La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Doi:10.1016/j.fertnstert.2006.08.024
Aging and infertility in women The Practice Committee of the American Society for Reproductive Medicine
American Society for Reproductive Medicine, Birmingham, Alabama
BACKGROUND
addition to ovaries with average to low follicle numbers and
Female fertility begins to decline many years prior to the
onset of menopause despite continued regular ovulatory cy-cles. Although there is no strict definition of advanced re-
PHYSIOLOGY OF REPRODUCTIVE AGING
productive age in women, infertility becomes more pro-
The age at which menopause occurs reflects near complete
nounced after the age of 35. A classic report on the effect of
depletion of the ovarian follicular pool Subtle changes in
female age on fertility found that the percentage of women
early follicular phase serum concentrations of FSH (in-
not using contraception who remained childless rose steadily
crease) and inhibin B (decrease) precede changes in men-
according to their age at marriage: 6% at age 20 to 24, 9% at
strual regularity and ovarian steroid secretion. Risk factors
age 25 to 29, 15% at age 30 to 34, 30% at age 35 to 39, and
for early loss of ovarian reserve include smoking, family
64% at age 40 to 44 Similarly, a sharp decline in
history of premature ovarian failure, significant ovarian pa-
pregnancy rate with advancing female age is noted with
thology, and previous ovarian surgery.
donor insemination studies (which control for fertility of themale partner and coital frequency) and with assisted
The age-associated decline in female fecundity and in-
reproductive technologies (ART) including in vitro fertiliza-
creased risk of spontaneous abortion are largely attributable
tion (IVF). The risk of spontaneous abortion increases with
to abnormalities in the oocyte. The meiotic spindle in the
female age According to the 1999 Assisted Reproductive
oocytes of older women frequently exhibits abnormalities in
Technology Success Rates, the percentage of clinical preg-
chromosome alignment and microtubular matrix composi-
nancies (gestational sac as imaged with sonography) that
tion Higher rates of single chromatid abnormalities in
failed to result in a live birth rose according to the woman’s
oocytes as well as aneuploidy in preimplantation em-
age: 14% for patients under age 35, 19% at age 35 to 37,
bryos and ongoing pregnancies, are observed in older
25% at age 38 to 40, and 40% after age 40
women. The higher rate of aneuploidy is a major cause ofincreased spontaneous abortion and decreased live birth rates
A recent review of studies on the effects of male age on
in women of advanced reproductive age.
semen quality and fertility concluded that increasing age isassociated with a decline in semen volume, sperm motility,
The prevalence of uterine pathology, such as fibroids and
and sperm morphology, but not sperm concentration
endometrial polyps, increases with age yet there is little
There is some decline in male fertility with age, particularly
evidence that uterine factors have a significant impact on
over the age of 50, but the results of many of these studies
age-related infertility. Age does not appear to have a signif-
are confounded by female partner age. There is no absolute
icant effect on morphological or histological responses of the
age at which men cannot father a child. Fertility is thus more
uterus to steroid stimulation A recent study has not
related to the age of the female than the male partner.
found an age-related decline in ART cycle delivery rateswhen oocyte donation is performed
The average age of childbearing has increased over the
past three decades as more women have pursued higher
EVALUATION
education and careers and postponed marriage. Concur-
Tests to evaluate infertility provide information about cur-
rently, a large cohort of women born during the “Baby
rent fertility but do not predict when the onset of age-related
Boom” (1946 –1964) have reached their late reproductive
infertility will occur. Although infertility is commonly de-
years, resulting in more women in this age group seeking
fined as the inability to conceive after one year of unpro-
assistance for infertility. Not all women of advanced repro-
tected intercourse, normal older women may take longer
ductive age who wish to conceive experience infertility.
than one year to conceive. Therefore, earlier evaluation of
Those older women who do present to physicians for infer-
infertility is warranted in women over the age of 35. The
tility may have other fertility problems (e.g., male factor) in
consequences of undiagnosed infertility factors can be moredetrimental to women who have limited time to achieve asuccessful pregnancy. In addition to infertility testing, the
Committee Opinion Under revision June 2006.
preconception medical evaluation should also include
screening for significant medical disorders such as hyperten-
sion and diabetes, which are more frequent in older women.
