La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Hepatitiscentral.net2
A Simple Noninvasive Index Can Predict Both
Significant Fibrosis and Cirrhosis in Patients With
Chun-Tao Wai,1 Joel K. Greenson,2 Robert J. Fontana,1 John D. Kalbfleisch,3 Jorge A. Marrero,1
Hari S. Conjeevaram,1 and Anna S.-F. Lok1
Information on the stage of liver fibrosis is essential in managing chronic hepatitis C (CHC) patients. However, most models for predicting liver fibrosis are complicated and separate formulas are needed to predict significant fibrosis and cirrhosis. The aim of our study was to construct one simple model consisting of routine laboratory data to predict both significant fibrosis and cirrhosis among patients with CHC. Consecutive treatment-naive CHC patients who underwent liver biopsy over a 25-month period were divided into 2 sequential cohorts: training set (n ؍ 192) and validation set (n ؍ 78). The best model for predicting both significant fibrosis (Ishak score > 3) and cirrhosis in the training set included platelets, aspartate aminotransferase (AST), and alkaline phosphatase with an area under ROC curves (AUC) of 0.82 and 0.92, respectively. A novel index, AST to platelet ratio index (APRI), was developed to amplify the opposing effects of liver fibrosis on AST and platelet count. The AUC of APRI for predicting significant fibrosis and cirrhosis were 0.80 and 0.89, respec- tively, in the training set. Using optimized cut-off values, significant fibrosis could be predicted accurately in 51% and cirrhosis in 81% of patients. The AUC of APRI for pre- dicting significant fibrosis and cirrhosis in the validation set were 0.88 and 0.94, respectively. In conclusion, our study showed that a simple index using readily available laboratory results can identify CHC patients with significant fibrosis and cirrhosis with a high degree of accuracy. Application of this index may decrease the need for staging liver biopsy specimens among CHC patients. (HEPATOLOGY 2003;38:518-526.)
Histologicexaminationoftheliverisanintegral treatmentpossiblycouldbedelayedorwithheld.Onthe
part of the evaluation of patients with chronic
other hand, patients with significant fibrosis (i.e., septal or
hepatitis C (CHC).1,2 Knowledge of the stage of
bridging fibrosis) progress almost invariably to cirrhosis
liver fibrosis is essential for prognostication and decisions
over a 10- to 20- year period so antiviral treatment should
on antiviral treatment.3,4 CHC patients with no or min-
be strongly considered.5 For patients with cirrhosis, sur-
imal fibrosis at presentation appear to progress slowly and
veillance for hepatocellular carcinoma and gastroesopha-geal varices should be considered also.6,7
Liver biopsy is currently the gold standard in assessing
Abbreviations: CHC, chronic hepatitis C; AST, aspartate aminotransferase;
liver histology. Although percutaneous liver biopsy is in gen-
ALT, alanine aminotransferase; HCV, hepatitis C virus; IDU, injection drug use;
eral a safe procedure, it is costly and does carry a small risk for
ALP, alkaline phosphatase; ULN, upper limit of normal; ROC, receiver operatingcharacteristics; AUC, area under receiver operating curves; CI, confidence interval;
complication.8 In addition, there could be sampling error
APRI, aspartate aminotransferase to platelet count ratio index.
because only 1/50,000 of the organ is sampled. Furthermore,
From the 1Division of Gastroenterology, 2Department of Pathology, 3Department
inter- and intraobserver discrepancies of 10% to 20% in
of Biostatistics, University of Michigan Medical School, Ann Arbor, MI.Received March 11, 2003, accepted May 20, 2003.
assessing hepatic fibrosis have been reported, which may lead
Supported by the Singapore HMDP Fellowship (C.T.W.) and by National In-
to understaging of cirrhosis.9-11 Hence, there is a need to
stitutes of Health contract N01-DK-9-2323, and grants U01-DK-57577, U01-
develop accurate and reliable noninvasive means to assess the
DK-62498, and R43-AI-51919 (A.S.-F.L.).Address reprint requests to: Anna S.-F. Lok, M.D., Division of Gastroenterology,University of Michigan Medical Center, 3912 Taubman Center, Box 0362, Ann
Noninvasive approaches to assess histology in CHC
Arbor, MI 48109-0362. E-mail: aslok@umich.edu; fax: 734-936-7392.
patients include clinical symptoms and signs, routine lab-
Copyright 2003 by the American Association for the Study of Liver Diseases. 0270-9139/03/3802-0030$30.00/0
oratory tests, serum markers of fibrosis and inflammation,
quantitative assays of liver function, and radiologic imag-
ing studies.12-15 However, at present, none of these tests or
Patients were divided into 2 sets: consecutive patients
markers alone is accurate or reliable in predicting histol-
who were biopsied between January 2001 and July 2002
ogy, in particular, liver fibrosis. An ideal noninvasive di-
constituted the training set, whereas those patients who
agnostic test for hepatic fibrosis should be simple, readily
were biopsied between August 2002 and January 2003
available, inexpensive, and accurate.16 An index compris-
constituted the validation set. All study subjects gave in-
ing routinely available laboratory tests would meet these
formed consent for the liver biopsy. This study was ap-
proved by the Institutional Review Board.
