La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Doi:10.1016/s0736-4679(03)00197-5
The Journal of Emergency Medicine, Vol. 25, No. 3, pp. 245–249, 2003
doi:10.1016/S0736-4679(03)00197-5 Original Contributions RIZATRIPTAN RPD FOR SEVERE MIGRAINE IN THE EMERGENCY DEPARTMENT—A MULTICENTER STUDY
Emile Hay, MD,* Joseph Rodrig, MD,† Amer Hussain, MD,‡ Hashmonai Derazon, MD,* Giorgio
Kopelovitch, MD,† Ella Dashkovsky, MD,‡ Natalia Bokish, MD,* Michael Kafka, MD,‡
Irina Shtibelman, RN,* and Shoshana Nassimyan, RN*
*Department of Emergency Medicine of the Barzilai Medical Center, Ashkelon, Israel, †Sanz Medical Center, Laniado Hospital,
Netanya, Israel, and ‡Bnei Zion Hospital, Haifa, Israel
Reprint Address: Emile Hay, MD, Head of Emergency Department, Barzilai Medical Center, Ashkelon 78306, Israel
e Abstract—Many patients with severe migraine come to INTRODUCTION the Emergency Department (ED) due to failure of different drug regimens to stop their headache. We treated 98 pa-
Migraine affects 13 to 18% of women and 3 to 6% of
tients with severe migraine who were seen in three different
men, with peak prevalence between 35 and 45 years of
EDs. We used rizatriptan RPD wafers 10 mg and observed
age Although there is considerable variation in the
the patients for 2 h. We found that at 2 h, 92.9% (91/98) of
severity and frequency of migraine attacks among pa-
the patients had pain relief, and 73.5% were pain free. The
tients and within individuals, more than half of all pa-
mean time to pain relief was 26.9 ؎ 29.6 min with a median
tients with migraines have restricted their work and their
of 15 min, and the time to pain free was 70.2 ؎ 47.3 min with a median of 75 min. Eighty-five percent of the patients
social life significantly The exact pathophysiology of
were free of associated symptoms, such as nausea and
migraine remains poorly understood, but numerous stud-
vomiting, at 2 h with a mean time to symptom free of 55 ؎
ies support the neurovascular theory and the role of the
47.5 min and a median of 45 min. Rizatriptan was reported to be much better than other drugs by 74.4% of the pa- tients. Side effects were minor and transient. Recurrence of
Until the last decade, migraine patients had a rather
migraine occurred part of the day in 17.1% of the patients
limited choice of antimigraine drugs. Traditional thera-
and all day or almost all day in 8.6% of the patients only.
pies included simple analgesics such as acetaminophen
The results were consistent in all three EDs. We conclude
and salicylates, nonsteroidal anti-inflammatory drugs, er-
that rizatriptan RPD is very effective and reliable as a
gotamine, and antiemetic drugs The revolution in
first-line therapy for acute migraine in the ED. It dis-
migraine therapy began with the discovery of the triptan
solves immediately in the mouth without the inconve-
drugs, which activate the serotonin receptor 5-HT
nience of an injection. It works fast and has few side effects and low headache recurrence. 2003 Elsevier
and relieve the headache Several triptan drugs
are being marketed, including sumatriptan, naratriptan,zolmitriptan, and rizatriptan (Rizalt). Other new
e Keywords—migraine; rizatriptan; rizatriptan in ED;
triptans are under investigations. These drugs differ in
migraine in ED
their bioavailability, onset of action, duration of action,
RECEIVED: 15 February 2002; FINAL SUBMISSION RECEIVED: 4 December 2002;ACCEPTED: 7 January 2003
adverse reactions, their capability to penetrate the blood
Table 1. Exclusion Criteria
brain barrier (BBB), and activation of 5-HT receptors
which easily penetrates the BBB, is rapidly absorbed,
and has a rapid onset of action Studies with
Unstable angina pectoris. Basilar migraine.
