La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Ilsensodellamedicina.it
DIAGNOSTIC TRACKS AND TRICKS FOR SEIZURES: DIAGNOSIS AND CLASSIFICATION Tracey A. Milligan, MD, MS Introduction Epileptic seizures are a common medical problem. Ten percent of the population will have one seizure and the cumulative lifetime incidence of epilepsy is 3 percent.1 In the United States, approximately 2.5 million people have epilepsy. Epilepsy affects people of every background and age and is associated with impaired quality of life and an increased mortality rate of 2-3 times higher than the general population. In addition, epilepsy, as well as its treatment, can have serious consequences and over one half of all patients with epilepsy continue to experience at least occasional seizures despite treatment.2 Optimal diagnosis and classification of seizures can reduce the risk of morbidity and mortality and greatly improve the quality of life. Optimal diagnosis of epilepsy is one of the most frequent and greatest challenges facing neurologists. In the most recent National Disease and Therapeutic Index, convulsions and epilepsy together were the leading diagnoses treated by neurologists.3 An added complexity for the diagnosis of seizures is that it is rare that the event is actually witnessed by the neurologist (unlike movement disorders for example) and other than a video-EEG showing a definite clinical-electrical event, there is no gold standard diagnostic test. Even our most frequently used diagnostic test of EEG, can result in misdiagnosis (summarized in a recent Neurology supplement).4 Failure to diagnose epilepsy can have significant consequences as seizures can be life threatening. Misdiagnosis of epilepsy can leave the underlying etiology untreated with potentially fatal consequences and result in a reduced quality of life from patient distress, unnecessary driving restrictions, employment difficulties and the unnecessary use of antiepileptic drugs (AEDs) with their inherent immediate and long term side effects. The following tips, presented as frequently asked questions, emphasize some of important considerations when seeing a patient complaining of a seizure or seizure-like event. Reference is also made to current AAN Practice Parameters: Evaluating an Apparent Unprovoked First Seizure in Adults5, Reassessment: Neuroimaging in the Emergency Patient Presenting with Seizure6, Use of Serum Prolactin in Diagnosing Epileptic Seizures7, and to the 3 Epilepsy Quality Measures approved January 2012 by the Centers for Medicare and Medicaid Services (CMS) with required reporting anticipated to start in 2014. Eight measures were approved by the workgroup,8 but only 3 were adopted by CMS: 1)
Frequency of each seizure type should be reported at each visit
The etiology (or epilepsy syndrome) should be reported at each visit
Counseling for women of child bearing potential with epilepsy should be provided annually
FAQs 1. Was it a seizure? Patients may present for evaluation of “seizures” or have been diagnosed in the emergency room with a “seizure” and sometimes already are taking an AED. However, no matter how or when the diagnosis of seizure was made, the first question should be “Was it a seizure?” A thorough and complete history from the patient and eye- witnesses is one of the strongest diagnostic tools (Level B evidence),9 with the caveat that eye-witness reports can be misleading and/or inaccurate.10,11 An excellent “Tips for Seizure Observation and Recording” is provided by the American Epilepsy Society. 12 A seizure is defined as a temporary alteration in brain function due to abnormal excessive or synchronous neuronal activity. However, occasionally non-neurologists will label other events with altered consciousness and/or bodily shaking as a seizure. Additionally, other paroxysmal events may not be considered as consistent with seizures. A common educational tip given to non-neurologists is: Not all seizures shake and not all shakes are seizures. Some of the most common mimickers of seizures in adults are psychogenic events and episodes of reduced cerebral perfusion (Tables 1 and 2).
2013 The American Academy of Neurology Institute.
Table 1 Clinical distinction of psychogenic nonepileptic seizures (PNES) from tonic-clonic epileptic seizures (ES) Clinical Feature
May stop and stop, pelvic thrusting, back arching,
erratic movements and absence of stereotypy
Syncope commonly results in myoclonic movements that can mimic seizures,13 referred to as “syncopal convulsions.” Electroencephalograms done during even the most dramatic convulsive movements, do not show seizure activity and rather show slowing or minimal cerebral activity. Table 2 Features that distinguish syncope versus seizure Clinical Feature