Many studies have been performed to evaluate the use
Methods. A list of consecutive CHC patients who un-
of readily available laboratory test results to predict signif-
derwent percutaneous liver biopsy at the University of
icant fibrosis or cirrhosis in patients with CHC.17-21
Michigan Medical Center was generated from the De-
However, sensitivity was generally poor, and most studies
partment of Pathology. Clinical information about these
did not validate their results in a separate group of pa-
patients obtained from electronic medical record and
tients. A recent study by Forns et al.21 performed internal
hard-copy clinical charts were reviewed by one investiga-
validation using a randomly chosen cohort from the study
tor (C.T.W.) to assess eligibility for the study. Demo-
patients and found that absence of significant fibrosis
graphics and laboratory variables were recorded. Other
could be predicted in 39% of patients. However, only
clinical variables were extracted from the medical records
24% of their patients had significant fibrosis so it is un-
according to a set of predetermined criteria.
certain if the results could be extrapolated to patients with
Patients on diabetic medications or patients who had a
past history of diabetes mellitus were considered to have
For the prediction of cirrhosis, most studies examined
diabetes mellitus. Patients who had been drinking more
the usefulness of predetermined formulas such as aspar-
than an average of 7 drinks per week, for more than 4
tate aminotransferase (AST)/alanine aminotransferase
weeks in a row before the liver biopsy, were considered
(ALT) ratio or the cirrhosis discriminant score, without
current drinkers. Patients who drank less than 7 drinks
analyzing other confounding factors or validating their
per week for the past 4 weeks in a row were considered
results.22-26 Kaul et al.27 performed univariate and multi-
nondrinkers. Patients who had stopped drinking com-
variate analysis on 351 patients and derived a model con-
pletely for more than 1 year before the biopsy were con-
sisting of gender, AST, platelet count, and spider nevi.
sidered ex-drinkers. Patients with no explicitly mentioned
This model was validated internally and externally with
amount or duration of drinking were considered to have
good accuracy but it included one subjective variable.
We aimed to develop one single model consisting of
Patients with a history of blood transfusion before
readily available, objective laboratory data to predict both
1992 were considered to have acquired CHC through
significant fibrosis and cirrhosis in treatment-naive CHC
transfusion.28,29 For those with multiple transfusions,
patients. To accomplish this, a training set of clinical and
the date of the first transfusion was considered to be the
laboratory data from 192 consecutive CHC patients were
time of infection. Patients with a history of injection
used to formulate predictive models, which were vali-
drug use (IDU) were considered to have acquired CHC
through IDU and the year in which IDU began wasconsidered to be the time of infection. Patients with no
Patients and Methods
history of transfusion or IDU, but who had othermodes of percutaneous exposure such as a tattoo, oc-
Patients. This retrospective cohort study included
cupational exposure, and so forth, were considered to
579 consecutive adult patients with CHC who had un-
have acquired CHC through others means and the year
dergone percutaneous liver biopsy at the University of
of first percutaneous exposure was considered as the
Michigan Medical Center from January 2001 to January
time of infection. Patients without parenteral risk fac-
2003. The diagnosis of CHC was established by the pres-
tors were considered to be unknown regarding both the
ence of hepatitis C virus (HCV) RNA using polymerase
chain reaction assays. Patients with the following condi-
Except for HCV genotype, only laboratory results per-
tions were excluded from the study: presence of other
formed within 4 months from the date of the liver biopsy
causes of liver disease, hepatocellular carcinoma, prior
were used for this study. If more than one set of laboratory
liver transplantation, prior interferon therapy, immuno-
test results were available, the results closest to the time of
suppressive therapy, insufficient liver tissue for staging of
biopsy were used. Results of serum aminotransferase and
fibrosis, and incomplete data on complete blood counts
alkaline phosphatase (ALP) levels were expressed as ratios
of the upper limit of normal (ULN). HCV-RNA level was
expressed as log10 IU/mL. Abdominal ultrasound reports
Table 1. Comparison of Patients in the Training
within 6 months from the time of biopsy were reviewed. and Validation Sets
Patients with splenomegaly, enlarged spleen, or spleen
Training Set Validation Set
size of more than 14 cm were considered to have spleno-
Variable P Value
Histologic slides of all eligible patients were retrieved.
All liver biopsies were reviewed by one pathologist
(J.K.G.), who had no knowledge of the clinical character-
istics of the study subjects. Hepatic fibrosis was assessed
using the Ishak fibrosis score.31 Significant fibrosis was
defined as Ishak score of 3 or more (presence of bridging
fibrosis) and cirrhosis as Ishak score of 5 or 6. Statistical Analysis. Data were expressed as mean Ϯ
SEM unless otherwise stated. Statistical analysis was
performed by SPSS software version 9.0 (SPSS Inc.,
Chicago, IL). There were 2 endpoints in this study:
presence of significant fibrosis and cirrhosis. The fol-
lowing variables were included in the univariate analy-
sis: demographics (age, sex, ethnicity), alcohol intake,
viral factors (mode of HCV infection, age at infection,
duration of infection, HCV-RNA level, genotype), and
other test results (white cell count, platelet count, in-
ternational normalized ratio, bilirubin, albumin, ALT,
AST, and ALP). All continuous variables were analyzed
after logarithmic transformation for normality of dis-
tribution. Categoric variables were compared by 2 or
Fisher exact tests, whereas continuous variables were
compared with the Student’s t test. Correlation was
evaluated by the Spearman correlation coefficient. A
2-sided P value of less than .05 was considered statisti-
NOTE. Values are expressed as mean Ϯ SEM.
For the formulation of predictive models, univariate
analysis was performed on variables between patients withand without the study endpoints in the training set. Sig-
Characteristics of the Patients in the Training Set.
nificant variables from the univariate analysis (P Ͻ .05),
From January 2001 to July 2002, 428 percutaneous liver
together with age at biopsy, were then subjected to mul-
biopsies were performed on patients with CHC at our
tivariate analysis by forward logistic regression to identify
institution. A total of 236 patients were excluded from the
independent factors associated with either endpoint.
study: 102 had prior interferon therapy, 82 had prior liver
Variables with missing values in more than 20% of the
transplants, 23 had concomitant liver diseases, 9 were on
patients (i.e., splenomegaly on ultrasonography, body
immunosuppressive therapy, 4 had insufficient liver tis-
mass index, age at infection, and duration of infection)
sues for staging of fibrosis, and 16 had incomplete data on
were not included in the regression analysis.
complete blood count and/or liver panel.
