La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
1471-2415-7-3.fm
BMC Ophthalmology
Research article TOZAL Study: An open case control study of an oral antioxidant and omega-3 supplement for dry AMD Francis E Cangemi*
Address: Vitreo-Retinal Associates of New Jersey, 119 Prospect Street, Ridgewood, New Jersey 07450 USA
Email: Francis E Cangemi* - franciscangemi@aol.com
Received: 6 November 2006Accepted: 26 February 2007
BMC Ophthalmology 2007, 7:3
2007 Cangemi; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: The primary objective of this prospective study was to measure the change from baseline in visual function – Best-Corrected Visual Acuity (BCVA) via the Early Treatment Diabetic Retinopathy Study (ETDRS) chart, contrast sensitivity, central 10 degree visual fields and retinal imaging (angiograms and photographs) at 6 months in subjects with atrophic (dry) age-related macular degeneration treated with a targeted nutritional supplement. Methods: 37 mixed gender patients with a mean age of 76.3 +/- 7.8 years were enrolled at 5 independent study sites and received standard of care with a novel formulation of a nutritional supplement. Results were compared to a placebo cohort constructed from the literature that was matched for inclusion and exclusion criteria. A paired t-test was used to test a null hypothesis and a two-sided alpha level of 0.05 was used to determine statistical significance. Results: 76.7% of subjects receiving the nutritional supplement demonstrated stabilization or improvement of BCVA at 6 months. Subjects gained an average of 0.0541 logMAR or one-half of a line of visual acuity (VA) over the 6-month period. There was a statistically significant improvement in VA from baseline with P = .045. The results provide strong evidence that the treatment being studied produces an improvement in VA. Conclusion: Treatment with this unique nutritional supplement increased VA above the expected baseline decrease in the majority of patients in this population with dry macular degeneration. The results of the TOZAL study agree with the LAST and CARMIS studies and are predictive for positive visual acuity outcomes in the AREDS II trial. However, patients will likely require supplementation for longer than 6 months to effect changes in additional visual parameters. Background
atrophic, or non-exudative, AMD is the most common
Age-related Macular Degeneration (AMD) is a progressive
form and is characterized by progressive devitalization of
disorder associated with central vision loss and is the lead-
retinal pigment epithelium (RPE) and the formation of
ing cause of visual impairment and blindness in people
fatty deposits under the RPE known as soft drusen [1].
over the age of 60. More than 15 million Americans over
Although the underlying cause of AMD is unknown, risk
the age of 60 have AMD with an additional 50 million
factors have been defined and include age greater than 50,
Americans at risk for developing the disorder [1]. Dry,
Caucasian race, nutrition, smoking, atherosclerotic vascu-
(page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
lar disease, genetics, and sunlight exposure [1-4]. At this
The microcurrent in this study was self-administered by
time, there is no known cure for AMD. Patients not receiv-
the patient, 2 treatments each day, using an automated
ing treatment have demonstrated a loss of VA at 6 months
microcurrent stimulator with a preset current of 800
of at least 0.8 lines and up to 1.5 lines [5-7].
micro-amps at frequency settings of 292 Hz (6 minutes),30 Hz (3 minutes), 9.1 Hz (2 minutes), and 0.3 Hz (1
Multiple studies have suggested that manipulation of
minute) for a total of 12 minutes. The sham device was
nutritional factors can play a significant role in slowing
identical to the treatment device, including LED indica-
the onset or limiting the effects of AMD [8-13]. In 1996,
tors and audible tones; however, there was no electrical
Richer et al found that a broad-spectrum antioxidant and
current output. Electrical current administered at levels
mineral supplement was effective in delaying AMD-
below 1 milliamp (1,000 micro-amps) has no detectable
related vision loss, but was unable to reverse existing
vision loss [14,15]. The Age-Related Eye Disease Study(AREDS), sponsored by the National Eye Institute, dem-
MCS treatment was found to have little significant effect
onstrated that high levels of antioxidants and zinc were
on any of the efficacy endpoints and thus was abandoned.