2013 The American Academy of Neurology Institute.
Table 3 Nonepileptic disorders that can be mistaken for epileptic seizures in adults
Syncope (vasovagal/neurocardiogenic, decreased cardiac output, volume depletion, arrhythmia)
Migraine (classic, basilar, confusional, acephalgic)
Cerebrovascular (transient ischemic attack, amyloid angiopathy)
Sleep disorders (REM behavior disorder, narcolepsy, parasomnias)
Movement disorders (tics, nonepileptic myoclonus, tremor)
Psychiatric (panic, dissociation, conversion, malingering)
Syncope (vasovagal/neurocardiogenic, decreased cardiac output, volume depletion, arrhythmia)
Migraine (classic, basilar, confusional, acephalgic)
Cerebrovascular (transient ischemic attack, amyloid angiopathy)
2. Was the seizure provoked? Seizures are commonly provoked. Although determination of a provoking factor may not change the initial work- up, it will significantly impact patient counseling and management. Medications are a common source of provoked seizures, either directly or by leading to metabolic changes such as hyponatremia or hypoglycemia. Illicit drug use and alcohol can lead to provoked seizures as well (Table 4). More comprehensive lists of medications that can provoke seizures are easily available. 14 Table 4: Some causes of provoked seizures Metabolic
Stimulants (amphetamines, cocaine, ecstasy,
baclofen, benzodiazepines, barbiturates, diphenhydramine)
Acute neurologic injury can lead to provoked seizures, which may require short term treatment with an AED, but do not necessarily lead to epilepsy (e.g., head injury, acute stroke, encephalitis). The search for provoking factors is also an important component in persons with epilepsy. These factors include: AED nonadhearance, lack of adequate sleep, hormonal changes in women, non-neurologic infections, and stress. 3. Does the patient have epilepsy? Epilepsy is defined as the tendency to have recurrent unprovoked seizures. Historically, the operational definition has been having 2 or more unprovoked seizures. An alternative and controversial definition requiring only 1 seizure proposed by the International League Against Epilepsy (ILAE) is: a disorder of the brain characterized by an enduring predisposition to generate epileptic seizures and by the neurobiologic, cognitive, psychological and
2013 The American Academy of Neurology Institute.
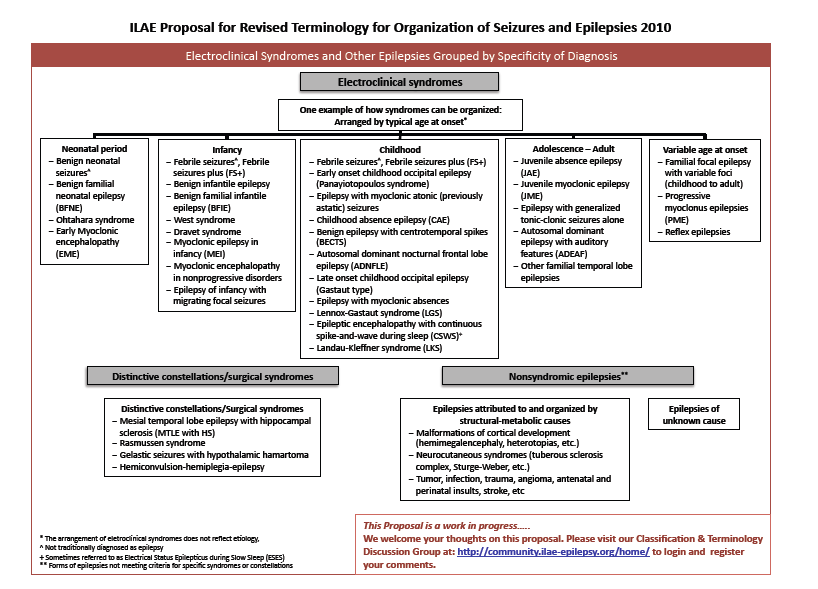
social consequences of this condition.15 This definition has utility in guiding management and recognizing the risk of seizures in those individuals, similar to how risk of stroke is managed in individuals with transient ischemic attacks or cerebrovascular disease. But the diagnosis of epilepsy has wider implications for the patient including social stigma, job disqualifications, and life insurance and thus in some ways is a higher stakes diagnosis. A detailed history after a recognized single seizure, can often lead to the diagnosis of epilepsy. A clearly recognized seizure after an aura that has occurred in the past in isolation, screening for myoclonic seizures or other events which in retrospect were seizures can lead to the diagnosis of epilepsy. 4. How do I classify the epilepsy? The classification of epilepsy is the domain of the neurologist and leads to determination of the appropriate track in diagnostic testing, treatment, prognosis and patient counseling. The classification of epilepsy, like other diseases in neurology, is changing with the growing scientific knowledge, particularly in the field of genetics. The ILAE currently has an evolving classification schemes for epilepsy. The first classification system, developed in 1981 ,16 divides seizures in to three types, with subtypes of each: partial (focal seizures involving only part of the brain), generalized (seizures involving both hemispheres in the brain), and unclassifiable. This system allowed for simple classification that helped determine diagnostic evaluation, the choice of medication, and prognosis. A supplement to this system of classification was developed in 1989- the ILAE Classification of Epilepsies and Epileptic Syndromes. 