Formulas with risk scores that could best predict the
The mean age of the 192 patients included in the train-
study endpoints (significant fibrosis and cirrhosis) were
ing set was 46.8 Ϯ 0.6 years, 123 (64%) were men, 151
constructed by entering different sets of independent vari-
(79%) were Caucasians, and 16 (8%) were African Amer-
ables into the regression model. The diagnostic value of
icans. Thirteen (7%) patients had diabetes mellitus (Ta-
each formula was assessed by the area under the receiver
ble 1). The age at infection and duration of infection,
operating characteristic (ROC) curves.
available in 65% of the patients, were 21.1 Ϯ 0.7 years
The best model derived from the training set then was
and 26.7 Ϯ 0.7 years, respectively. Of the 98 patients who
applied to the validation set to test for accuracy by mea-
had ultrasound results, 18 (18%) had splenomegaly. The
suring the areas under the ROC curves.
mean Ishak fibrosis score was 2.83 Ϯ 0.10. Ninety-one
Table 2. Univariate Analysis of Variables Associated With the Presence of Significant Fibrosis and Cirrhosis in the Training Set No Significant Fibrosis Significant Fibrosis No Cirrhosis Cirrhosis Ishak Score 0-2 Ishak Score 3-6 Ishak score 0-4 Ishak Score 5-6 Variable (n ؍ 101) P Value (n ؍ 164) P Value
(47%) patients had significant fibrosis and 28 (15%) had
Regression formula for prediction of significant fibrosis:
Predictors of Significant Fibrosis and Cirrhosis From the Training Set. Variables associated with the
presence of significant fibrosis and cirrhosis were first as-
Ϫ 0.375⅐ln (platelet count [109/L]).
sessed by univariate analysis (Table 2). Subsequent mul-tivariate analysis showed that platelet count (P Ͻ .001),
Regression formula for prediction of cirrhosis:
AST level (P Ͻ .001), and ALP level (P ϭ .029) were theindependent predictors of significant fibrosis whereas
platelet count (P Ͻ .001), AST level (P ϭ .017), white cell
count (P ϭ .01), ALP level (P ϭ .019), and AST/ALT
Ϫ 0.436⅐ln (platelet count [109/L]).
ratio (P ϭ .001) were the independent predictors of cir-rhosis.
Although both histologic endpoints could be predicted by
Variables in the best models for prediction of signifi-
the same variables, 2 separate formulas were required and
cant fibrosis included platelet count, AST levels, and ALP
levels, and for prediction of cirrhosis platelet count, white
Validation Set. From August 2002 to January 2003,
cell count, AST level, ALP level, and AST/ALT ratio (Ta-
151 liver biopsies were performed on adult patients with
ble 3). Models with only platelet count and AST level
CHC. Seventy-three patients were excluded from the
were more simple and had accuracies comparable with
study: 39 had prior interferon therapy, 23 had prior liver
those with 3 or more variables in prediction of both end-
transplant, 5 had concomitant liver diseases, 2 were on
immunosuppressive therapy, and 4 had incomplete re-
Table 3. Models With Different Combination of Variables for Predicting Significant Fibrosis and Cirrhosis in the Training Set and the Validation Set Training Set Validation Set Prediction of Prediction of Significant Fibrosis Prediction of Cirrhosis Significant Fibrosis Prediction of Cirrhosis Variables in the Model AUC (95% CI) AUC (95% CI) AUC (95% CI) AUC (95% CI)