able to reduced the risk of development of advanced AMD
Only the nutritional supplement aspect of the study is
by approximately 25% [16]. In 2004, the Lutein Antioxi-
reported and discussed here (ie, patients receiving sham
dant Supplementation Trial (LAST) demonstrated that
MCS and nutritional supplement, n = 37).
nutritional supplementation with lutein or lutein togetherwith antioxidants, vitamins, and minerals improved vis-
Each subject was scheduled for 5 visits (Figure 1). During
ual function and symptoms in patients with atrophic age-
the first visit, subjects who met the inclusion and exclu-
sion criteria (Table 1) and signed a consent to participateunderwent a comprehensive eye examination including
Nutritional supplements have become the first line of
medical and ophthalmic history, refraction, BCVA meas-
defense for clinicians in battling dry AMD. Vitamin and
ured by ETDRS (logMAR) at 4 m, biomicroscopy, intraoc-
mineral formulations are a valid therapeutic tool and are
ular lens evaluation, intraocular pressure, dilated fundus
many orders of magnitude less toxic than aspirin and
exam, fluorescein angiogram and retinal photographs,
contrast sensitivity, full threshold visual fields, and macu-lar testing (central 10° threshold visual filed). Addition-
The Taurine, Omega-3 Fatty Acids, Zinc, Antioxidant,
ally, each subject completed the Visual Function
Lutein (TOZAL) study sought to identify the potential
benefits of a novel supplement designed to limit the riskof AMD and progressive vision loss while also reducing or
During the second visit at week 1, BCVA (logMAR) and
eliminating the risk of adverse events.
contrast sensitivity were measured and the nutritionalsupplement was dispensed. The TOZAL nutritional sup-
plement formulation used in this study is outlined in
This study was approved by an independent ethics com-
Table 2. This is a novel supplement formulation and is
mittee and an independent review board and was con-
currently patent pending. Subjects were instructed to self-
ducted at five independent clinical sites. The study was
administer the oral supplements at 2 capsules 3 times per
day concurrent with food intake. Treatment compliancewas assessed at each subsequent visit via a daily patient
Study Design
This prospective, double-blind, 6-month trial enrolled 73subjects with at least 1 eye diagnosed with dry AMD. There
During the third visit at week 2, BCVA (logMAR) and con-
were 5 independent study sites: site 1 enrolled 19 patients,
site 2 enrolled 15 patients, site 3 enrolled 13 patients, site4 enrolled 12 patients, and site 5 enrolled 14 patients.
During the fourth visit at week 11, BCVA (logMAR) and
Patients were randomly assigned 1 of 2 treatment arms: 1)
contrast sensitivity were measured. In addition, retinal
microcurrent stimulation (MCS) treatment and nutri-
photographs, fluorescein angiogram, macular testing, and
tional supplement (n = 36), and 2) sham MCS and nutri-
full threshold visual fields were conducted.
The final and exit visit was at week 24 and was a repeat of
In 1998, Allen et al reported that patients with dry AMD
the first visit in addition to a compliance assessment.
