La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Evidence for anti-osteoporosis therapy in acute fracture situations—recommendations of a multidisciplinary workshop of the international society for fracture repair
j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / b o n e
Evidence for anti-osteoporosis therapy in acute fracture situations—Recommendations
of a multidisciplinary workshop of the International Society for Fracture Repair
The International Society for Fracture Repair convened a multidisciplinary workshop to assess the current
evidence around the interaction between anti-osteoporosis drugs and the healing of incident fractures, with
a view to making recommendations for clinical practice. The consensus was that there is no evidence-based
reason to withhold anti-resorptive therapy while a fracture heals, whether or not the patient was taking such
therapy when the fracture occurred. The workshop also considered existing models of service provision for
secondary prevention and concluded that the essential ingredient for reliable delivery is the inclusion of a
dedicated coordinator role. Several unresolved issues were defined as subjects for further research, including
the question of whether continuous long-term administration of anti-resorptives may impair bone quality.
The rapidly changing area requires re-assessment of drugs and their interaction with fracture healing in the
2009 Elsevier Inc. All rights reserved.
opportunity to intervene in one half of future hip fracture cases. Pharmacological intervention at this “signal” fracture stage has the
A recent study of the global burden of osteoporotic fractures
potential to halve future fracture incidence, including hip fractures,
estimated that 9 million new osteoporotic fractures occurred during
within 3 years treatment, contingent upon good persistence and
the year 2000. The number of individuals suffering from the
compliance with treatment Thus, in a relatively short time frame,
consequences of osteoporotic fractures in the year 2000 was
up to one quarter of hip fractures could be averted in addition to
conservatively estimated to be 50 million worldwide A previous
substantial numbers of fractures at other skeletal sites. Health
study from the same authors, based upon data from 1990, estimated
economic assessments have demonstrated such intervention to be
the global prevalence of hip fracture with disability at 4.5 million
highly cost-effective which has resulted in endorsement of
patients , which corresponded to 1.4% of the burden of disease
secondary fracture prevention by Health Technology Appraisal
amongst women in the established market economies. An ongoing
demographic shift within the worldwide human population is fuelling
Accordingly, this provides the orthopaedic surgeon with an
an epidemic of fragility fractures. Currently, 323 million people
opportunity to play a central role in preventing future fracture.
worldwide are aged over 65 years, a figure which is predicted to rise
Surgical treatment of the fragility fracture and liaison regarding the
to 1.6 billion by 2050 . Consequently, the global incidence of hip
initiation of pharmaceutical treatment of the underlying osteoporosis
fracture is anticipated to reach 6.3 million by 2050, with three
should occur simultaneously. However, a concern over possible
quarters of these fractures occurring in the rapidly ageing Asian and
delayed fracture healing associated with bisphosphonates, the most
Latin American populations. Accordingly, if healthcare systems are to
commonly prescribed anti-osteoporosis treatment, and the lack of
avoid being overwhelmed by cases of elderly trauma, determined
guidelines detailing the context of this concern may discourage
efforts need to be applied worldwide to curb the rising prevalence of
surgeons from initiating secondary prevention.
fragility fracture, particularly at the hip.
A workshop was undertaken by the International Society for
Fracture predicts fracture. Two major meta-analyses have estab-
Fracture Repair (ISFR) in order to reach a consensus about the current
lished that a prior fracture at least doubles a patient's future fracture
evidence of the interaction of fracture healing with currently available
osteoporosis drugs and subsequent recommendations for secondary
Osteoporosis is a chronic disease that many patients will endure
prevention after fracture. The faculty comprised leading experts in the
for several decades, during which time they will suffer multiple
field of orthopaedic surgery, endocrinology, bone biology, biome-
fracture events. Unfortunately, osteoporosis often remains undetect-
chanics, pharmaceutics, healthcare systems and radiology.
ed or untreated until a fragility fracture occurs. Furthermore, in the
The specific goals of the ISFR workshop were
absence of a systematic approach to delivery of secondary fractureprevention, the majority of patients fail to receive treatment
1. to review the preclinical and clinical evidence of the interaction of
designed to reduce future fracture risk Accordingly, the
osteoporosis drugs and fracture healing or fixation;
delivery of secondary preventative intervention when patients
2. to review the issues around secondary prevention of fragility
present with fragility fracture at any skeletal site provides an
fractures, including long-term management;
8756-3282/$ – see front matter 2009 Elsevier Inc. All rights reserved. doi:
3. to discuss what clinical healthcare systems are required for
4. to identify research questions that need to be addressed to
facilitate more effective secondary prevention.