NOTE. NA, not applicable because not all the variables were significant in the regression model.
sults on blood count or liver panel. Seventy-eight patients
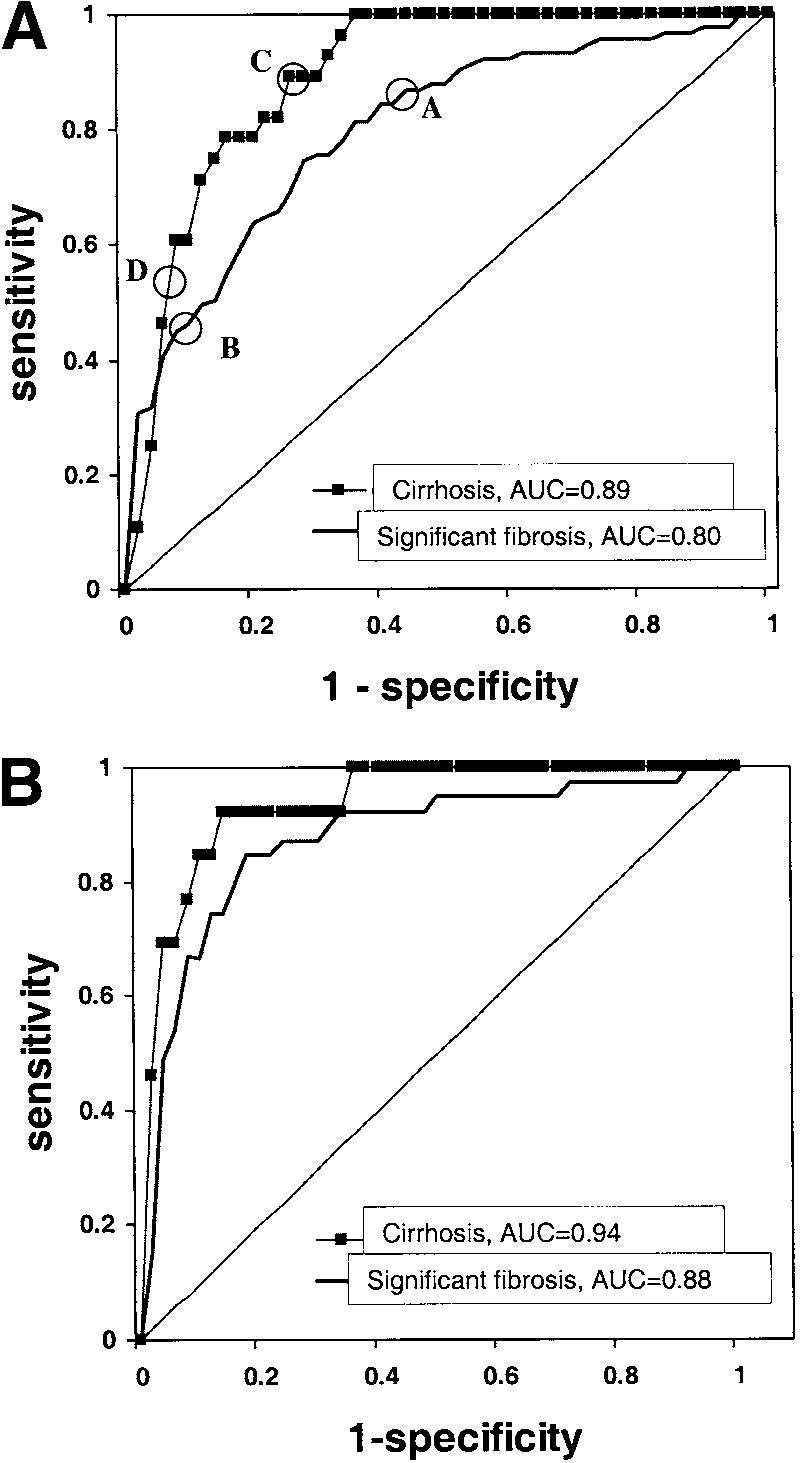
ROC curves of APRI for predicting significant fibrosis
fulfilled the study entry criteria and comprised the valida-
and cirrhosis in the training set were plotted in Fig. 2A
tion set. Characteristics of the validation set were similar
with AUC of 0.80 and 0.89, respectively (Table 3). Based
to that of the training set, in particular, there was no
on the ROC, 2 cut-off points were chosen to predict the
difference in the mean fibrosis score and the proportion
absence (coordinate A: APRI Յ 0.50) or presence (coor-
with significant fibrosis and cirrhosis. The 2 groups also
dinate B: APRI Ͼ 1.50) of significant fibrosis (Fig. 2A).
were comparable in platelet count and AST value. How-
For patients with APRI of 0.50 or less, 47 of 55 (85%)
ever, there were more African Americans, a higher pro-
would not have significant fibrosis. Among the 91 pa-
portion with acquisition of hepatitis C through other
tients who had significant fibrosis, only 8 (9%) would
means besides transfusion and IDU, a higher viral load,
have APRI of 0.50 or less, 7 of whom had an Ishak score
and a higher ALP level in the validation set (Table 1).
of 3 and 1 had an Ishak score of 4. For patients with APRI
Models comprising platelet count and AST level for
greater than 1.50, 37 of 42 (88%) would have significant
prediction of significant fibrosis and cirrhosis were ap-
fibrosis, and only 5 of 101 (5%) without significant fibro-
plied to the validation set. The area under ROCs (AUC)
sis would be classified incorrectly. Together, using APRI
for prediction of significant fibrosis and cirrhosis were
below the lower cut-off value (0.50) and above the higher
0.87 (95% confidence interval [CI], 0.79-0.95) and 0.93
cut-off value (1.50), 51% of the patients could be identi-
(95% CI, 0.85-1.0), respectively. Formulas with more
fied correctly as either without or with significant fibrosis
variables did not improve the AUC for either significant
fibrosis or cirrhosis in the validation set (Table 3).
Similarly, 2 cut-off points were chosen to predict the
Novel Index in Predicting Liver Fibrosis. Because
absence (coordinate C: APRI Յ 1.00) or presence (coor-
platelet count and AST level were the most important
dinate D: APRI Ͼ 2.00) of cirrhosis (Fig. 2A). For pa-
predictors of both significant fibrosis and cirrhosis, we
tients with APRI of 1.00 or less, 123 of 126 (98%) would
further analyzed the relationship between these 2 factors
not have cirrhosis. Only 3 of 28 (11%) with cirrhosis
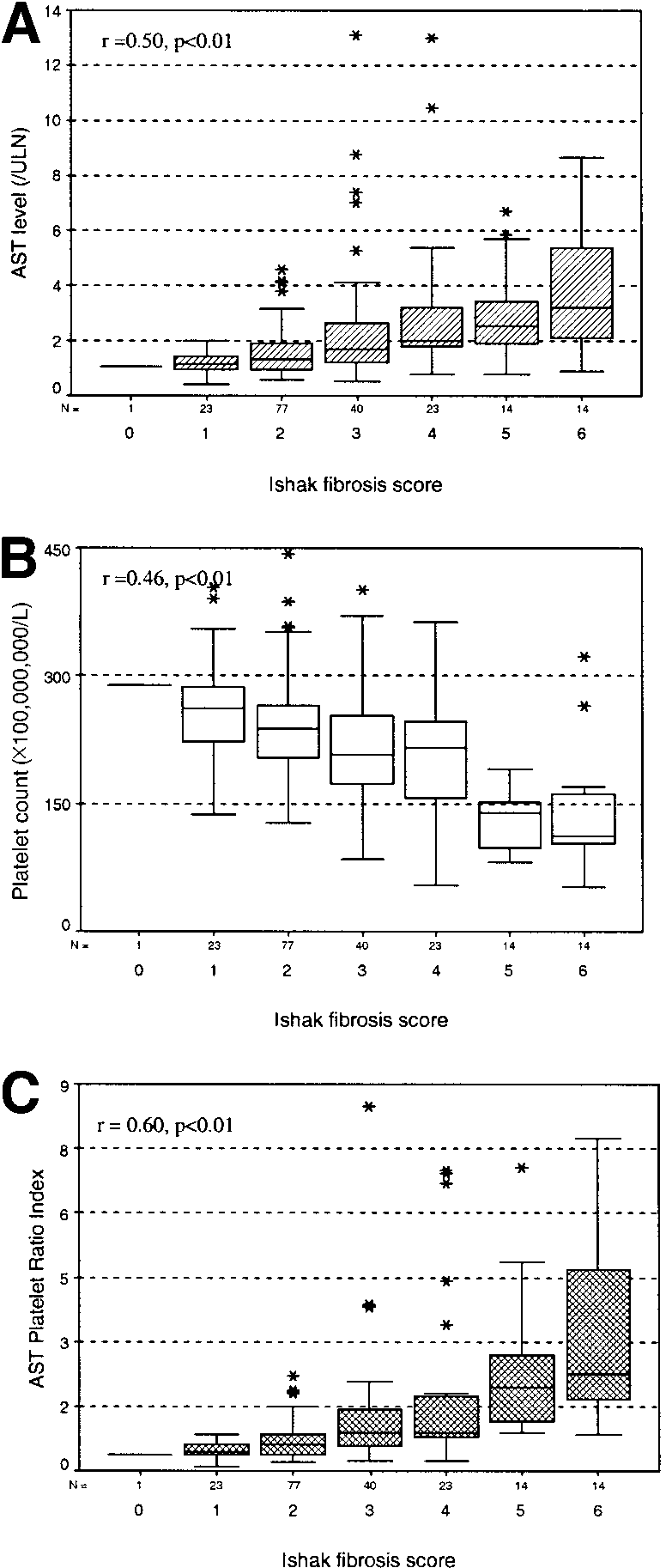
and the stage of hepatic fibrosis. Figure 1A and B showed
would be classified falsely. On the other hand, for patients
that severity of liver fibrosis was correlated significantly
with APRI greater than 2.00, 16 of 28 (57%) had cirrho-
with a gradual increase in AST level (r ϭ .50, P Ͻ .001) as
sis, and only 12 of 164 (7%) without cirrhosis would be
well as a decrease in platelet count (r ϭ Ϫ.46, P Ͻ .001).
identified falsely. Among the 12 patients with APRI