treated with a combination of nutrients and microcurrentelectricity showed slowing or reversing of the progress ofAMD for most subjects [18]. (page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
Figure 1 gn Study design. (page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
Table 1: Inclusion and exclusion criteria
Inclusion Criteria• Signed written consent• Between the ages of 50 and 90, inclusive• Any race or gender• Diagnosis of nonexudative (dry) AMD in at least 1 eye having > 10 large soft drusen 63 μm in diameter, within 3,000 um of the fovea center, documented on macular exam, retinal angiography and fundus photographs• Able to understand and comply with the requirements of the trial• BCVA in the trial eye(s) of 20/32 to 20/125 inclusive as measured by ETDRS (logMAR)• Subjects must not have conditions that limit the view to the fundus (eg vitreous hemorrhage, cataracts, an epiretinal membrane). All subjects with = 2+ nuclear opacities and/or significant central opacity (PSC or ASC) > 1+ will undergo Potential Acuity Meter (PAM) testing. If the vision is = 2 lines improved on PAM over standard acuity measurement then the subject will not be eligible for the trial• Subjects must be available for a minimum trial duration of approximately 6 months• Subjects must agree to take only the nutritional supplement that is provided during this study• Subjects or eyes must not meet any of the exclusion criteriaExclusion CriteriaAny of the following excluded a subject from the trial:• Currently enrolled in an ophthalmic clinical trial• Eyes with concomitant macular or choroidal disorders other than AMD and with indefinite signs of AMD• Eyes with a diagnosis of exudative (wet) AMD with active subretinal neovascularization (SRNV) or CNV lesions requiring laser photocoagulation in the study eye• Subjects with significant ocular lens opacities causing vision decrease• Subjects with amblyopia• Subjects with optic nerve disease (neuropathy, atrophy, papilledema), unstable glaucoma as defined by intraocular pressures greater than 25 mm Hg, 3 or more glaucoma medications, C/D of 0.8 or greater and visual fields consistent with glaucoma; history of retina-vitreous surgery, degenerative myopia, active posterior intraocular inflammatory disease, chronic use of topical ocular steroid medications, vasoproliferative retinopathies (other than AMD), rhegmatogenous retinal detachment, and inherited macular dystrophies• Subjects with demand type pacemakers or epilepsy• Subjects with uncontrolled hypertension (defined as diastolic of 90 or greater and systolic of 150 or greater)• Subjects with recent history (within the previous year) of cerebral vascular disease• manifested with transient ischemic attacks (TIA's) or cerebral vascular accidents (CVA's)• Subjects with a history of AIDS• Subjects who have received any previous experimental procedure in either eye or the use of any investigational drug or treatment within 30 days prior to enrolling in the trial• Subjects who have had intraocular surgery in trial eye within 3 months prior to enrolling in the trial• Smokers or any tobacco use
Objective Measures
The primary safety variables were unexpected ocular or
The primary objective was to measure the change in BCVA
systemic findings, adverse event rate, and temporary and
from baseline to 6 months in subjects with non-exudative
permanent discontinuation. Investigators were required
macular degeneration treated with a nutritional supple-
to report any treatment-related adverse events or serious
ment. The secondary efficacy variable was objective signs
non-treatment-related adverse events and severe adverse
Table 2: Nutritional supplement formulation (page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
Adverse events included any undesirable clinical occur-
measured as visit 2 (week 1). Change from baseline was
rence in a subject whether considered related to treatment
evaluated at weeks 11 and 24. Repeated measures mixed
or not. Serious adverse events included those in which
model (Proc Mixed, SAS, 8.2) was fitted to compare mean
information suggested that treatment caused or may have
change in VA from baseline between the groups, with Visit
caused or contributed to death or serious injury including,
and Treatment-by-Visit interaction included as main
but not limited to, permanent decrease in BCVA (≥ 2
effects, baseline VA as covariate, and Eye as the within-
lines) or hospitalization. Significant adverse events
included those that required medical intervention or war-ranted discontinuation (temporary or permanent) from
A secondary analysis set was also constructed, comprised
the clinical trial. These events were non-sight-threatening
of 1 eye per patient meeting the 20/32–20/125 entrance
conditions that were determined to be device-related.
VA criteria. If both the left and the right eye met the crite-
Non-significant adverse events were events that did not
ria, the "best" eye was used.
warrant discontinuation from the clinical trial.
The safety analysis set consisted of all randomized sub-
Subjects could discontinue or withdraw from the trial for
jects who received at least 1 dose of treatment. Incidence
any reason. Investigators could discontinue a subject if, in
of unexpected ocular or systemic findings, adverse events,
his/her opinion, it was in the best interest of the patient,
and temporary/permanent discontinuation were tabu-
if there was non-compliance with study visits, if there was
lated and evaluated using Fisher's exact test. All tests were
more that 25% non-compliance with self-administration
of treatment, or if there was protocol deviation. Placebo Arm Demographics and Baseline Characteristics
The IRB for this study determined that standard of care for
Demographics and baseline characteristics of the 37
age-related macular degeneration must include an Age-
patients receiving the nutritional supplement are outlined
Related Eye Disease Study (AREDS)-type nutritional sup-
in Table 3. Subjects enrolled in the TOZAL study were
plement and that no true placebo arm would be permissi-
matched for inclusion and exclusion criteria with the
ble. A placebo arm was constructed from a review of the
MIRA-1 study. Subjects in both cohorts were similar
literature. The exclusion and inclusion criteria used for the
across age, gender, ethnicity, and mean baseline BCVA [7].