Clinical observations indicate that fragility fractures heal despite
the abnormality of bone remodelling in osteoporosis. There is no clearevidence yet as to whether complications during the course of healingare attributable to implant anchorage problems in osteoporotic boneor to possibly delayed healing in elderly patients. In animal models offracture, fracture healing takes longer in older animals Thereis conflicting evidence as to whether ovariectomy adds an additionalimpediment to healing. Some animal studies show deficient healing,especially in the early response [], and some do not . Differences in the timing of ovariectomy, age of the animals anddietary factors make comparisons and conclusions difficult.
The seemingly normal fracture healing potential in patients with
compromised bone structure and turnover can be explained by the
Fig. 1. Illustration of the main consequences of common osteoporosis drugs for fracture
different pathways of fracture repair and bone remodelling. Fracture
repair involves different stages of tissue differentiation that resembleaspects of embryological skeletal development Recently, the role
ties but did not improve mechanical parameters such as strength .
of osteoclasts in fracture repair has begun to be elucidated. The initial
To date, there are no reported suggestions of negative effects on
inflammatory phase and subsequent bone formation during the repair
fracture healing from PTH treatment.
phase are largely osteoclast independent, whereas the coupled
A newer anti-osteoporosis drug, strontium ranelate, showed no
remodelling of woven bone to lamellar bone during the remodelling
effect on fracture healing in the one animal study (in rats) published
phase at the end of fracture repair does depend on osteoclast activity.
In addition to PTH, some interesting anabolic drugs are currently
being developed. However, while animal models are appropriate forexploring mechanisms, underlying pathophysiology and specific
It is expected that anabolic agents used to treat osteoporosis would
biological hypotheses, they do not always accurately predict human
have a beneficial effect on fracture healing. However, most patients
treatment efficacy and preclinical findings need to be confirmed
who need treatment for osteoporosis will currently receive anti-
catabolic agents, and it is important to know whether this may haveany disadvantage for the healing of incident fractures.
Numerous animal experiments have addressed the interaction
between drugs used for osteoporosis treatment and different aspects
Biomechanical tests and clinical experience have shown that
of fracture healing (see and ) . However, it remains
implant anchorage is impaired in osteoporotic bone. In animal
unclear to what extent the findings can be extrapolated to humans
studies, implants failed earlier (via cut-out or cut-through) in
due to the known limitations of animal models
compromised bone structures than in healthy bone Osteopo-
There is no evidence in preclinical studies that anti-catabolic drugs
rosis drugs can improve implant fixation. This was shown in a
impair the restoration of mechanical integrity, irrespective of when
variety of animal experiments using different types of systemic or
they are administered or their mechanism of action, despite the fact
locally applied bisphosphonates This effect has been repro-
that they may delay remodelling Several animal experiments
duced in a patient level 1 study utilizing an external fixator for
have shown that different anti-catabolic drugs lead to larger callus of
treatment of proximal femur fractures. Extraction torque was
increased mechanical stiffness and strength. However, it is not clear if
significantly higher in patients treated with bisphosphonate .
there is a critical upper limit of callus stiffness and strength with
Both systemic and local peri-operative treatment with bispho-
respect to the strength of the adjacent intact bone. In a comparative
sphonates have been shown to improve the fixation of total knee
study in ovariectomized rats, Cao et al. found no major effect of
replacements, measured as a reduction of the postoperative
raloxifene and oestrogen on fracture healing responses. Alendronate
did not interfere with initial union but led to increased callus size anddecreased remodelling. However ultimate load and stiffness at16 weeks post fracture was highest in the alendronate group. Although
most fractures heal by secondary healing via external callus formation,
Classification of osteoporosis drugs based on their mode of action and their currentlyknown consequences for fracture healing.