However, there was significant overlap in AST and plate-
greater than 2.00 but who did not have cirrhosis, 1 had an
let among patients with different stages of fibrosis. To
Ishak score of 2, 6 had an Ishak score of 3, and 5 had an
amplify the difference in AST and platelet values among
Ishak score of 4. Using the cut-off values of 1.00 and 2.00,
patients with different fibrosis stages, we devised a novel
the absence or presence of cirrhosis can be identified in
index, called the AST to platelet ratio index (APRI):
Applying APRI to the validation set, AUC for predic-
tion of significant fibrosis and cirrhosis were 0.88 (95%
CI, 0.80-0.96) and 0.94 (95% CI, 0.89-1.0), respectively
APRI was correlated significantly with the stage of fibro-
(Fig. 2B). Accuracy of using APRI for prediction of sig-
sis, with a higher correlation coefficient than platelet
nificant fibrosis and cirrhosis in the validation set is com-
count, or AST level alone (r ϭ .60, P Ͻ .001) (Fig. 1C).
parable with models with a formula comprising more
Finally, we applied the models to the 270 patients from
the training and validation sets combined. For the formu-las comprising platelet count and AST level, the AUCwere 0.82 (95% CI, 0.77-0.87) and 0.92 (95% CI, 0.87-0.96) for prediction of significant fibrosis and cirrhosis,respectively. For APRI, the AUC were 0.83 (95% CI,0.78-0.88) and 0.90 (95% CI, 0.86-0.94) for predictionof significant fibrosis and cirrhosis, respectively.
To show the use of APRI in predicting fibrosis, for a
hypothetical patient with CHC who has a platelet countof 120 ϫ 109/L and an AST level of 90 IU/L (ULN ϭ45), the APRI could be calculated as follows:
This APRI value is more than 1.5 (the higher cut-off valuefor significant fibrosis), so the positive predictive value forsignificant fibrosis is 0.88. The APRI value is less than 2.0
Fig. 1. Box plot of (A) AST, (B) platelet count, and (C) AST platelet
ratio index in relation to the Ishak fibrosis score. The box represents the interquartile range. The whiskers indicate the highest and lowest values, and the asterisks represent outliers. The line across the box indicates the median value.
variables (Table 3). Predictive values of the APRI in thevalidation set were similar to that in the training set. Forthe prediction of significant fibrosis in the validation set,the positive predictive value and negative predictive valueof an APRI of 0.50 were 64% and 90%, and the corre-sponding values for an APRI of 1.50 were 91% and 65%,respectively. For the prediction of cirrhosis in the valida-tion set, the positive and negative predictive value of anAPRI of 1.00 were 35% and 100%, and the correspond-
Fig. 2. ROC curves of APRI in the prediction of significant fibrosis and
cirrhosis in the (A) training set and (B) validation set. An AUC of 1.0 is
ing values for APRI of 2.00 were 65% and 95%, respec-
characteristic of an ideal test, whereas an AUC of 0.5 or less indicates
Table 4. Accuracy of APRI in Predicting Significant Fibrosis and Cirrhosis in the Training Set Actual Fibrosis All Patients Stage 0-2 Stage 3-6 (n ؍ 192) (n ؍ 101) Sensitivity Specificity Actual Fibrosis Stage 0-4 Stage 5-6 (n ؍ 164)
Abbreviations: PPV, positive predictive value; NPV, negative predictive value.