Multicenter Investigation of Rheopheresis for AMD(MIRA-1) trial were followed for the TOZAL study. Patient
Visual Acuity Outcomes
demographics between subjects enrolled in the MIRA-1
In the per-protocol analysis, the mean change from base-
study and the TOZAL study were similar. All subjects in
line in ETDRS BCVA (logMAR) was calculated at 3 and 6
the MIRA-1 study received an oral supplement consisting
months (Figure 2). While the placebo arm experienced a
of 400 mg vitamin C, 200 IU vitamin E, 40 mg zinc, and
negative mean ETDRS line change of 1.49 lines at 6
3,000 IU beta-carotene [7]. The results from the placebo
months (loss of VA), the treatment group demonstrated a
arm of the MIRA-1 study are used as a comparator in this
positive mean ETDRS line change of 0.54 lines at 6
months (gain in VA). The mean logMAR line differencebetween the treatment and placebo-control groups was
Statistical Analysis
2.03 lines at 6 months postbaseline. A continual improve-
Sample size and power calculations were based on the pri-
ment in BCVA (logMAR) over time was demonstrated in
mary efficacy endpoint. Results from two rheopheresis
the treatment group, while overall, the placebo arm con-
studies (Brunner and MIRA-1) were used to estimate the
mean change expected [7,19]. Thirty-four patients wereincluded in the per-protocol analysis.
At 6 months, of those subjects in the treatment arm,56.7% experienced improved BCVA (logMAR), 20.0%
Statistical analyses were performed using SPSS for Win-
maintained their BCVA (logMAR), and 23.3% experi-
dows (SPSS 14.0, SPSS Inc., Chicago, IL). A paired t-test
enced worsened BCVA (logMAR). Overall 76.7% of
was used to test the null hypothesis, with the average VA
patients improved or maintained their BCVA (logMAR)
score the same at baseline and follow-up. A two-sided
with the TOZAL nutritional supplementation (Figure 3).
alpha level of 0.05 was used to determine statistical signif-icance. Secondary Outcomes Fluorescein angiogram, retinal photographs, contrast sen-
Primary efficacy endpoint analysis consisted of all rand-
sitivity, full-threshold visual fields, macular testing (cen-
omized and dispensed subjects with baseline and at least
tral 10° threshold visual field), and the Visual Function
1 post-treatment VA recorded. Baseline was equated to VA
(page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
Table 3: Demographics and baseline characteristics
Questionanaire-25 (VFQ-25) were found to have little sig-
quent events were systemic gastrointestinal (GI) reactions,
including gastric upset, reflux, nausea, and taste perver-sion. The majority of these events occurred in patients
Statistical Analyses
who had not followed the prescribed procedure of taking
The average (SD) VA score was 0.409 (0.196) versus 0.355
the supplement concurrent food intake. After adjusting
(0.184) for baseline and follow-up respectively, t = -2.09;
their treatment schedule to always administering the
df = 33; P = .045. Figure 4 demonstrates the average (and
nutritional supplement with food, the majority of GI
95% confidence interval [CI] for the average) VA score at
issues resolved. Overall, there does not appear to be any
baseline and at follow-up. Tables 4 and 5 show a statisti-
significant adverse events related to the nutritional sup-
cally significant increase in the VA score from baseline to
follow-up. Thus, the null hypothesis, the average VA scoreis the same at baseline and follow-up, was rejected and it
Discussion
was concluded that there was a statistically significant
Visual Acuity
improvement in VA from baseline to follow-up. Table 5
Left untreated, patients with AMD are at risk for substan-
shows that the average increase in VA was 0.0541 and the
tial vision loss. The literature suggests that without inter-
95% CI for the average increase was (-0.107, -0.0013).
vention, patients with AMD will experience a loss in VA ofat least 0.8 lines and up to 1.5 lines at 6 months [5-7].