Correspondence to: Practice Committee, American Society for Repro-
In women 40 and older, it is advisable to perform mammog-
ductive Medicine, 1209 Montgomery Highway, Birmingham, Alabama35216.
raphy prior to attempting pregnancy. S248 Fertility and Sterilityா Vol. 86, Suppl 4, November 2006
Copyright 2006 American Society for Reproductive Medicine, Published by Elsevier Inc.
The infertility evaluation in women of advanced repro-
to gonadotropins In the future, transvaginal ultra-
ductive age should include an assessment of ovarian reserve.
sound may be an effective way of estimating ovarian reserve.
The term ovarian reserve describes a woman’s reproductive
Currently it seems reasonable to test ovarian reserve by
potential with respect to ovarian follicle number and oocyte
using day 3 FSH and estradiol or the CCCT in all infertile
quality. The measurement of serum basal FSH and estradiol
women age 35 and older who desire pregnancy. Ovarian
on day 3 of the menstrual cycle is often used to test for
reserve testing may be considered in patients under age 35 with
ovarian reserve. FSH and estradiol should be measured in the
a solitary ovary, history of ovarian surgery, poor response to
early follicular phase because accelerated follicular develop-
exogenous gonadotropins, exposure to chemotherapeutic agents
ment may be associated with reproductive aging. Elevated
or ionizing radiation, and unexplained infertility.
FSH and estradiol levels are independent predictors of poorprognosis in older women Common criteria fornormal ovarian reserve are an early follicular phase FSH
COUNSELING
level of Ͻ10 mIU/mL and an estradiol level of Ͻ80 pg/mL.
Preconception counseling should include a discussion of the
Higher cutoff values for FSH have been reported (as high as
increased risks of aneuploidy, spontaneous abortion, and
20 to 25 mIU/mL for FSH) because of the use of different
obstetric complications such as delivery by cesarean section,
FSH assay reference standards The normal range for
hypertension, and gestational diabetes associated with
FSH ideally should be determined in a normal fertile popu-
increasing maternal age. The rate of all clinically significant
lation by each laboratory. In the event that such data are not
cytogenetic abnormalities in live births increases from about
available, the laboratory’s stated upper limit for the follicular
1/500 for women under 30 to 1/270 at age 30, 1/80 at age 35,
phase can be used as an arbitrary and imperfect cutoff to
Counseling after ovarian reserve testing should include a
The clomiphene citrate challenge test (CCCT), which is
discussion of the results. While they may predict a lower
another test of ovarian reserve, is performed by measuring a
pregnancy rate, abnormal ovarian reserve test results do not
day 3 FSH, administering clomiphene citrate 100 mg orally
preclude the possibility of pregnancy and should not be pre-
on cycle days 5 to 9, and then measuring FSH on cycle day
sented to patients as absolute. Likewise, ovarian reserve testing
10 The test is considered to be abnormal if either
alone may yield falsely reassuring results, as advanced maternal
the day 3 or the day 10 FSH is above the threshold value for
age and ovarian reserve test results are independent predictors
of infertility. Both should be used when counseling couplesregarding their chances for conception
Women with abnormal basal FSH, estradiol, or CCCT
have lower live birth rates with ovulation induction and
TREATMENT
intrauterine insemination Women with dimin-ished ovarian reserve also experience decreased responses to
Treatment options for age-related infertility include con-
ovulation induction, require higher doses of gonadotropin,
trolled ovarian hyperstimulation with intrauterine insemina-
have higher IVF cycle cancellation rates, and experience
tion (COH/IUI), IVF, and oocyte donation. Except for oo-
lower pregnancy rates through IVF In a general
cyte donation, these treatments are intended to accelerate the
infertility population, an abnormal CCCT predicts that a
time to conception rather than directly affect oocyte or
successful pregnancy will be achieved about 5% of the time
embryo quality. Expectant management, which should be
A single elevated day 3 FSH value connotes a poor
reserved for couples who do not desire medical intervention,
prognosis, even when values in subsequent cycles are normal
is also considered a treatment option but is less likely to
result in pregnancy in women of advanced reproductive ageCOH/IUI consists of gonadotropins administered to
Other tests of ovarian reserve under study include circu-
initiate growth and ovulation of multiple follicles in con-
lating inhibin B levels, the gonadotropin-releasing hormone
junction with the placement of washed sperm in the uterine
agonist test, and small antral follicle count by ultrasound.