it has been suggested bisphosphonates might have an effect on (callus-free) direct fracture healing . Direct healing in a mechanically rigid
fixation relies on osteoclastic activity for the remodelling of the
fracture surfaces. However, neither preclinical nor clinical data are
available that support the theoretical concerns. The clinical relevance
seems limited since absolute stability and subsequent possible
primary fracture healing without callus formation is not the goal of
today's fracture treatment in osteoporotic patients
In rodents, intermittent PTH stimulated fracture healing , with
doses as low as 10 μg/kg/day having a positive effect . In primates,
Increased rate of remodellingIncreased strength in animal models
larger doses accelerated remodelling and improved material proper-
Improved implant anchorage was also achieved in animal
measurement of bone turnover markers (within the first week, before
experiments with PTH ], though to date no data are available
fracture healing elevates them) will give guidance .
that support these findings in humans. The reproduction of findings
There have been recent reports of femoral diaphyseal fractures in
from animal experiments in clinical studies is complicated by the fact
patients on long-term bisphosphonate treatment . Schilcher
that there is no universally accepted measure of fracture healing in
and Aspenberg calculated an incidence density for a patient on
humans. Alternatively, the rate of prospectively defined bone-related
bisphosphonate of 1/1000 per year (95% CI = 0.3–2). These subjects
complications, or measurement of function and radiological status at
are unlikely to benefit from continuation of bisphosphonate treat-
defined time points of healing, could be used
ment and may need consideration of an anabolic agent, eithersystemically (e.g. PTH) or locally. However, Schilcher and Aspenberg
concluded that “a treatment-associated incidence density of 1/1,000 is
Osteonecrosis of the jaw (ONJ) is a complex adverse event of
acceptable, considering that bisphosphonate treatment is likely to
uncertain causal mechanism associated with bisphosphonate use. It
reduce the incidence density of any fracture by 15/1000 according to a
can be defined as a non-healing extraction socket or exposed bone in
the oral cavity that does not heal after 6 weeks of appropriate therapy,sometimes with progression to sequestration associated with puru-
Clinical systems for reliably delivering secondary prevention
lent discharge into the oral cavity or onto the skin surface. ONJ ismostly reported in cancer patients receiving intravenous bispho-
Integrated secondary fracture prevention delivery systems need to
sphonate therapy and rarely in patients receiving low doses of
be tailored to individual healthcare systems. They should be
intravenous or oral bisphosphonates for non-cancer indications such
integrated into multimodal care, which includes acute geriatric and
as fracture prevention in osteoporosis A recent review
medical support, appropriate supplementation with calcium and
summarized the current knowledge: “The incidence or prevalence
vitamin D and nutrition as well as falls assessment. Comanagement of
of ONJ in patients taking bisphosphonates for osteoporosis seems to
the patient by geriatricians, rheumatologists or endocrinologists,
be very low No causal relationship has been unequivocally
gynaecologists, radiologists and general practitioners together with
demonstrated between ONJ and bisphosphonate therapy.”
allied healthcare professionals is required for effective long-term careand also has the potential to increase the uptake of secondaryprevention.
Initiation of osteoporosis treatment after fracture
Recently, several international organisations, including the Inter-
national Osteoporosis Foundation, the Bone and Joint Decade and the
The evidence base for prevention overwhelms the non-evidence-
International Society for Fracture Repair, have jointly advocated a
based concerns about the adverse consequences of pharmaceutical
systematic approach to the provision of secondary prevention as a
treatment of osteoporosis on fracture healing The choice of drug
means to close the current worldwide fragility fracture management
should take into account long-term compliance with medication
gap . Services based upon the dedicated coordinator model have
and should be in accordance with national guidelines.
been successfully implemented in many countries. A recent editorialin the orthopaedic literature titled “Time to invest in a fracture liaison
When should the first dose be given after fracture?
nurse!” recommends investment in the dedicated coordinatorapproach as a priority for all trauma units
Treatment should be initiated before discharge from the acute
fracture ward to ensure follow-up. It is important that patients are
rendered vitamin D-replete and have an adequate oral calcium intakebefore the administration of anti-catabolic drugs, both to maximize
efficacy and to avoid the risk of hypocalcaemia.
