistreri E, Darney P. A randomized controlled
23. Lichtenberg ES. Complications of osmotic dilators. Obstet Gynecol Surv
trial of laminaria, oral misoprostol, and vaginal misoprostol before abortion.
24. Darvish AM, Ahmad RM, Mohammad AM. Cervical priming prior to
30. Singh K, Fong YF, Prasad RN, Dong F. Evacuation interval after vaginal
operative hysteroscopy: a randomized comparison of laminaria versus
misoprostol for preabortion cervical priming: A randomized clinical trial.
misoprostol. Hum Reprod 2004; 19:2391–4.
MAY JOGC MAI 2006 l
Microscopic colitisChris J. J. Mulder1, Ivar M. Harkema2, Jos W. R. Meijer31 Department of Gastroenterology, Vrije Universiteit Medisch Centrum / Free University Medical Centre, Amsterdam, the Netherlands2 Department of Gastroenterology, Ziekenhuis Rijnstate / Rijnstate Hospital, Arnhem, the Netherlands3 Department of Pathology, Ziekenhuis Rijnstate / Rijnstate Hospital, Arnhem, the Netherlands
APO-SALBUTAMOL INHALER NAME OF THE MEDICINE Chemical Name: RS)-2-tert-butylamino-1-(4-hydroxy-3-hydroxymethyl-phenyl) ethanol sulfate. C13H21NO3.½ H2SO4 Structural Formula: CAS Registry Number: 51022-70-9 DESCRIPTION Salbutamol sulfate is a white or almost white powder. It is soluble in water but is only slightly soluble in alcohol, chloroform and ether. 1.2mg of s
 Use of Misoprostol Before Hysteroscopy: A Systematic Review
Studies included in the meta-analysis
Use of Misoprostol Before Hysteroscopy: A Systematic Review
Studies included in the meta-analysis