A post-hoc power analysis reveals that a sample size of 34achieves 80% power to detect a difference of 0.062
The LAST study reported Snellen equivalent VA improve-
between the baseline and follow-up average acuity score
ments in both intervention groups (Group 1 L: lutein 10
assuming a standard deviation of the differences (follow-
mg; Group 2 L/A: lutein 10 mg/antioxidant/vitamin and
up minus baseline) of 0.126 and with a significance level
mineral broad-spectrum supplementation formula), with
(alpha) of 0.05 using a two-sided paired t-test. If the true
mean eye improvements of 5.4 letters for group 1 L (95%
population change (follow-up minus baseline) was -
CI, 2.7–8.0, P = .01) and 3.5 letters for group 2 L/A (95%
0.062 with a standard deviation of 0.126, then this study
CI, 0.8–6.1, P = .04) [13].
would have had an 80% chance of detecting this differ-ence at the 0.05 level of significance.
The 6-month LUXEA study demonstrated that supple-mentation with carotenoids, lutein, and zeaxanthin can
Adverse Effects
improve mesoptic contrast acuity thresholds and visual
There were no significant systemic or ocular adverse
performance at low illumination [20].
events related to the nutritional supplement. The most fre-
(page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
e in 0.5 asel b m Nutrition Supple ment
Mean ETDRS line change at 3 and 6 months.
The CARMIS study treated 153 patients with AMD
ment prescribed in the TOZAL trial allowed for 76.7% of
(AREDS category 3, 4) and VA of greater than 20/32 (0.3
subjects to improve or maintain their VA, with up to 0.5
LogMAR) with lutein 10 mg, zeaxanthin 1 mg, astaxan-
lines of VA improvement at 6 months.
thin 4 mg, vitamin C 180 mg, vitamin E 30 mg, zinc 22.5mg, and copper 1 mg (AZYR SIF®, Sifi Italy). Patients
Nutritional Supplements
received baseline, 6-month, and 1-year follow-up with
Countless studies support the use of high-dose vitamins,
ETDRS and the 39-item NEI-VFQ. After 1 year, treated
antioxidants, omega-3 fatty acids, zinc, and carotenoids in
patients showed stabilization of VA and significantly bet-
the treatment of AMD. In addition, studies on the serum
ter ETDRS scores (87 +/- 6) compared to controls (80 +/-
levels of compounds including vitamins A, C, and E, car-
7; P = .02). VFQ-39 scores were significantly increased in
otenoids, zinc, selenium, and fibroblast growth factor in
the treatment group (P = .001) [21].
subjects with AMD suggest that low levels of these com-pounds put patients at greater risk for the development of
The AREDS formula does not address the vast majority of
AMD [8-13]. However, recent reports of adverse events
patients who want to improve visual function while pre-
associated with specific supplement components empha-
venting advanced AMD. The targeted nutritional supple-
size the need for improved supplement formulation. (page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
ts with improved or maintained BCVA at 6
Percent of subjects with improved or maintained BCVA at 6 months.
CI for average) visual acuity at baseline
Average (and 95% CI for average) visual acuity at baseline
Results of several large studies suggest that supplemental
beta-carotene increases the risk of developing lung cancerin heavy smokers [22-24]. Thus, it has been recom-mended that subjects with a history of smoking avoid sup-plemental beta-carotene as part of an AMD preventionprogram. However, an increased intake of foods rich in
avoided [27]. In an attempt to address these potential risk
beta-carotene has not been found to pose a heightened
factors, the TOZAL supplement was designed with 200 IU
risk for the development of lung cancer among current
and non-smokers [25]. Other carotenoids derived fromwhole foods (lutein, zeaxanthin, and lycopene) are also
Supplemental zinc has been found to decrease the rate of
not associated with increased risk for lung cancer [25].