17 Epilepsies were divided into four groups: localization-related (involves one or more focal areas of the brain), generalized (involves both hemispheres of the brain at the same time), undetermined, and special syndromes. Within the localized and generalized groups, there are further subdivisions into idiopathic (no identifiable cause), symptomatic (identified or suspected cause), or cryptogenic (a suspected cause that cannot be definitively identified). In 2010, the ILAE proposed a new classification system with new, alternative concepts and terminology. 18 Originally a 5 axis description was proposed (Axis 1:ictal phenomenology, axis 2: seizure type, axis 3: syndrome-when known, axis 4: genetic defect or specific pathological substrate for symptomatic focal epilepsies, and axis 5: impairment classification). More recently, the changes were summarized in the table on the next page. 19 The most recent classification system in part stresses the importance of seizure description. A glossary of terminology is easily available. 20 The implications of the newest proposal include an increased use of the following terms: focal, localization- related, networks limited to one hemisphere versus rapidly engaging bilaterally distributed networks, neocortical or hippocampal, genetic cause, structural metabolic cause, unknown cause.
2013 The American Academy of Neurology Institute.
5. How helpful and necessary is diagnostic testing? The following tests are often used in patients who have had a possible seizure: laboratory testing, EEG, and neuroimaging. In general, studies have shown a low yield of laboratory diagnostic testing, unless otherwise suggested by history or examination. Leukocytosis and metabolic acidosis can be seen after a seizure, but tend to be quite transient. After a convulsion, a raised CPK to a level that requires intervention can be seen. The American College of Emergency Physicians recommends testing levels of sodium, glucose and pregnancy testing in women of childbearing age. 21 Calcium testing in patients with malignancy is also advised. Other laboratory tests are frequently performed as they can reveal information which helps with etiology and changes in management; these tests include: electrolytes, renal function, liver function, toxicology screening. Prolactin testing done correctly can help distinguish PNES from ES, but is not reliable in distinguishing between ES and other causes of loss of consciousness such as syncope. The AAN Practice Parameter states: Elevated serum prolactin assay, when measured within 20 minutes after a suspected event, is a useful adjunct for the differentiation of GTC or CPS from PNES among adults and older children (Level B). 7 There is variation in the protocols used in the studies reviewed for this Practice Parameter, but a possible protocol within these guidelines is: 1) Measure prolactin level after possible CPS/GTC versus PNES event within 10-20 minutes; 2) Measure another level after the patient has been event free for at least 6 hours (baseline level); 3) Consider a positive elevation of prolactin if it is 2X baseline level. This degree of prolactin elevation has a positive predictive value for ES. There is a low sensitivity (47-58.2%) and high specificity (89.9-95.7%) for ES. Lumbar puncture may be helpful in patients with immunosuppression or fever (Level U). 5 It can be considered in other instances, although it is generally not performed without suspicion of an acute neurologic process.