During the time that a fracture callus is actively forming bone,
• Can we develop a valid system that can monitor the progress of
there is an increased sequestration of bisphosphonates zoledronic
fracture healing and the mechanical properties in fracture repair, in
acid and pamidronate at the fracture site . Evidence for other
a way not limited by the type of fixation?
bisphosphonates is lacking, but it is likely to be a class effect. In the
• Can we define or quantify the effect of (a) ageing and (b)
recurrent fracture trial concerns have been raised that a possible loss
osteoporosis on fracture healing in humans?
of systemic efficacy may have resulted from the timing of drug
• Are there appropriate animal models to study drug and fracture
administration relative to the fracture event. If this were true, then it
healing interactions, especially in osteoporosis?
would be logical to give intravenous bolus bisphosphonate either very
• What more can be discerned about osteoporosis drugs and fracture
soon after fracture or after the major mineralisation of the callus has
occurred. Loss of efficacy due to sequestration is likely to be less of an
• Does the state of bone turnover affect the ability to heal a fracture?
issue with more frequent dosing, such as weekly or monthly oral
• Can we optimise bisphosphonate regimens so that we achieve both
bisphosphonates, as less of the total dose would be given during the
whole-skeleton protection and late fracture remodelling?
avid uptake phase. There is to date no direct evidence that initiation of
• Does the long term suppression of bone turnover have adverse
treatment should be delayed, and so the recommendation of
effects on bone quality (e.g. microcrack accumulation) and fracture
commencing as soon as practical currently stands.
risk? Does this depend on the anti-catabolic mechanism of action? Isthe type and location of fracture different after long term anti-
The response to fracture in patients already on osteoporosis treatment
• What more can be discerned about osteoporosis drugs and fracture
The occurrence of a fragility fracture while on osteoporosis
treatment does not necessarily mean that the treatment wasineffective, as it is known that fracture rates are only reduced by25–60% .
In these cases, the physician should take the opportunity to review
the osteoporosis treatment and consider whether it remains appro-
• How do we integrate the use of anti-catabolic agents with
priate or whether a change in therapy is justified. It may be that
background use of osteoporosis treatment?
• Can we demonstrate the impact of intervention strategies on
[18] Auer JA, Goodship A, Arnoczky S, Pearce S, Price J, Claes L, et al. Refining animal
models in fracture research: seeking consensus in optimising both animal welfare
fracture rates, e.g. fracture liaison services?
and scientific validity for appropriate biomedical use. BMC Musculoskelet Disord
• Is there measurable patient benefit from agents used to accelerate
[19] O'Loughlin PF, Morr S, Bogunovic L, Kim AD, Park B, Lane JM. Selection and
development of preclinical models in fracture-healing research. J Bone Joint SurgAm 2008;90(Suppl 1):79–84.
[20] McDonald MM, Dulai S, Godfrey C, Amanat N, Sztynda T, Little DG. Bolus or weekly
zoledronic acid administration does not delay endochondral fracture repair but
This manuscript focuses on an area that is rapidly changing. Even
weekly dosing enhances delays in hard callus remodeling. Bone 2008.
[21] Cao Y, Mori S, Mashiba T, Westmore MS, Ma L, Sato M, et al. Raloxifene, estrogen,
during the writing process new results, from both in preclinical and
and alendronate affect the processes of fracture repair differently in ovariecto-
clinical studies, on the interaction between several osteoporosis drugs
mized rats. J Bone Miner Res 2002;17-12:2237–46.
and fracture healing have been published. These new findings could
[22] Shapiro F. Bone development and its relation to fracture repair. The role of
mesenchymal osteoblasts and surface osteoblasts. Eur Cell Mater 2008;15:
not be integrated into this consensus statement and will be the focus
[23] Perren SM, Linke B, Schwieger K, Wahl D, Schneider E. Aspects of internal fixation
of fractures in porotic bone. Principles, technologies and procedures using lockedplate screws. Acta Chir Orthop Traumatol Cech 2005;72-2:89–97.