Women with decreased ovarian responsiveness to gonado-
COH/IUI has limited efficacy for women over 40 with
tropin may have decreased serum inhibin B levels even when
otherwise unexplained infertility, yielding a per cycle deliv-
FSH levels are normal This finding suggests that in-
ery rate of 5% or less (range 1.4% to 5.2%) This
hibin B may be a more sensitive marker of ovarian reserve
compares with a live birth rate per cycle of 17% to 22% for
than FSH. However, routine testing for serum inhibin B
women under 35 and 8% to 10% for women aged 35 to 40
levels is not recommended at this time due to limited avail-
There have been no studies comparing COH/
ability of reliable assays and conflicting data regarding its
IUI with IVF. Unfortunately, most reports have been retro-
prognostic value The gonadotropin-releasing hormone
spective case series or cohort studies that would be expected
agonist challenge test is not recommended for routine clin-
to overestimate treatment effectiveness.
ical use because of limited data on its prognostic value. Thenumber of small antral follicles visible on transvaginal ul-
The presence of male factor, tubal disease, endometriosis,
trasound appears to correlate directly with ovarian response
or pelvic adhesions would argue for proceeding directly to
FERTILITY & STERILITYா
IVF in women of advanced reproductive age. Pregnancy
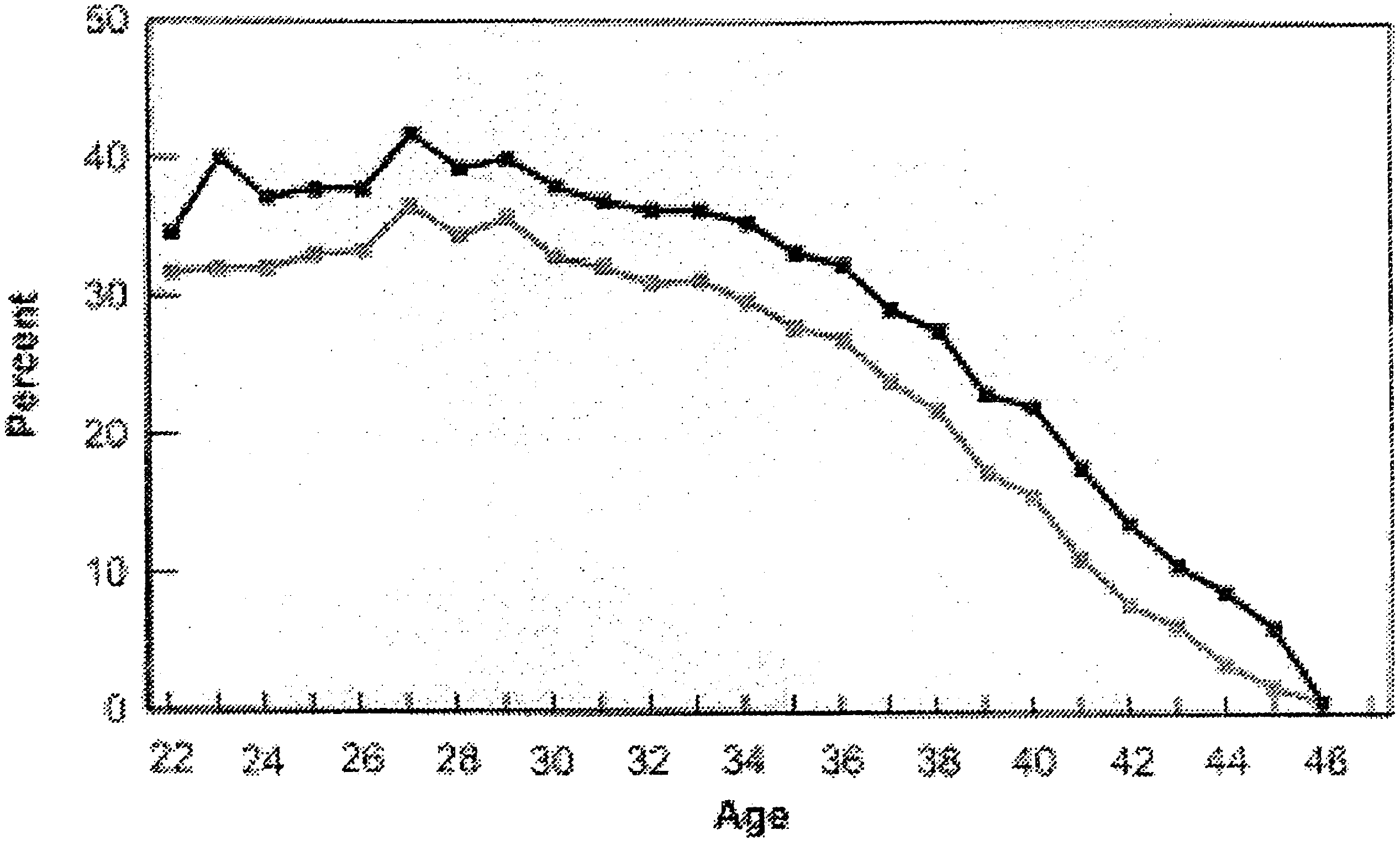
rates from IVF are generally higher than from COH/IUI butalso decline significantly with age. According to the 1999Embryo implantation rates as a function of Assisted Reproductive Technology Success Rates, live birth
female age
rates per cycle were 32.2% in women under 35, 26.2% in
Implantation rate
women aged 35 to 37, 18.5% in women aged 38 to 40, 9.7%in women aged 41 to 42, and approximately 5% in women
In a recent multicenter review of 431 initiated IVF cycles
in women Ն41 years, there were no clinical pregnancies in
women Ն45 years and no deliveries in women Ն44 years of
Reprinted with permission (Fertil Steril 1996;65:783–
age . This age-related decline in IVF success is related to