2013 The American Academy of Neurology Institute.
EEG should be performed in every patient with a suspected seizure or epilepsy. The AAN Practice Parameter is worded less strongly and states that after a first seizure an EEG should be considered as part of the routine neurodiagnostic evaluation (Level B). 5 Although only approximately 40% of patients with epilepsy will have an abnormal routine EEG ,22 the implications are significant. An EEG may be diagnostic and lead to further information about the type of epilepsy and syndrome that lead to a change in management (focal vs. primary generalized, absence, JME) (Level C). 5 EEG can also assist in the diagnosis of the etiology of seizures or epilepsy syndrome (e.g., CJD, HSV, SSPE, BRE, Absence). The EEG results can also guide further testing and review of neuroimaging. EEG can occasionally capture the event and assist in the diagnosis of alternative etiologies. EEG is helpful in assessing the risk of seizure recurrence after a first unprovoked seizure (Level B) as the risk of a second seizure within 2 years is 55% in patients with an abnormal EEG versus 10% if the EEG was normal. A longer EEG recording in patients with epilepsy may increase the sensitivity to 90% 23 and an EEG done within 24 hours of the seizure also has a higher yield for epileptiform discharges (51% vs. 34%) King 98. Sleep deprivation can also increase the yield of obtaining epileptiform discharges. 24 Ambulatory EEG monitoring has a modestly increased yield over routine EEG (34% versus 24%) and a greater likelihood of capturing an event (15%). 25 EEG sensitivity and specificity is related to the skills of the interpreter and striving towards specificity rather than sensitivity yields a more accurate prediction. 26 Video-EEG monitoring is indicated when diagnosis is unclear, the patient fails to respond to treatment, and when full characterization of seizures is required for other reasons. Neuroimaging is indicated in all adults presenting with a seizure. AAN Practice Guidelines state that brain imaging using CT or MRI should be considered as part of the neurodiagnostic evaluation of adults presenting with an apparent unprovoked first seizure (Level B). 5 MRI is the preferred neuroimaging modality and has a yield of approximately 10%. The type of MRI and review of the MRI results are best determined and performed by the patient’s neurologist in consultation with a neuroradiologist. Neuroimaging can identify structural abnormalities that cause certain epilepsies and lead to a high risk of recurrence. It is not indicated routinely when a diagnosis of idiopathic generalized epilepsy has been made, 9 however should be considered when seizures continue in spite of appropriate AED therapy. Concluding Remarks The correct diagnosis of seizure and type of epilepsy is the foundation for excellent neurologic care in this patient population. Diagnosis is best accomplished by history including that of the event and predisposing conditions, examination, diagnostic testing including EEG and MRI. Even after a thoughtful and thorough diagnosis, reconsideration is indicated when the patient does not respond to initial management. Referral to an epilepsy center is indicated for all patients who do not have their seizures fully controlled without adverse side effects. References: 1. Hauser WA, Annegers JF, Kurland LT. Incidence of epilepsy and unprovoked seizures in Rochester,
Minnesota: 1935-1984. Epilepsia 1993;34:453-68.
2. Collaborative Group for the Study of Epilepsy. Prognosis of epilepsy in newly referred patients. A multicenter
prospective study of the effects of monotherapy on the long-term course of epilepsy. Epilepsia 1992; 33:45-51.
3. IMS Health Incorporated. Web. 2 Feb. 2013.
https://web01.imshealth.com/ndti/SpecialityProfiles/Neurology.pdf
4. Tatum WO. How not to read an EEG: Introductory statements. Neurology 2013; 80:S1-S3.
5. Krumholz A, Wiebe S, Gronseth G, et al. Practice parameter: evaluating an apparent unprovoked first seizure
in adults (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology 2007; 69: 1996-2007.
6. Harden CL, Huff JS, Schwartz TH, et al. Reassessment: Neuroimaging in the emergency patient presenting
with seizure (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2007; 69: 1772-1780.
2013 The American Academy of Neurology Institute.
7. Chen DK, So, YT, Fisher RS. Use of serum prolactin in diagnosing epileptic seizures: Report of the
Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology. Neurology 2005; 65:668-675.
8. American Academy of Neurology. Web. 2 Feb. 2013 < http://www.aan.com/globals/axon/assets/9079.pdf >
9. National Collaborating Centre for Primary Care. The diagnosis and management of the epilepsies in adults
and children in primary and secondary care. London (UK): Royal College of General Practitioners; 2004 Oct.