[24] Andreassen TT, Ejersted C, Oxlund H. Intermittent parathyroid hormone (1–34)
treatment increases callus formation and mechanical strength of healing rat
Secondary prevention is of paramount importance and should be
fractures. J Bone Miner Res 1999;14-6:960–8.
[25] Nakajima A, Shimoji N, Shiomi K, Shimizu S, Moriya H, Einhorn TA, et al.
implemented as soon as possible after a fragility fracture. The
Mechanisms for the enhancement of fracture healing in rats treated with
evidence base for prevention overwhelms concerns about possible
intermittent low-dose human parathyroid hormone (1–34). J Bone Miner Res
adverse consequences of osteoporosis treatment on fracture healing.
[26] Manabe T, Mori S, Mashiba T, Kaji Y, Iwata K, Komatsubara S, et al. Human
A tailored systematic approach that enables routine delivery of
parathyroid hormone (1–34) accelerates natural fracture healing process in the
secondary fracture prevention must be developed by individual
femoral osteotomy model of cynomolgus monkeys. Bone 2007;40-6:1475–82.
healthcare systems throughout the world. Rapid and comprehensive
[27] Cebesoy O, Tutar E, Kose KC, Baltaci Y, Bagci C. Effect of strontium ranelate on
implementation of this strategy is vital if trauma units and national
fracture healing in rat tibia. Joint Bone Spine 2007;74-6:590–3.
[28] Goldhahn J, Suhm N, S G, Blauth M, Hanson B. Influence of osteoporosis on fracture
healthcare budgets are to avoid being overwhelmed by the increasing
fixation—a systematic literature review. Osteoporos Int 2007;19-6:761-72.
[29] Aspenberg P. Drugs and fracture repair. Acta Orthop 2005;76-6:741–8. [30] Moroni A, Faldini C, Hoang-Kim A, Pegreffi F, Giannini S. Alendronate improves
screw fixation in osteoporotic bone. J Bone Joint Surg Am 2007;89-1:96–101.
[31] Hilding M, Aspenberg P. Local peroperative treatment with a bisphosphonate
improves the fixation of total knee prostheses: a randomized, double-blind
[1] Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability
radiostereometric study of 50 patients. Acta Orthop 2007;78-6:795–9.
associated with osteoporotic fractures. Osteoporos Int 2006;17-12:1726–33.
[32] Hilding M, Aspenberg P. Postoperative clodronate decreases prosthetic migration:
[2] Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality and
4-year follow-up of a randomized radiostereometric study of 50 total knee
disability associated with hip fracture. Osteoporos Int 2004;15-11:897–902.
patients. Acta Orthop 2006;77-6:912–6.
[3] Dennison E, Mohamed MA, Cooper C. Epidemiology of osteoporosis. Rheum Dis
[33] Skripitz R, Aspenberg P. Implant fixation enhanced by intermittent treatment with
parathyroid hormone. J Bone Joint Surg Br 2001;83-3:437–40.
[4] Kanis JA, Johnell O, De Laet C, Johansson H, Oden A, Delmas P, et al. A meta-analysis
[34] Goldhahn J, Mitlak B, Aspenberg P, Kanis J, Rizzoli R, Reginster J-Y. Critical issues in
of previous fracture and subsequent fracture risk. Bone 2004;35-2:375–82.
translational and clinical research for the study of new technologies to enhance
[5] Klotzbuecher CM, Ross PD, Landsman PB, Abbott 3rd TA, Berger M. Patients with
bone repair. J Bone Joint Surg (Am) 2008;90(Suppl 1):43–7.
prior fractures have an increased risk of future fractures: a summary of the
[35] Khosla S, Burr D, Cauley J, Dempster DW, Ebeling PR, Felsenberg D, et al.
literature and statistical synthesis. J Bone Miner Res 2000;15-4:721–39.