(the higher cut-off level for cirrhosis), so the negative pre-
naive patients only because several studies have shown
dictive value for cirrhosis is 0.93. Hence, this patient is
that liver histology may improve even among nonre-
likely to have significant fibrosis but not cirrhosis.
sponders to interferon-based therapy.33-35
Secondly, our study included a sufficient proportion of
Discussion
patients with significant fibrosis (47%) and cirrhosis
In this study, we attempted to develop a single model
(15%), thus allowing us to study variables that could pre-
using routinely available laboratory test results to predict
dict both of the study endpoints within the same patient
significant fibrosis and cirrhosis in a consecutive series of
population. Although the overall study population only
treatment-naive CHC patients. We found that platelet
included 270 patients, and differences in race and mode
count, AST level, and ALP level were the independent
of infection were present between the training and valida-
predictors for significant fibrosis, whereas platelet and
tion sets, the accuracy of APRI was validated in a sequen-
white cell count, AST and ALP levels, as well as AST/ALT
tial cohort of CHC patients undergoing a liver biopsy at
ratio, were the independent predictors for cirrhosis. Our
our institution. This suggests that the model is robust and
findings echoed results from many previous studies,
which showed that platelet count, AST level, and AST/ALT
Most importantly, our predictive model consists of ob-
ratio were important predictors of either significant fibrosis
jective and readily available laboratory variables. Both
or cirrhosis.17-27 To amplify the opposite relationship be-
platelet count and AST level are routine tests performed
tween the stage of fibrosis and AST level and platelet count,
in CHC patients in clinical practice, so no additional tests
we devised a novel index, the APRI, which was simple to use
are needed. The finding of decreased platelet count and
and had comparable accuracy with models that comprised 3
increased AST level with progression of liver fibrosis has
or more variables in predicting both significant fibrosis and
been reported in many studies. With increasing fibrosis
cirrhosis. The performance of APRI in predicting significant
and worsening portal hypertension, there is increased se-
fibrosis and cirrhosis was validated in a subsequent set of
questration and destruction of platelets in the enlarging
spleen.36 In addition, studies in liver transplant patients
Many studies on prediction of significant fibrosis and
showed that progression of liver fibrosis is associated with
cirrhosis among CHC patients have been published in the
decreased production of thrombopoietin by hepatocytes,
past few years.13-27 Our study has several unique features.
and hence reduced platelet production.37,38 Progression
First, we recruited consecutive patients undergoing per-
of liver fibrosis may reduce the clearance of AST,39 lead-
cutaneous liver biopsies at our medical center who met
ing to increased serum AST levels. In addition, advanced
eligibility criteria. Many prior studies have recruited only
liver disease may be associated with mitochondrial injury,
patients enrolled in treatment trials,18,32 which may have
resulting in more marked release of AST, which is present
introduced selection bias. Our study included treatment-
in mitochondria and cytoplasm, relative to ALT.40,41
To amplify the difference in AST and platelet values
were objective laboratory results, most of which were
among patients with different stages of fibrosis, we de-
available in the hospital computer system. All histologic
vised a novel index, the APRI. The concept of a ratio of 2
slides were retrieved and re-read by one liver pathologist
important variables in prediction of significant fibrosis is
(J.K.G.) to avoid interobserver discrepancy. In addition,
not new. In the study by Williams and Hoofnagle,32 the
all the slides were re-read over a 12-week period to mini-
investigators observed that as patients with chronic liver
disease progressed, AST levels increased more than ALT
We acknowledge that there are limitations to our
levels. The investigators exploited the difference between
study. Our study included patients from a university
these 2 factors and devised the AST/ALT ratio for predic-
hepatology clinic, half of whom had significant fibrosis on
tion of cirrhosis. Although several investigators have con-
histology and none had prior antiviral treatment.
firmed the value of AST/ALT ratio in predicting
Whether our results can be generalized to community-
cirrhosis,22-25 its accuracy varies widely among studies,
based practice in which patients may have milder disease,
with positive predictive values ranging from 0.64 to 1.00,
or to patients who failed prior antiviral therapy remain to
and negative predictive values ranging from 0.72 to 0.88,
be determined. Despite the simplicity and accuracy of the
respectively. In this study, although AST/ALT ratio was 1
APRI, there was overlap among patients with different
of the 5 independent predictors of cirrhosis, it alone was
stages of fibrosis. Thus, the use of APRI in the prediction
insufficient for accurate prediction of cirrhosis. In addi-
of fibrosis in individual patients with CHC must be con-
tion, AST/ALT ratio alone has not been shown to be
firmed in prospective studies. Finally, our study is based
useful in predicting significant fibrosis.17-21
on the premise that liver biopsy is the gold standard for
The APRI was accurate in predicting both significant
assessing hepatic fibrosis, but sampling error as well as
fibrosis and cirrhosis, with area under ROC of 0.80 and
intra- and interobserver variability can complicate the
0.89 in the training set, and 0.88 and 0.94 in the valida-
correlations between histology and noninvasive markers
tion set, respectively. Although we could not define one
single cut-off value to predict either study endpoint, using
In conclusion, we showed that a simple index, the
values below the lower cut-off level or above the higher
APRI, consisting of 2 readily available laboratory results
cut-off level, a prediction of absence or presence of cirrho-
(AST level and platelet count), can predict significant
sis could be made in 81% of patients. Similarly, a predic-
fibrosis and cirrhosis in treatment-naive CHC patients
tion of absence or presence of significant fibrosis could be
with a very high degree of accuracy. Our results were
made in 51% of patients. Our index compared favorably
validated in a subsequent cohort of CHC patients at our
with results from other studies. Forns et al.21 could predict
institute. The APRI can be determined in the clinic or at
significant fibrosis in 51% of patients using 4 factors
the bedside. Using one simple formula, significant fibrosis
(platelet count, ␥-glutamyltransferase level, age, and cho-
and cirrhosis can be predicted accurately in 51% and 81%
lesterol), with an AUC of 0.94. The fibrosis index from
of treatment-naive CHC patients, respectively, potentially
the MULTIVIRC group could predict significant fibrosis
avoiding the need for liver biopsies in these patients. Further
in 46% of patients by using a combination of 6 markers
prospective studies are needed to validate the APRI in a larger
(␣2 macroglobulin, haptoglobin, ␥ globulin, apolipop-
number of CHC patients in other institutes, in particular,
totein A1, ␥ glutamyl-transpeptidase, and total bilirubin),
community-based practices where the prevalence of signifi-
with an AUC of 0.84.15 Although the value of the index of
cant fibrosis and cirrhosis may be lower, and in patients who
Forns et al.21 in predicting the absence of significant fi-
had received antiviral therapy previously.
brosis was better than the APRI, it involved a complicatedformula. The major advantage of the APRI is its simplic-
References
ity. APRI can be determined in the clinic or bedside with-out the help of a calculator. Moreover, the APRI allows
1. Gebo KA, Herlong HF, Torbenson MS, Jenckes MW, Chander G, Ghanem
KG, El-Kamary SS, et al. Role of liver biopsy in management of chronic
clinicians to use one formula to predict significant fibrosis
hepatitis C: a systematic review. HEPATOLOGY 2002;36:S161-S172.