loss of VA associated with AMD [16]. High doses of zincwere included in the AREDS supplement (80 mg as zinc
The supplement prescribed in the TOZAL study was
oxide), as well as copper (2 mg) to help prevent copper
designed to address the risk of lung cancer among smok-
deficiency associated with zinc supplementation. In the
ers receiving supplemental beta-carotene by focusing on
AREDS study, 7.5% of participants receiving a zinc-con-
beta-carotene derived from whole foods. The TOZAL sup-
taining nutritional supplements vs 5.0% of participants
plement contained 18,640 IU of natural beta-carotene
receiving no zinc in their nutritional supplement reported
urinary tract problems that required hospitalization, aswell as increased rates of anemia (anemia results were
Recent data link high doses of vitamin E to a 13% increase
found not to be statistically significant) [16]. In an effort
in the risk for heart failure [26]. In addition, a separate
to limit the adverse effects associated with high-dose zinc,
study found that doses of 400 IU or more of vitamin E
the TOZAL supplement was designed with 69.6 mg zinc
increased the chance of early death or, according to the
and 1.6 mg copper. No urinary tract adverse events or ane-
[23,24] authors, "all-cause mortality" and should be
mia were reported during the TOZAL trial. Table 4: Paired samples statistics (page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
Table 5: Paired samples test
95% Confidence Interval of the Difference
In 1998, van den Berg et al found that lutein negatively
Additional material
affected beta-carotene absorption when the two weregiven simultaneously [28]. This decrease in absorption
Additional File 1
may affect the amount of beta-carotene available for con-
version to retinol. In the AREDS study, lutein was not a
constituent of the formula, thereby circumventing the
issue. As newer formulas are developed that contain
lutein, consideration must be given to administering vita-min A in addition to beta-carotene. In the TOZAL study,
Additional File 2
this adjustment was made by administering 18,640 IU of
natural beta-carotene and 10,000 IU of vitamin A.
While toxicity has occurred at dosages of vitamin A of upto 50,000 IU/day for a period of 18 to 24 months, [29-32]an intake of 10,000 IU/day has not been associated withtoxicity and is considered safe. Acknowledgements The author wishes to acknowledge the following researchers and study Conclusion
centers who participated in this study: Richard Rosen, M.D., New York Eye
The present study confirms previously published reports
& Ear Infirmary; Baruch Kupperman, M.D., Ph.D., University of California
on the direction and magnitude of improved visual acuity
Irvine; Frederick Davidorf, M.D., Ohio State University; Brain Berger, M.D.,
in dry AMD [13,20,21]. That we did not find improve-
ments in other visual function parameters such as the con-trast sensitivity function, is likely related to the short
The author also wishes to thank the following for their considerable con-tributions with respect to biostatistical consultations and analysis: David M.
duration of this study. The National Eye Institute's AREDS
Harris, Ph.D., Bio-Medical Consultants; John Burkhart, Ph.D., Burkhart and
II trial will follow a qualitatively similar supplement (i.e.,
Associates; Steven D. Creech, M.S., Statistically Significant Consulting, LLC.
the AREDS II formula has lower zinc, higher omega-3,lutein and zeaxanthin in some of its treatment arms) as
Funding for the study and for the manuscript preparation was provided by
TOZAL (without the addition of taurine). The results of
the TOZAL study reported here support the potential forpositive visual outcomes in the AREDS II trial. References 1. National Eye Institute. Vision problems in the US 2006 ].
We can not completely dismiss microcurrent stimulation
(with or without supplementation) as we did not evaluate
all available methods of stimulation. 132:682-692.
Christen WG, Glynn RJ, Manson JE, Ajani UA, Burning JE:
Treatment based on dietary manipulation should con-
JAMA 1996, 276:1147-1151.
tinue to be pursued and refined as a simple, low-cost,
JAMA 1996, 276:1141-1146.
Newsome DA, Swartz M, Leone NC, Elston RC, Miller E:
Competing interests Arch Ophthalmol 1988, 106:192-198.
The author(s) declare that they have no competing inter-
Ladewig MS, Ladewig K, Guner M, Heidrich H: Prostoglandin E1 infusion therapy in dry age-related macular degeneration. Prostoglandins Leuko Essent Fatty Acids 2005, 72:251-256.
MIRA-1 study group, Pulido JS: Trans Am Ophthalmol Soc 2002, 100:85-106. (page number not for citation purposes)BMC Ophthalmology 2007, 7:3
http://www.biomedcentral.com/1471-2415/7/3
Curr Eye Res 2004, 29:387-401.