Bisphosphonate-associated osteonecrosis of the jaw: report of a task force of the
[6] Giangregorio L, Papaioannou A, Cranney A, Zytaruk N, Adachi JD. Fragility fractures
American Society for Bone and Mineral Research. J Bone Miner Res 2007;22-10:
and the osteoporosis care gap: an international phenomenon. Semin Arthritis
[36] Cartsos VM, Zhu S, Zavras AI. Bisphosphonate use and the risk of adverse jaw
[7] Elliot-Gibson V, Bogoch ER, Jamal SA, Beaton DE. Practice patterns in the diagnosis
outcomes: a medical claims study of 714,217 people. J Am Dent Assoc 2008;139-1:
and treatment of osteoporosis after a fragility fracture: a systematic review.
[37] Grbic JT, Landesberg R, Lin SQ, Mesenbrink P, Reid IR, Leung PC, et al. Incidence of
[8] Seeman E, Compston J, Adachi J, Brandi ML, Cooper C, Dawson-Hughes B, et al.
osteonecrosis of the jaw in women with postmenopausal osteoporosis in the
Non-compliance: the Achilles' heel of anti-fracture efficacy. Osteoporos Int
health outcomes and reduced incidence with zoledronic acid once yearly pivotal
fracture trial. J Am Dent Assoc 2008;139-1:32–40.
[9] King AB, Saag KG, Burge RT, Pisu M, Goel N. Fracture Reduction Affects Medicare
[38] Rizzoli R, Burlet N, Cahall D, Delmas PD, Eriksen EF, Felsenberg D, et al.
Economics (FRAME): impact of increased osteoporosis diagnosis and treatment.
Osteonecrosis of the jaw and bisphosphonate treatment for osteoporosis. Bone
Osteoporos Int 2005;16-12:1545–57.
[10] Meyer Jr RA, Tsahakis PJ, Martin DF, Banks DM, Harrow ME, Kiebzak GM. Age
[39] Petrella RJ, Jones TJ. Do patients receive recommended treatment of osteoporosis
and ovariectomy impair both the normalization of mechanical properties and
following hip fracture in primary care? BMC Fam Pract 2006;7:31.
the accretion of mineral by the fracture callus in rats. J Orthop Res 2001;19-3:
[40] Majumdar SR, Johnson JA, Lier DA, Russell AS, Hanley DA, Blitz S, et al. Persistence,
reproducibility, and cost-effectiveness of an intervention to improve the quality of
[11] Lill CA, Hesseln J, Schlegel U, Eckhardt C, Goldhahn J, Schneider E. Biomechanical
osteoporosis care after a fracture of the wrist: results of a controlled trial.
evaluation of healing in a non-critical defect in a large animal model of
osteoporosis. Journal of Orthopaedic Research 2003;21-5:836–42.
[41] Amanat N, McDonald M, Godfrey C, Bilston L, Little D. Optimal timing of a single
[12] Meyer Jr RA, Desai BR, Heiner DE, Fiechtl J, Porter S, Meyer MH. Young, adult,
dose of zoledronic acid to increase strength in rat fracture repair. J Bone Miner Res
and old rats have similar changes in mRNA expression of many skeletal genes
after fracture despite delayed healing with age. J Orthop Res 2006;24-10:
[42] O'Donnell S, Cranney A, Wells GA, Adachi JD, Reginster JY. Strontium ranelate for
preventing and treating postmenopausal osteoporosis. Cochrane Database Syst
[13] Xu SW, Yu R, Zhao GF, Wang JW. Early period of fracture healing in ovariectomized
rats. Chin J Traumatol 2003;6-3:160–6.