2. National Institutes of Health Consensus Development Conference State-
Although our study was retrospective in design, we
ment: Management of hepatitis C: 2002—June 10-12, 2002. HEPATOL-
took all the necessary measures to maximize the accuracy
3. Dienstage JL. The role of liver biopsy in chronic hepatitis C. HEPATOLOGY
of our data collection. To ensure consistency in data ex-
traction, a predetermined set of criteria for all subjective
4. Lauer GM, Walker BD. Hepatitis C virus infection. N Engl J Med 2001;
variables was established before the medical records were
5. Yano M, Kumada H, Hage M, Ikeda K, Shimamatsu K, Inoue O, Hashi-
reviewed, and all data extraction was performed by one
moto E, et al. The long-term pathological evolution of chronic hepatitis C.
investigator (C.T.W.). The key variables in our study
6. Lok A, McMahon BJ. Chronic hepatitis B. HEPATOLOGY 2001;34:1225-
24. Park GJ, Lin BP, Ngu MC, Jones DB, Katelaris PH. Apartate aminotrans-
ferase: alanine aminotransferase ratio in chronic hepatitis C infection: is it
7. Jalan R, Hayes PC. UK guidelines on the management of variceal haem-
a useful predictor of cirrhosis? J Gastroenterol Hepatol 2000;15:386-390.
orrhage in cirrhotic patients. Gut 2000;46:III1-III15.
25. Imperiale TF, Said AT, Cummings OW, Born LJ. Need for validation of
8. Cadranel JF, Rufat P, Degos F. Practices of liver biopsy in France: results of
clinical decision aids: use of the AST/ALT ratio in predicting cirrhosis in
a prospective nationwide survey. HEPATOLOGY 2000;32:477-481.
chronic hepatitis C. Am J Gastroenterol 2000;95:2328-2332.
9. Bedossa P, Poynard T, and the Metavir Cooperative Group. Intraobserver
26. Saddeh S, Cammell G, Carey WD, Younossi Z, Barnes D, Easley K. The role
and interobserver variations in liver biopsy interpretation in patients with
of liver biopsy in chronic hepatitis C. HEPATOLOGY 2001;133:196-200.
chronic hepatitis C. HEPATOLOGY 1994;20:15-20.
27. Kaul V, Friedenberg FK, Braitman LE, Anis U, Zaeri N, Fazili J, Herrine
10. Westin J, Lagging LM, Wejstal R, Norkans G, Dhillon AP. Interobserver
SK, et al. Development and validation of a model to diagnose cirrhosis in
study of liver histology using the Ishak score in patients with chronic
patients with hepatitis C. Am J Gastroenterol 2002;97:2623-2628.
hepatitis C virus infection. Liver 1999;19:183-187.
28. Alter MJ. Prevention of spread of hepatitis C. HEPATOLOGY 2002;36:S93-S98.
11. Regev A, Berho M, Jeffers LJ, Milikowski C, Molina EG, Pyrsopoulos NT,
29. Centers for Disease Control. Recommendation for prevention and control
Feng ZZ, et al. Sampling error and intraobserver variation in liver biopsy in
of hepatitis C virus (HCV) infection and HCV-related chronic disease.
patients with chronic HCV infection. Am J Gastroenterol 2002;97:2614-
MMWR Morb Mortal Wkly Rep 1998;47:RR-19:RR-39.
30. Dardenne AN. The spleen. In: Cosgrove DO, Meire HB, Dewbury KCD,
12. Geroge J. Biochemical markers of hepatic fibrogenesis: single measure-
eds. Clinical Ultrasound. Edinburgh: Churchill Livingstone, 1993;353-365.
ments are not reliable enough to replace liver biopsy. J Gastroenterol Hepa-
31. Ishak K, Baptista A, Bianchi L, Callea F, De Groote J, Gudat J, Denk H,
et al. Histological grading and staging of chronic hepatitis. J Hepatol
13. McHutchison JG, Blatt LM, de Medina M, Craig JR, Conrad A, Schiff
ER, Tong MJ. Measurement of serum hyaluronic acid in patients with
32. Williams AL, Hoofnagle JH. Ratio of serum aspartate to alanine amino-
chronic hepatitis C and its relationship to liver histology. Consensus In-
transferase in chronic hepatitis. Relationship to cirrhosis. Gastroenterology
terferon Study Group. J Gastroenterol Hepatol 2000;15:945-951.
14. Guechot J, Laudat A, Loria A, Serfaty L, Poupon R, Giboudeau J. Diag-
33. de Ledinghen V, Trimoulet P, Winnock M, Bernard PH, Bourliere M,
nostic accuracy of hyaluronan and type III procollagen amino-terminal
Portal I, Remy AJ, et al. Daily or three times per week interferon alpha-2b
peptide serum assays as markers of liver fibrosis in chronic viral hepatitis C
in combination with ribavirin or interferon alone for the treatment of
evaluated by ROC curve analysis. Clin Chem 1996;42:558-563.
patients with chronic hepatitis C not responding to previous interferon
15. Imbert-Bismut F, Ratziu V, Pieroni L, Charlotte F, Benhamou Y, Poynard
T, for the MULTIVIRC group. Biochemical markers of liver fibrosis in
34. Teuber G, Berg T, Naumann U, Raedle J, Brinkmann S, Hopf U, Zeuzem
patients with hepatitis C virus infection: a prospective study. Lancet 2001;
S. Randomized, placebo-controlled, double-blind trial with interferon-
alpha with and without amantadine sulphate in primary interferon-alpha
16. Fontana RJ, Lok AS. Noninvasive monitoring of patients with chronic
nonresponders with chronic hepatitis C. J Viral Hepat 2001;8:276-283.
hepatitis C. HEPATOLOGY 2002;36:S57-S64.