decreased ovarian responsiveness to gonadotropins and, more
Source: Centers for Disease Control and Prevention,
importantly, to a marked decline in embryo implantation rates
American Society for Reproductive Medicine, Society
Embryonic aneuploidy is likely the major reason for
for Assisted Reproductive Technology, RESOLVE. 1999 Assisted Reproductive Technology Success
Rates. Atlanta, GA. Centers for Disease Control and
The following alternative approaches have been described
for IVF treatment in women with decreased ovarian reserve:
ASRM Practice Committee. Aging and infertility in women. Fertil Steril2006.
1. Microdose GnRH agonist flare protocol or other flare
2. Use of a GnRH antagonist with gonadotropins. 3. Low-dose GnRH agonist suppression before gonadotro-
Unfortunately, there are no randomized trials to compare
the relative efficacy of these approaches. Exclusion of ane-
uploid embryos with preimplantation genetic diagnosis
5. Use of estrogen or oral contraceptives in the cycle prior to
(PGD) may lower the spontaneous abortion rate in IVF
cycles However, the technique is expensive and is notyet widely available. Its role in the treatment of age-relatedinfertility has yet to be defined.
Nuclear (germinal vesicle) transfer is an experimental
Pregnancy and live birth rates for ART cycles
technique in which the nucleus from the oocyte of an older
using fresh, nondonor eggs or embryos, by female
woman is transferred to the enucleated oocyte of a younger
age, 1999. Data from reference 4. Gray line ϭ live
woman. The safety and efficacy of this technique is currently
birth rate; solid line ϭ pregnancy rate. ASRM.
Aging and infertility in women. Fertil Steril 2002. Source: Centers for Disease Control and
No treatment other than oocyte donation has been shown
Prevention, American Society for Reproductive
to be effective for women over 40 and for those with com-
Medicine, Society for Assisted Reproductive
promised ovarian reserve. Although the resulting child will
not be biologically related to the birth mother, oocyte dona-
reproductive technology success rates. Atlanta,
tion yields the highest live birth rate of any ART treatment.