rizatriptan in two different doses, 5 and 10 mg, and in
two forms, conventional tablets and rapidly dissolving
Use of other triptans less than 24 h before beginning the
freeze-dried (RPD) wafers 10 mg, showed that it is
effective and well tolerated with low side effects and
better quality of life after treatment The RPD
Patients taking ergot derivatives, propranolol, SSRI and MAO
wafer dissolves immediately in the mouth and thus has
the advantage of eliminating the need for drinking water. This form is best tolerated by the vomiting patient
Patients with severe migraine attack often seek help in
severe to the degree that they refrained from any physical
the Emergency Department (ED). Drugs usually used to
or social activity. Only patients who had at least one
treat acute migraine in the ED include parenteral opioids
migraine attack per month during the last 6 months and
and phenothiazines These drugs, although ef-
graded their headache as severe were enrolled in the
fective, are nonspecific and have many side effects, in-
study. For all the patients, it was the first time that they
cluding severe hypotension Sumatriptan subcu-
ever took rizatriptan in any form for their migraine, but
taneous injections have been used to treat acute migraine
not necessarily their first experience with other triptans.
in the ED with good results, with the inconvenience of
Exclusion criteria are described in Eligible
administering an injection. Hay reported a pain relief rate
patients were treated with RzRPD 10 mg wafer and
of 80% within 20 to 30 min, and pain free rate of 75%
observed for 2 h. Nonresponders, patients who had no
within 90 min Akpunonu et al. reported a pain relief
improvement of their headache, and partial responders,
rate of 75% within 34 min, and 70% of the patients had
patients who had pain relief but were not pain free,
received other analgesics. During the 2-h observation
period, we evaluated the following parameters every 15
(RzRPD) would be superior due to its ease of adminis-
min: time to cessation of associated symptoms; nausea
tration, its rapid onset of action, and its specific antimi-
and vomiting; photophobia and phonophobia; time to
graine effect. For this reason, we conducted the follow-
pain relief; time to pain free; and adverse reactions.
ing prospective unblinded study to examine the efficacy,
Patients were discharged home or admitted to the hospi-
tolerability, and quality of life after Rizatriptan RPD
tal if their headache remained as severe as before.
wafer (RzRPD) administration as a first-line therapy for
Two nurses conducted telephone interviews with each
acute migraine in the ED. The study was conducted
patient 24 h after discharge from the ED. Patients were
simultaneously in three different Emergency Depart-
asked to answer a quality-of-life questionnaire to evalu-
ments. The Institutional Board for Research in Human
ate the rate of migraine recurrence and associated symp-
Beings did not approve the use of placebo for double-
toms, and any disability that interfered with the quality of
blind study. The members of the Board thought it was
life after discharge Interference with quality of
not ethical to give placebo to patients with severe head-
life was evaluated by the persistence of nervousness,
ache in the ED. We could not obtain the agreement of
restriction of social and work activities, disturbed con-
other companies to conduct a double-drug double-blind
centration, sleep disturbance, and disturbed mood.
This study was approved by the Institutional Board
The study was supported financially by Merck Sharp
and Dome Pharmaceutical Co. None of the authors hasany association with the company. MATERIALS AND METHODS
A total of 98 patients were enrolled in the study, 87.8%of them were women. The mean age was 40.39 Ϯ 9.95,
Patients over 18 years of age with known migraine [the
range 18 – 63 years. summarizes the presence of
International Headache Society (IHS) definition of mi-
associated symptoms among the patients, before and
graine who came to the ED for acute migraine
after RzRPD treatment. At 2 h, 90.6% of the patients
attack were considered eligible for the study. Patients
were free of nausea, 100% stopped vomiting, 89% were
were asked to grade their headache as mild, moderate, or
free of phonophobia, and 90% were free of photophobia. Table 2. Associated Symptoms Among Patients (N ؍ 98) Table 4. Side Effects During the 2-Hour Observation
Ninety-one patients out of 98 (92.9%) had pain reliefwithin 2 h and 73.5% of the patients were pain free by
DISCUSSION
2 h. The mean time to pain relief was 26.9 Ϯ 29.6 minwith a median of 15 min, and the mean time to pain free
Our study demonstrates better efficacy of rizatriptan in
was 70.2 Ϯ 47.3 min with a median of 75 min
achieving pain relief and pain free end points at 2 h than
Eighty-five percent (85%) of the patients were free of
in previous studies. The majority of our patients, 92.9%,
associated symptoms within 2 h, with a mean time to
had pain relief with a median time to relief of 15 min vs.
symptom free of 55 Ϯ 47.5 min and a median of 45 min.