10. Mannan JB, Wieshmann UC. How accurate are witness descriptions of epileptic seizures? Seizure 2003;
11. Rugg-Gunn FJ, Harrison NA, Duncan JS. Evaluation of the accuracy of seizure descriptions by the relatives
of patients with epilepsy. Epilepsy Res 2001; 43:193-199.
12. American Epilepsy Society. Web. 2 Feb. 2013.
http://www.aesnet.org/files/dmfile/tips_seizure_observation_recording3.pdf
13. Lempert T, Bauer M, Schmidt D. Syncope: A videometric analysis of 56 episodes of transient cerebral
14. American Epilepsy Society. Web. 2 Feb 2013.
http://www.aesnet.org/files/dmfile/drugsthatcancauseseizuresup72009.pdf
15. Fisher RS, van Emde Boas W, Blume W, Elger C, Genton P, Lee P, et al. Epileptic seizures and epilepsy:
definitions proposed by the International League Against Epilepsy ILAE and the International Bureau for Epilepsy (IBE). Epilepsia 2005: 46:470-472.
16. William O. Tatu Commission on Classification and Terminology of the International League Against Epilepsy.
Proposal for revised clinical and electroencephalographic classification of epileptic seizures. Epilepsia 1981; 22:489-501.
17. Commission on Classification and Terminology of the International League Against Epilepsy. Proposal for
revised classification of epilepsies and epileptic syndromes. Epilepsia 1989; 30:389-399.
18. Berg AT, Berkovic, SF, Brodie MJ, Buchhalter, J, Cross JH, Van Emde Boas,W, Engel J, French J, Glauser
TA., Mathern GW, Moshé SL, Nordli,D, Plouin P Scheffer I E. Revised terminology and concepts for organization of seizures and epilepsies: Report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia 2010, 51: 676–685.
19. International League Against Epilepsy. Web. 2 Feb. 2013
http://www.ilae.org/Visitors/Centre/ctf/ctfoverview.cfm
20. International League Against Epilepsy. Web. 2 Feb. 2013
http://www.ilae.org/Visitors/Centre/ctf/glossary.cfm#intro
21. American College of Emergency Physicians. Clinical policy: critical issues in the evaluation and management
of adult patients presenting to the emergency department with seizures. Ann Emerg Med. 2004;43:605-25.
22. Salinsky M, Kanter R, Dasheiff RM. Effectiveness of multiple EEGs in supporting the diagnosis of epilepsy:An
operational curve. Epilepsia 1987; 28(4):331-34.
23. So E, Ruggles K, Ahmann P. Yield of Sphenoidal Recordings in Sleep-Deprived Outpatients. J Clin
24. King MA, Newton MR, Jackson GD, et al. Epileptology of the first-seizure presentation: a clinical, EEG and
MRI study of 300 consecutive patients. Lancet 1998;352:1007–11.
2013 The American Academy of Neurology Institute.
25. Liporace J, Tatum W 4th, Morris GL 3rd. Clinical utility of sleep-deprived versus computer-assisted
ambulatory 16-channel EEG in epilepsy patients: a multicenter study. Epilepsy Res. Nov 1998;32(3):357-62.
26. Gilbert DL, Sethuraman G, Kotagal U, Buncher CR. Meta-analysis of EEG test performance shows wide
variation among studies. Neurology 2003;60:564-570.
2013 The American Academy of Neurology Institute.
Hong Kong Exchanges and Clearing Limited and The Stock Exchange of Hong KongLimited take no responsibility for the contents of this announcement, make no representationas to its accuracy or completeness and expressly disclaim any liability whatsoever for anyloss howsoever arising from or in reliance upon the whole or any part of the contents of thisannouncement. (incorporated in the Cayman Island
P R E V E N Z I O N E D E L L A S E R V I Z I O S A N I T A R I O N A Z I O N A L E D I F F U S I O N E D E L L E P.O. 7 Rev . 00 Azienda Sanitaria Locale 3 I N F E Z I O N I D A M R S I N Cso. Svizzera, 164 – 10149 TORINO – Tel. 011/4393111 P A Z I E N T I S O T T O P O S T I A D Pag. 1 di Pag . 5 I M P I A N T O D I P A C E – M A K E R UOa CARDIOLOGIA
 5. How helpful and necessary is diagnostic testing?
5. How helpful and necessary is diagnostic testing?