GA: Centers for Disease Control and Prevention,
It is the treatment of choice for age-related infertility not
successfully addressed by other methods. Pregnancy rateswith oocyte donation are dependent on the age of the donorrather than the recipient.
● A relatively large group of women is experiencing age-
related infertility due to social trends that lead to deferredchildbearing and to the current age of the “Baby Boom”generation.
● Age-related infertility is due to oocyte abnormalities and
● Clinical tests to estimate ovarian reserve include FSH and
estradiol levels in the early follicular phase (e.g., day 3) or
ASRM Practice Committee. Aging and infertility in women. Fertil Steril 2006.
a clomiphene citrate challenge test. Aging and infertility in women
● Evaluation and treatment of infertility should not be de-
outcome in patients undergoing in vitro fertilization. Fertil Steril
17. Navot D, Rosenwaks Z, Margalioth EJ. Prognostic assessment of fe-
Treatment of infertility when the cause is limited to de-
male fecundity. Lancet 1987;2:645–7.
creased ovarian reserve is empirical at present except for
18. Tanbo T, Dale PO, Lunde O, Norman N, Abyholm T. Prediction of
response to controlled ovarian hyperstimulation: a comparison of basaland clomiphene citrate-stimulated follicle-stimulating hormone levels. Acknowledgments: This report was developed under the direction of the
Practice Committee of the American Society for Reproductive Medicine
19. Scott RT, Leonardi MR, Hofmann GE, Illions EH, Neal GS, Navot D.
as a service to its members and other practicing clinicians. While this
A prospective evaluation of clomiphene citrate challenge test screening
report reflects appropriate management of a problem encountered in the
of the general infertility population. Obstet Gynecol 1993;82:539 – 44.
practice of reproductive medicine, it is not intended to be the only
20. Buyalos RP, Daneshmand S, Brzechffa PR. Basal estradiol and follicle-
approved standard of practice or to dictate an exclusive course of
stimulating hormone predict fecundity in women of advanced repro-
treatment. Other plans of management may be appropriate, taking into
ductive age undergoing ovulation induction therapy. Fertil Steril 1997;
account the needs of the individual patient, available resources and
institutional or clinical practice limitations. This report was approved by
21. Toner JP, Philput CB, Jones GS, Muasher SJ. Basal follicle stimulating
the Practice Committee of the American Society for Reproductive Med-
hormone level is a better predictor of in vitro fertilization performance
icine in November 2001 and the Board of Directors of the American
than age. Fertil Steril 1991;55:784 –91.
Society for Reproductive Medicine in January 2002.
22. Scott RT, Opsahl MS, Leonardi MR, Neall GS, Illions EH, Navot D.
Life table analysis of pregnancy rates in a general infertility populationrelative to ovarian reserve and patient age. Hum Reprod 1995;10:1706 –10. REFERENCES
23. Scott RT Jr, Hofmann GE, Oehninger S, Muasher SJ. Intercycle vari-
ability of day 3 follicle-stimulating hormone level and its effect on
1. Menken J, Trussell J, Larsen U. Age and infertility. Science 1986;233:
stimulation quality in in vitro fertilization. Fertil Steril 1990;54:297–302.
24. Martin JS, Nisker JA, Tummon IS, Daniel SA, Auckland JL, Feyles V.
2. Schwartz D, Mayaux MJ. Female fecundity as a function of age: results
Future in vitro fertilization pregnancy potential of women with variably
of artificial insemination in 2193 nulliparous women with azoospermic
elevated day 3 follicle-stimulating hormone levels. Fertil Steril 1996;
husbands. Federation CECOS. N Engl J Med 1982;306:404 – 6.
3. Smith KE, Buyalos RP. The profound impact of patient age on preg-
25. Seifer DB, Scott RT Jr, Bergh PA, Abrogast LK, Friedman CI, Mack
nancy outcome after early detection of fetal cardiac activity. Fertil Steril
CK, et al. Women with declining ovarian reserve may demonstrate a
decrease in day 3 serum inhibin B before a rise in day 3 follicle-
4. Centers for Disease Control and Prevention, American Society for
stimulating hormone. Fertil Steril 1999;72:63–5.