[43] Cranney A, Wells G, Willan A, Griffith L, Zytaruk N, Robinson V, et al. Meta-
[14] Namkung-Matthai H, Appleyard R, Jansen J, Hao Lin J, Maastricht S, Swain M, et al.
analyses of therapies for postmenopausal osteoporosis. II. Meta-analysis of
Osteoporosis influences the early period of fracture healing in a rat osteoporotic
alendronate for the treatment of postmenopausal women. Endocr Rev 2002;23-
[15] Melhus G, Solberg LB, Dimmen S, Madsen JE, Nordsletten L, Reinholt FP.
[44] Wells GA, Cranney A, Peterson J, Boucher M, Shea B, Robinson V, et al. Alendronate
Experimental osteoporosis induced by ovariectomy and vitamin D deficiency
for the primary and secondary prevention of osteoporotic fractures in postmen-
does not markedly affect fracture healing in rats. Acta Orthop 2007;78-3:
opausal women. Cochrane Database Syst Rev 2008;1:CD001155.
[45] Ivaska KK, Gerdhem P, Akesson K, Garnero P, Obrant KJ. Effect of fracture on bone
[16] Gerstenfeld LC, Cullinane DM, Barnes GL, Graves DT, Einhorn TA. Fracture healing
turnover markers: a longitudinal study comparing marker levels before and after
as a post-natal developmental process: molecular, spatial, and temporal aspects of
injury in 113 elderly women. J Bone Miner Res 2007;22-8:1155–64.
its regulation. J Cell Biochem 2003;88-5:873–84.
[46] Lenart BA, Lorich DG, Lane JM. Atypical fractures of the femoral diaphysis in
[17] Egermann M, Goldhahn J, Schneider E. Animal models for fracture treatment in
postmenopausal women taking alendronate. N Engl J Med 2008;358-12:
osteoporosis. Osteoporos Int 2005;16(Suppl 2):S129–38.
[47] Goh SK, Yang KY, Koh JS, Wong MK, Chua SY, Chua DT, et al. Subtrochanteric
insufficiency fractures in patients on alendronate therapy: a caution. J Bone Joint
Orthopaedic Section, Department of Clinical and Experimental Medicine,
[48] Schilcher J, Aspenberg P. Incidence of stress fractures of the femoral shaft in
women treated with bisphosphonate. Acta Orthop 2009:1–3.
[49] Bouxsein ML, Kaufman J, Tosi L, Cummings S, Lane J, Johnell O. Recommendations
for optimal care of the fragility fracture patient to reduce the risk of futurefracture. J Am Acad Orthop Surg 2004;12-6:385–95.
Institute of Orthopaedics and Musculoskeletal Science, UCL,
[50] Larsson S. Time to invest in a “fracture liaison nurse”! Injury 2007;38-11:1225–6.
Royal National Orthopaedic Hospital, Stanmore, United Kingdom
on behalf of the ISFR working group drugs and fracture repair1
AO Clinical Priority Program Fracture Fixation in Osteoporotic Bone
1Members of the ISFR working group drugs and fracture repair
The Children's Hospital at Westmead, New South Wales, Australia
(in alphabetical order): Aspenberg Per, Sweden; Augat Peter,
Germany; Bavonratanavech Suthorn, Thailand; Bostrom Mathias,
USA; Chehade Mellick, Australia; Chenu Chantal, United Kingdom;
Faculty of Education Health and Sciences, University of Derby,
Claes Lutz, Germany; Dunstan Colin, Australia; Falb Dean, USA
(Stryker Biotech); Fazzalari Nicola, Australia; Findlay David, Australia;Friedlaender Gary, USA; Genant Harry, USA; Gilchrist Nigel, Australia;
Goldhahn Jörg, Switzerland; Goodship Allen, UK; Hoang-Kim Amy,
Bone and Joint Research Laboratory, SA Pathology and Hanson Institute,
Italy; Hooper Michael, Australia; Inderjeeth Charles, Australia;
Little David, Australia; Marsh David, United Kingdom; Matsushita
Takashi, Japan; Mitchell Paul, United Kingdom; Mori Satoshi, Japan;
Moroni Antonio, Italy; Parkinson Ian, Australia; Phipps Roger, USA