67– 80% found in other studies, and 73.5% were pain
Rizatriptan was reported to be much better than other
free by 2 h with a median of 75 min vs. 40 – 49% of the
drugs ever used by 74.4% of the patients, 18.9% reported
it as slightly better, and only 6.7% of the patients re-
same is true for the percentage of symptom-free patients
ported that it was similar to other drugs. None reported
at 2 h: 85% in our study with a median time of 45 min vs.
that it was worse than other therapies. The results of the
22–75% in the same studies cited We believe
three EDs were not significantly different, emphasizing
that these significant differences originate from the dif-
the consistency of the effect of RzRPD.
ferent design of the studies. Our patients were examined
Only a few patients reported side effects during the
in the EDs, and it was the emergency physician who
2-h treatment schedule. The side effects are presented in
decided whether that headache was consistent with the
Side effects included: weakness in 4 patients
definition of the IHS of migraine. It should be remem-
and dizziness in 5 patients. Two patients experienced
bered that a migraine patient may also have a tension
euphoria. All these side effects were transient and not
headache severe enough to be confused with acute mi-
necessarily related to rizatriptan RPD. Three patients
graine, and this patient will not respond properly to
were hospitalized for 24 h for continuous pain and their
rizatriptan, meaning failure of treatment. Only those se-
course was uneventful. Two of them were diagnosed
lected patients with acute migraine were treated with
with tension headache and the third with upper respira-
rizatriptan. One may conclude that the more specific the
diagnosis of the attack, the better the response will be.
The results of the quality of life survey 24 h after
Our results are also better than those achieved with
discharge from the ED are presented in Most ofthe patients (74.3%) had hardly any headache, 17.1% hadheadache part of the day, and 8.6% continued to expe-rience headache all day or almost all day. More than half
Table 5. Quality of Life 24 Hours After Release From the
of the patients had restriction of normal activities and
mood disturbances. About 40% of the patients had dif-
ficulties in concentration and interference with sleep. Table 3. Time to Pain Relief, Symptom Free and Pain Free Figure 1. Present study results compared to average results of previous studies.
sumatriptan injection, and without the inconvenience of
that the patients ignored the side effects, or perhaps they
thought that side effects were part of the migraine. In-
Regarding recurrence of migraine among rizatriptan
terestingly, two patients reported euphoria, a side effect
10 mg responders, it is reported to range between 35%
that we did not find in other studies. A possible expla-
and 47% In our study, the rate of recurrence
nation is the activation of serotonin receptors by this
was much lower: 74.3% of the patients reported they had
hardly any headache during the 24 h after discharge;17.1% of the patients experienced headache part of theday and only 8.6% reported headache for the whole day. CONCLUSIONS
Again, these differences in the results might originatefrom the rigid selection of patients and from the different
We find rizatriptan RPD wafer 10 mg to be very effective
method of follow-up. In our study, two nurses conducted
as a first-line therapy for acute migraine attack diagnosed
the telephone interviews and contacted every patient who
by physicians in the ED. Most patients left the ED
was enrolled in the study. The nurses explained all the
without pain and without the need for additional analge-
questions to the patients and the questionnaires were
sics. The immediate side effects were minimal and most
of the patients found it to be much better than any other
Rizatriptan also showed good results in the rest of the
drug. We strongly recommend the use of rizatriptan RPD
parameters of quality of life except for restriction of
10 mg wafers for the treatment of acute migraine in theED.
normal life activities, disturbed concentration, and dis-turbed mood. About half of the patients reported thesedisturbances all day or part of the day.
Despite these encouraging results, one should be
REFERENCES
aware of the limitations of the study. Partial responders
1. Stewart WF, Schechter A, Rasmussen BK. Migraine prevalence. A
took other analgesics that might affect the results, and
review of population based studies. Neurology 1994;44(Suppl):
patients were not offered a second tablet of rizatriptan,
which could have changed the results. The same reser-
2. Rasmussen BK, Olesen J. Migraine with aura and migraine without
aura: an epidemiologic study. Cephalalgia 1992;12:221– 8.