35. Di Bisceglie AM, Thompson J, Smith-Wilkaitis N, Brunt EM, Bacon BR.
17. Bonacini M, Hadi G, Govindarajan S, Lindsay KL. Utility of a discriminant
score for diagnosing advanced fibrosis or cirrhosis in patients with chronic
Combination of interferon and ribavirin in chronic hepatitis C: re-treat-
hepatitis C virus infection. Am J Gastroenterol 1997;92:1302-1304.
ment of nonresponders to interferon. HEPATOLOGY 2001;33:704-707.
18. Pohl A, Behling C, Oliver D, Kilani M, Monson P, Hassanein T. Serum
36. Aster R. Pooling of platelets in the spleen: role in the pathogenesis of
aminotransferase levels and platelet counts as predictors of degree of fibro-
“hypersplenic” thrombocytopenia. J Clin Invest 1996;45:645-657.
sis in chronic hepatitis C virus infection. Am J Gastroenterol 2001;96:
37. Kawasaki T, Takeshita A, Souda K, Kobayashi Y, Kikuyama M, Suzuki F,
Kageyama F, et al. Serum thrombopoietin levels in patients with chronic
19. Poynard T, Bedossa P, METAVIR and CLINIVIR cooperative study
hepatitis and liver cirrhosis. Am J Gastroenterol 1999;94:1918-1922.
groups. Age and platelet count: a simple index for predicting the presence
38. Adinolfi LE, Giordano MG, Andreana A, Tripodi MF, Utili R, Cesaro G,
of histological lesions in patients with antibodies to hepatitis C virus. J
Ragone E, et al. Hepatic fibrosis plays a central role in the pathogenesis of
thrombocytopenia in patients with chronic viral hepatitis. Br J Haematol
20. Wong V, Caronia S, Wight D, Almer CR, Petrik J, Britton P, Alexander
GJM. Importance of age in chronic hepatitis C virus infection. J Viral
39. Kamimoto Y, Horiuchi S, Tanase S, Morino Y. Plasma clearance of intra-
venously injected aspartate aminotransferase isozymes: evidence for pref-
21. Forns X, Ampurdanes S, Llovet JM, Aponte J, Quinto L, Martinez-Bauer E,
erential uptake by sinusoidal liver cells. HEPATOLOGY 1985;5:367-375.
Bruguera M, et al. Identification of chronic hepatitis C patients without he-
40. Okuda M, Li K, Beard MR, Showalter LA, Scholle F, Lemon SM, Wein-
patic fibrosis by a simple predictive model. HEPATOLOGY 2002;36:986-992.
man SA. Mitochondrial injury, oxidative stress, and antioxidant gene ex-
22. Reedy DW, Loo AT, Levine RA. AST/ALT ratio Ͼ or ϭ 1 is not diagnos-
pression are induced by hepatitis C virus core protein. Gastroenterology
tic of cirrhosis in patients with chronic hepatitis C. Dig Dis Sci 1998;43:
41. Nalpas B, Vassault A, Le Guillou A, Lesgourgues B, Ferry N, Lacour B,
23. Sheth SG, Flamm SL, Gordon FD, Chopra S. AST/ALT ratio predicts
Berthelot P. Serum activity of mitochondrial aspartate aminotransferase: a
cirrhosis in patients with chronic hepatitis C virus infection. Am J Gastro-
sensitive marker of alcoholism with or without alcoholic hepatitis. HEPA-
Title A Handbook of Statistical Analyses Using R (2nd Edition)Author Brian S. Everitt and Torsten HothornMaintainer Torsten Hothorn <Torsten.Hothorn@R-project.org>Description Functions, data sets, analyses and examples from the second edition of the book`A Handbook of Statistical Analyses Using R' (Brian S. Everitt and TorstenHothorn, Chapman & Hall/CRC, 2008). The first chapterof th
Manuscript of Review Article published in: MICROSCOPY RESEARCH and TECHNIQUE 2000; 48: 303-11 ROLE OF APOPTOSIS IN GASTRIC EPITHELIAL TURNOVER Axel von Herbay 1 , Jochen Rudi 2 1 Institute of Pathology, 2 Medizinische Klinik IV, University of Heidelberg, GermanyAddress for correspondance: Priv.-Doz. Dr. med. A. von Herbay, Pathologisches Institut,Universitätsklinikum, Im Neuenheimer F
 Finally, we applied the models to the 270 patients from
the training and validation sets combined. For the formu-las comprising platelet count and AST level, the AUCwere 0.82 (95% CI, 0.77-0.87) and 0.92 (95% CI, 0.87-0.96) for prediction of significant fibrosis and cirrhosis,respectively. For APRI, the AUC were 0.83 (95% CI,0.78-0.88) and 0.90 (95% CI, 0.86-0.94) for predictionof significant fibrosis and cirrhosis, respectively.
Finally, we applied the models to the 270 patients from
the training and validation sets combined. For the formu-las comprising platelet count and AST level, the AUCwere 0.82 (95% CI, 0.77-0.87) and 0.92 (95% CI, 0.87-0.96) for prediction of significant fibrosis and cirrhosis,respectively. For APRI, the AUC were 0.83 (95% CI,0.78-0.88) and 0.90 (95% CI, 0.86-0.94) for predictionof significant fibrosis and cirrhosis, respectively.