Reproductive Medicine, Society for Assisted Reproductive Technol-
26. Corson SL, Gutmann J, Batzer FR, Wallace H, Klein N, Soules MR.
ogy, RESOLVE. 1999 Assisted reproductive technology success rates.
Inhibin-B as a test of ovarian reserve for infertile women. Hum Reprod
Atlanta, GA: Centers for Disease Control and Prevention, 2001.
5. Kidd SA, Eskenazi B, Wyrobek AJ. Effects of male age on semen
quality and fertility: a review of the literature. Fertil Steril 2001;75:
27. Chang MY, Chiang CH, Hsieh TT, Soong YK, Hsu KH. Use of the
antral follicle count to predict the outcome of assisted reproductive
6. Faddy MJ, Gosden RG, Gougeon A, Richardson SJ, Nelson JF. Accel-
technologies. Fertil Steril 1998;69:505–10.
erated disappearance of ovarian follicles in mid-life: implications for
28. Frattarelli JL, Lauria-Costab DF, Miller BT, Bergh PA, Scott RT. Basal
forecasting menopause. Hum Reprod 1992;7:1342– 6.
antral follicle number and mean ovarian diameter predict cycle cancel-
7. Battaglia DE, Goodwin P, Klein NA, Soules MR. Influence of maternal
lation and ovarian responsiveness in assisted reproductive technology
age on meiotic spindle assembly in oocytes from naturally cycling
cycles. Fertil Steril 2000;74:512–7.
women. Hum Reprod 1996;11:2217–22.
29. Gilbert WM, Nesbitt TS, Danielsen B. Childbearing beyond age 40:
8. Angell RR. Aneuploidy in older women. Higher rates of aneuploidy in
pregnancy outcome in 24,032 cases. Obstet Gynecol 1999;93:9 –14.
oocytes from older women. Hum Reprod 1994;9:1199 –200.
30. Hook EB. Rates of chromosome abnormalities at different maternal
9. Benadiva CA, Kligman I, Munne S. Aneuploidy 16 in human embryos
ages. Obstet Gynecol 1981;58:282–5.
increases significantly with maternal age. Fertil Steril 1996;66:248 –55.
31. Agarwal SK, Buyalos RP. Clomiphene citrate with intrauterine insem-
10. Nagele F, O’Connor H, Davies A, Badawy A, Mohamed H, Magos A.
ination: is it effective therapy in women above the age of 35 years?
2500 outpatient diagnostic hysteroscopies. Obstet Gynecol 1996;88:
32. Pearlstone AC, Fournet N, Gambone JC, Pang SC, Buyalos RP. Ovu-
11. Noci I, Borri P, Chieffi O, Scarselli G, Biagiotti R, Moncini D, et al. Aging
lation induction in women age 40 and older: the importance of basal
of the human endometrium: a basic morphological and immunohistochem-
follicle-stimulating hormone level and chronological age. Fertil Steril
ical study. Eur J Obstet Gynecol Reprod Biol 1995;63:181–5.
12. Navot D, Drews MR, Bergh PA, et al. Age-related decline in female
33. Brzechffa PR, Buyalos RP. Female and male partner age and menotro-
fertility is not due to diminished capacity of the uterus to sustain
phin requirements influence pregnancy rates with human menopausal
embryo implantation. Fertil Steril 1994;61:97–101.
gonadotrophin therapy in combination with intrauterine insemination.
13. Hershlag A, Lesser M, Montefusco D, Lavy G, Kaplan P, Liu HC, et al.
Interinstitutional variability of follicle-stimulating hormone and estra-
34. Corsan G, Trias A, Trout S, Kemmann E. Ovulation induction com-
diol levels. Fertil Steril 1992;58:1123– 6.
bined with intrauterine insemination in women 40 years of age and
14. Smotrich DB, Widra EA, Gindoff PR, Levy MJ, Hall JL, Stillman RJ.
older: is it worthwhile? Hum Reprod 1996;11:1109 –12.