3. Pryse-Phillips W, Findlay H, Tugwell P, Edmeads J, Murray TJ,
Comparing side effects that the patients reported, it is
Nelson RF. A Canadian population survey on the clinical epide-
interesting that only few patients complained of adverse
miologic and societal impact of migraine and tension-type head-ache, part II. Can J Neurol Sci 1992;19:333–9.
reactions, and many of the known side effects were not
4. Ferrari MD, Saxena PR. On serotonin and migraine: a clinical and
reported, such as chest pain, dry mouth, and abdominal
pharmacological review. Cephalalgia 1993;13:151– 65.
5. Deliganis AV, Peroutka SJ. 5-Hydroxytriptamine 1D receptor ag-
pain. We don’t have any explanation for that, but perhaps
onist predicts antimigraine efficacy. Headache 1991;31:300 –5.
the migraine attack was so severe in our selected group
6. Ferrari MD. Migraine. Lancet 1998;351:1043–51.
7. Martin GR. Serotonin receptor involvement in the pathogenesis
rizatriptan wafer for the acute treatment of migraine. Cephalalgia
and treatment of migraine. Goadsby PJ, Silberstein SD, eds. Head-
ache. Boston: Butterworth-Heinemann; 1991:25–39.
21. Carleton SC, Shesser RF, Pietrzak MP, et al. Double-blind multi-
8. Tfelt-Hansen P, Johnson ES. Nonsteroidal anti-inflammatory drugs
center study trial to compare the efficacy of intramuscular dihy-
in the treatment of the acute migraine attack. Olesen J, Tfelt-
droergotamine plus hydroxyzine versus intramuscular mepiridine
Hansen P, Welch KMA, eds. The headaches. New York: Raven
plus hydroxyzine for the emergency department treatment of acute
migraine headache. Ann Emerg Med 1998;32:129 –38.
9. Goadsby PJ. Pathophysiology of migraine: a disease of the brain.
22. Lane PL, McLellan BA, Baggoley CJ. Comparative efficacy of
Goadsby PJ, Silberstein SD, eds. Headache. Boston: Butterworth-
chlorpromazine and meperidine with dimenhydrinate in migraine
headache. Ann Emerg Med 1989;18:360 – 65.
10. Humphrey PP, Feniuk W. Mode of action of the anti-migraine drug
23. Coppola M, Yealy DM, Leibold RA. Randomized, placebo-con-
sumatriptan. Trends Pharmacol Sci 1991;12:444 – 6.
trolled evaluation of prochlorperazine versus metoclopramide for
11. Meloche J. Triptans and migraine: which drug for which patient.
emergency department treatment of migraine headache. Ann
12. Williamson DJ, Shepheard SL, Hill RG, Hargreaves RJ. The novel
24. Ducharme J, Beveridge RC, Lee JS, Beaulieu S. Emergency man-
anti-migraine agent rizatriptan inhibits neurogenic dural vasodila-
agement of migraine: is the headache really over. Acad Emerg
tion and extravasation. Eur J Pharmacol 1997;328:61– 4.
13. Cumberbatch MJ, Hill RG, Hargreaves RJ. Rizatriptan has central
25. Mariani PJ. Adverse reactions to chlorpromazine in the treatment
antinociceptive effects against durally evoked responses. Eur
of migraine. Ann Emerg Med 1988;17:380 –1.
26. Hay E. Treatment of migraine with sumatriptan in the emergency
14. Visser WH, Terwindt GM, Reines SA, Jiang K, Lines CR, Ferrari
department. Am J Emerg Med 1994;12:388 –9.
MD. Rizatriptan vs sumatriptan in the acute treatment of migraine.
27. Akpunonu BE, Mutgi AB, Federman DJ, et al. Subcutaneous
A placebo- controlled, dose-ranging study. Dutch/US Rizatriptan
sumatriptan for treatment of acute migraine in patients admitted to
Study Group. Arch Neurol 1996;53:1132–7.
the emergency department: a multicenter study. Ann Emerg Med
15. Sciberras DG, Polvino WJ, Gertz BJ, et al. Initial human experi-
ence with MK-462 (rizatriptan): a novel 5-HT
28. Headache Classification Committee of the International Headache
Society. Classification and diagnostic criteria for headache disor-
16. Tfelt-Hansen P, Teall J, Rodriguez F, et al. Oral rizatriptan versus
ders, cranial neuralgias and facial pain. Cephalalgia 1998;8(Suppl):
oral sumatriptan: a direct comparative study in the acute treatment
of migraine. Rizatriptan 030 Study Group. Headache 1998;38:
29. Hartmaier SL, Santanello NC, Epstein RS, Silberstein SD. Devel-
opment of a brief 24-hour migraine specific quality of life ques-
17. Goldstein J, Ryan R, Jiang K, et al. Crossover comparison of
tionnaire. Headache 1995;35:320 –9.