Department of Medicine, Faculty of Medical and Health Sciences,
(Sanofi- Aventis/P&G); Pohl Tony, Australia; Reid Ian, New Zealand;
University of Auckland, Auckland, New Zealand
November 19, 2008 Use of Antipsychotics in Children Is Criticized WASHINGTON — Powerful antipsychotic medicines are being used far too cavalierly in children, and federal drug regulators must do more to warn doctors of their substantial risks, a panel of federal drug experts said Tuesday. More than 389,000 children and teenagers were treated last year with Risperdal, one of five popul
What Schools Need to Know About Preventing the Spread of FLU? About Flu Influenza, commonly called “the flu,” is a contagious respiratory illness caused by influenza viruses. Infection with influenza viruses can result in illness ranging from mild to severe and to life-threatening complications. Five hundred out of 100,000 children with high-risk conditions (such as heart disease or ast
 j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / b o n e
Evidence for anti-osteoporosis therapy in acute fracture situations—Recommendations
of a multidisciplinary workshop of the International Society for Fracture Repair
The International Society for Fracture Repair convened a multidisciplinary workshop to assess the current
evidence around the interaction between anti-osteoporosis drugs and the healing of incident fractures, with
a view to making recommendations for clinical practice. The consensus was that there is no evidence-based
reason to withhold anti-resorptive therapy while a fracture heals, whether or not the patient was taking such
therapy when the fracture occurred. The workshop also considered existing models of service provision for
secondary prevention and concluded that the essential ingredient for reliable delivery is the inclusion of a
dedicated coordinator role. Several unresolved issues were defined as subjects for further research, including
the question of whether continuous long-term administration of anti-resorptives may impair bone quality.
j o u r n a l h o m e p a g e : w w w. e l s ev i e r. c o m / l o c a t e / b o n e
Evidence for anti-osteoporosis therapy in acute fracture situations—Recommendations
of a multidisciplinary workshop of the International Society for Fracture Repair
The International Society for Fracture Repair convened a multidisciplinary workshop to assess the current
evidence around the interaction between anti-osteoporosis drugs and the healing of incident fractures, with
a view to making recommendations for clinical practice. The consensus was that there is no evidence-based
reason to withhold anti-resorptive therapy while a fracture heals, whether or not the patient was taking such
therapy when the fracture occurred. The workshop also considered existing models of service provision for
secondary prevention and concluded that the essential ingredient for reliable delivery is the inclusion of a
dedicated coordinator role. Several unresolved issues were defined as subjects for further research, including
the question of whether continuous long-term administration of anti-resorptives may impair bone quality.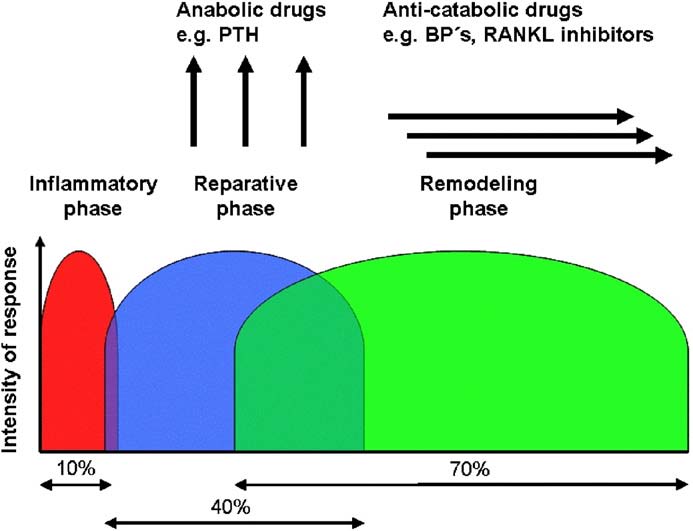 3. to discuss what clinical healthcare systems are required for
4. to identify research questions that need to be addressed to
facilitate more effective secondary prevention.
3. to discuss what clinical healthcare systems are required for
4. to identify research questions that need to be addressed to
facilitate more effective secondary prevention.