La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Diapositiva
Barbieri Antonio1, Palma Giuseppe1, Rosati Alessandra2 , Petrillo Antonella1,Di Benedetto Maria3, Longobardi Amelia3, Aldo Giudice1, Caterina Turco2, Arra Claudio1 1 Istituto Nazionale Tumori Fondazione “G.Pascale” Napoli. 2 Dipartimento di Scienze Farmaceutiche - Università degli Studi di Salerno - Fisciano 3 Dipartimento di Clinica Medica e Sperimentazione Sezione Istologica del Policlinico Università Federico II Napoli
Clinical studies indicate that stress, chronic depression, social support and other psychological
factors may influence cancer progression. Recent studies have identified biological signalling
pathways that could contribute to such effects even if the influence of the stress on some
tumors is not yet well understood. Environmental and psycho-social processes initiate a cascade
of information-processing pathways in the central nervous system (CNS) and periphery, which
subsequently trigger fight-or-flight stress responses in the autonomic nervous system (ANS), or
defeat/ withdrawal responses produced by the hypothalamic–pituitary–adrenal axis (HPA). In
the figure 1 , are reported the areas of the brain thought to be responsible for mediating
stress responses and their effects on the adrenal glands and other target tissues. HPA
responses are mediated by hypothalamic production of corticotrophin releasing factor and
arginine vasopressin, both of which activate the secretion of pituitary hormones such as
adrenocorticotropic hormone (ACTH), enkephalins and endorphins. ACTH induces downstream
release of glucocorticoids such as cortisol from the adrenal cortex. Glucocorticoids control
growth, metabolism and immune function. We show that in mice which undergo to stress
condition of restraint one week before tumor injection of B16-F10 murine melanoma cell line, the
tumor burden increases of 200% respect to control group, and 120% in mice treated with
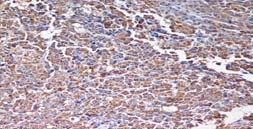
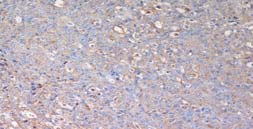
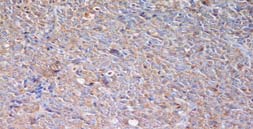
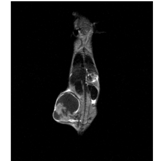
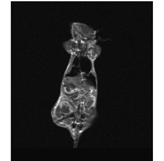
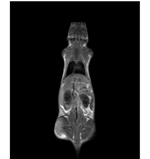
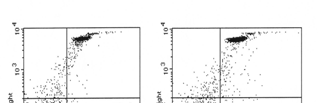
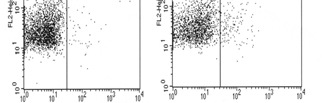
Figure 1 : Effects of stress-associated factros on the tumor microenvironment. Measure of ACTH and glucose level Figure 2: Measure of glucose and ACTH levels in different groups of treatment. Figure 3: FACs analisys of timocyte with annexin V and iodure propidie. On the rihgt the control mice and on the left the stressed mice. tumor growth C57BL/6 Figure 4: B16 cells IHC with anti-VEGF at 20x, a) Control, b) Placebo+daily stress, c) (m e m 1000 Propanolol+daily stress days post tumor injection Figure 6: Tumor Growth of B16F10 cell line Figure 5: A) Western Blot analysis of Figure 7: Magnetic resonance imaging (MRI). Melanoma B16 coronal expression of VEGF in B16F10 cell line. planes image T1-weighted (400/13) enhanced Gd-DTPA. a) Image B) Western Blot analysis of eNOS level with central tumor necrosis of the posterior right leg; b) Image of expression in B16F10 cell line. the tumor treated with stress + propranolol; c) Image of tumor treated with stress that present a significative central necrosis respect to other groups.
These data suggest that the stress influences the tumor progression and growth by activaction of β adrenergic
receptor and increases glucorticoids levels that induce a upregulation of VEGF and increase of eNOS levels. High
levels of eNOS induce expression of iNOS that produces an increase in VEGF expression and thymic atrophy by
induction of apoptosis of T cells. These finding suggest that the stress influences also tumors not “strictly”
hormone–dependent as melanoma. These mechanisms activated by the stress, help to understand new pathway
involved in tumor progression and could represent new strategies for protecting individuals with cancer from the
detrimental effects of stress biology on the progression of malignant disease. Our next goal is to discover new
drugs by double action in order to block tumor progression induced by stress, without somministration of more
drugs to the patient that could be dangerous in the time.
Florida Gulf Coast Ear, Nose & Throat, LLC PATIENT NAME:____________________________________________________________________ Last Date of Birth:______________ Age: ______ Sex: M - F Marital Status: S M D W SEP Name of Spouse / Parent if Patient is a Minor_______________________________________________________ Social Security#:_______________________ Email Address:_______________________
Editorials Evidence based medicine: what it is and what it isn't It's about integrating individual clinical expertise and the best external evidence Evidence based medicine, whose philosophical origins extend back to mid-19th century Paris and earlier, remains a hot topic for clinicians, public health practitioners, purchasers, planners, and the public. There are now frequent workshops in





 Barbieri Antonio1, Palma Giuseppe1, Rosati Alessandra2 , Petrillo Antonella1,Di Benedetto
Barbieri Antonio1, Palma Giuseppe1, Rosati Alessandra2 , Petrillo Antonella1,Di Benedetto