rizatriptan 5 mg and 10 mg versus sumatriptan 25 mg and 50 mg
30. Santanello NC, Hartmaier SL, Epstein RS, Silberstien SD. Vali-
in migraine. Rizatriptan Protocol 046 Study Group. Headache
dation of a new quality of life questionnaire for acute migraine
headache. Headache 1995;35:330 –7.
18. Santanello NC, Polis AB, Hartmaier SL, Kramer MS, Block GA,
31. Kramer MS, Matzura-Wolfe D, Polis A, et al. A placebo-controlled
Silberstein SD. Improvement in migraine-specific quality of life in
crossover study of rizatriptan in the treatment of multiple migraine
a clinical trial of rizatriptan. Cephalalgia 1997;17:867–72.
attacks. Rizatriptan Multiple Attack Study Group. Neurology
19. Teall J, Tuchman M, Cutler N, et al. Rizatriptan (Maxalt) for the
acute treatment of migraine and migraine recurrence. A placebo-
32. Visser WH, Teall JH, Malbecq W, et al. Early onset of action of
controlled, outpatient study. Headache 1998;38:281–7.
rizatriptan versus sumatriptan in the acute treatment of migraine
20. Ahrens SP, Farmer MV, Williams DL, et al. Efficacy and safety of
(abstract). Headache 1997;37:334 –5.
Sangue infetto: dagli errori ai bimbi “cavie”. E gli indennizzi non arrivano di Refusi e abbagli della commissione medica della Cecchignola di Roma nel valutare i risarcimenti. A Latina il caso di una donna che per 16 anni ha contagiato decine di pazienti. Dagli archivi del processo di Trento spuntano anche i trial clinici sugli umani, tra cui un 12enne. A volte basta un refuso per ri
Company Register FORBES COMPUTER SYSTEMS Please complete in typescript, First directors and secretary and intended situation of or in bold black capitals. registered office Company Number Company Name in full Proposed Registered Office (PO Box numbers only, are not acceptable)This is to certify that the above is/are the Registered holders
 The Journal of Emergency Medicine, Vol. 25, No. 3, pp. 245–249, 2003
doi:10.1016/S0736-4679(03)00197-5
The Journal of Emergency Medicine, Vol. 25, No. 3, pp. 245–249, 2003
doi:10.1016/S0736-4679(03)00197-5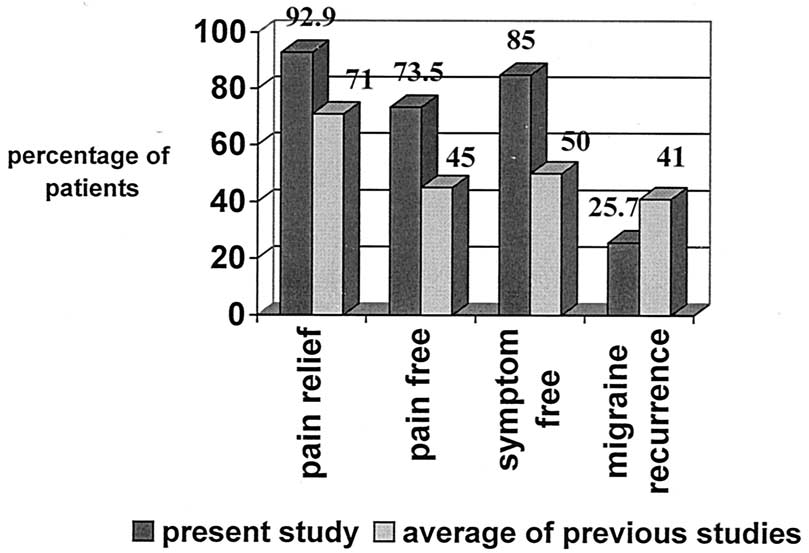 Figure 1. Present study results compared to average results of previous studies.
Figure 1. Present study results compared to average results of previous studies.