Prognostic value of day 3 estradiol on in vitro fertilization outcome.
35. Frederick JL, Denker MS, Rojas A, Horta I, Stone SC, Asch RH, et al.
Is there a role for ovarian stimulation and intra-uterine insemination
15. Frattarelli JL, Bergh PA, Drews MR, Sharara FI, Scott RT. Evaluation
after age 40? Hum Reprod 1994;9:2284 – 6.
of basal estradiol levels in assisted reproductive technology cycles.
36. Campana A, Sakkas D, Stalberg A, Bianchi PG, Comte I, Pache T, et al.
Intrauterine insemination: evaluation of the results according to the
16. Licciardi FL, Liu HC, Rosenwaks Z. Day 3 estradiol serum concentra-
woman’s age, sperm quality, total sperm count per insemination and
tions as prognosticators of ovarian stimulation response and pregnancy
life table analysis. Hum Reprod 1996;11:732– 6. FERTILITY & STERILITYா
37. Brzechffa PR, Daneshmand S, Buyalos RP. Sequential clomiphene
42. Hull MG, Fleming CF, Hughes AO, McDermott A. The age-related
citrate and human menopausal gondotrophin with intrauterine insemi-
decline in female fecundity: a quantitative controlled study of implant-
nation: the effect of patient age on clinical outcome. Hum Reprod
ing capacity and survival of individual embryos after in vitro fertiliza-
tion. Fertil Steril 1996;65:783–90.
38. Guzick DS, Carson SA, Coutifaris C, Overstreet JW, Factor-Litvak P,
43. Surrey ES, Bower J, Hill DM, Ramsey J, Surrey MW. Clinical and
Steinkampf MP, et al. Efficacy of superovulation and intrauterine
endocrine effects of a microdose GnRH agonist flare regimen admin-
insemination in the treatment of infertility. National Cooperative Re-
istered to poor responders who are undergoing in vitro fertilization.
productive Medicine Network. N Engl J Med 1999;340:177– 83.
39. Cohen MA, Chang PL, Uhler M, Legro R, Sauer MV, Lindheim SR.
44. Surrey ES, Schoolcraft WB. Evaluating strategies for improving ovar-
Reproductive outcome after sterilization reversal in women of ad-
ian response of the poor responder undergoing assisted reproductive
vanced reproductive age. J Assist Reprod Genet 1999;16:402– 4.
techniques. Fertil Steril 2000;73:667–76.
40. Ron-El R, Raziel A, Strassburger D, Schachter M, Kasterstein E,
45. Munne S, Magli C, Cohen J, Morton P, Sadowy S, Gianaroli L, et al.
Friedler S. Outcome of assisted reproductive technology in women over
Positive outcome after preimplantation diagnosis of aneuploidy in hu-
the age of 41. Fertil Steril 2000;74:471–5.
man embryos. Hum Reprod 1999;14:2191–9.
41. Munne S, Alikani M, Tomkin G, Grifo J, Cohen J. Embryo morphol-
46. Zhang J, Wang CW, Krey L, Liu H, Meng L, Blaszczyk A, et al. In
ogy, developmental rates, and maternal age are correlated with chro-
vitro maturation of human preovulatory oocytes reconstructed by ger-
mosome abnormalities. Fertil Steril 1995;64:382–91.
minal vesicle transfer. Fertil Steril 1999;71:726 –31. Aging and infertility in women
Le Mal Aigu des Montagnes Source « santé altitude en partenariat avec ARPE) Fédératio n française de la montagne et de l’escalade Commission Médicale Le Mal Aigu des Montagnes (MAM) touche à des degrés divers, toutes les personnes qui participent à des courses, trekkings ou expéditions en altitude Ses signes sont le plus souvent bénins : mal de tête, fa
 IVF in women of advanced reproductive age. Pregnancy
rates from IVF are generally higher than from COH/IUI butalso decline significantly with age. According to the 1999
Embryo implantation rates as a function of
IVF in women of advanced reproductive age. Pregnancy
rates from IVF are generally higher than from COH/IUI butalso decline significantly with age. According to the 1999
Embryo implantation rates as a function of