Bernstein PS, Zhao DY, Wintch SW, Ermakkov IV, McClane RW, Gel-
Am J Clin Nutr 1998, 68:82-89.
Ensmiger: Food nutrition encyclopedia Clovis, CA: Pegus Press; 1983.
Ophthalmology 2002, 109:1780-1787.
Wright: Nutrition therapy for the 1990s: a seminar for health care profes-
Werback: Nutrition influences on illness Tarzana, CA: Third Line Press;
272:1413-1420.
Bricklin: The practical encyclopedia of natural healing Emmaus, PA:
Conner WE, Neuringer M, Reisbick S: Essential fatty acids: the importance of n-2 fatty acids in the retina and the brain. Nutrition Reviews 1992, 50:21-29. Pre-publication history
The pre-publication history for this paper can be accessed
Mech Ageing Dev 1999, 107:159-164.
ww.biomedcentral.com/1471-2415/7/3/prepub
Optometry 2004, 75:216-230.
Age-Related Macular Degeneration Study Group: J Am Optom Assoc 1996, 67:12-29.
Age-Related Macular Degeneration Study Group: J Am Optom Assoc 1996, 67:30-49.
Age-Related Eye Disease Study Research Group:Arch Ophthalmol 2001, 119:1417-1436.
Litovitz TL, Klein-Schwartz W, Rodgers GC, Cobaugh DJ, Yoniss J, Omslaer JC, et al.Am J Emerg Med 2002, 20:391-452.
Allen MJ, Jarding JB, Zehner R: Macular degeneration treatment with nutrients and micro current electricity.J Orthomolec Med 1998, 13:211-214.
Brunner R, Widder RA, Walter P: Retina 2000, 20:483-491.
Kvansakul J, Rodriguez-Carmona M, Edgar DF, Barker FM, Kopcke W, Schalch W, et al.Ophthal- mic Physiol Opt 2006, 26:362-371.
Sartore M, Fregona I, Piermarocchi S, CARMIS Research Group: Effects of short-term supplementation with carotenoids and antioxidants on visual acuity and visual function in age- related macular degeneration.Presented at: ARVO; April 30-May 4, 2006; Fort Lauderdale, Florida .
Alpha-tocopherol beta-carotene cancer prevention study group: N Engl J Med 1994, 330:1029-1035.
Omenn GS, Goodman GE, Thornquist MD: J Natl Cancer Inst 1996, 88:1550-1559.
scientist can read your work free of charge
"BioMed Central will be the most significant development for disseminating the results of biomedical researc h in our lifetime."25:1315-1325.
Mannisto S, Smith-Warner SA, Spiegelman D:
Cancer Epidemiol Biomarkers Prev 2004, 13:40-48.
available free of charge to the entire biomedical community
Harvard Health Publications: Research linking high doses of vita- min E to heart failure is causing new worries about the
peer reviewed and published immediately upon acceptance
AREDS vitamins for macular degeneration.Harv Health Lett
cited in PubMed and archived on PubMed Central
2005, 30:6.
Miller ER, Pastor-Barriuso R, Dalal D: Meta-analysis: high-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med 2005, 142:46. (page number not for citation purposes)
Tuberkulose Die Herausgabe dieser Reihe durch das Robert Koch-Institut erfolgt auf der Grundlage des §4 Infektionsschutzgesetz (IfSG). Praktisch bedeutsame Angaben zu wichtigen Infektionskrankheiten sollen aktuell und konzentriert der Orientierung dienen. Die Beiträge werden in Zusammenarbeit mit den Nationalen Referenzzentren, Konsiliarlaboratorien sowie weiteren Experten erarbeitet. Die Pu
Efficacy of a green tea extract rich in catechin polyphenols andcaffeine in increasing 24-h energy expenditure and fat oxidationin humans1–3 Abdul G Dulloo, Claudette Duret, Dorothée Rohrer, Lucien Girardier, Nouri Mensi, Marc Fathi, Philippe Chantre,and Jacques Vandermander ABSTRACT context, there has been renewed interest in the potential thermo- Background: Current interest in the r
 BMC Ophthalmology
BMC Ophthalmology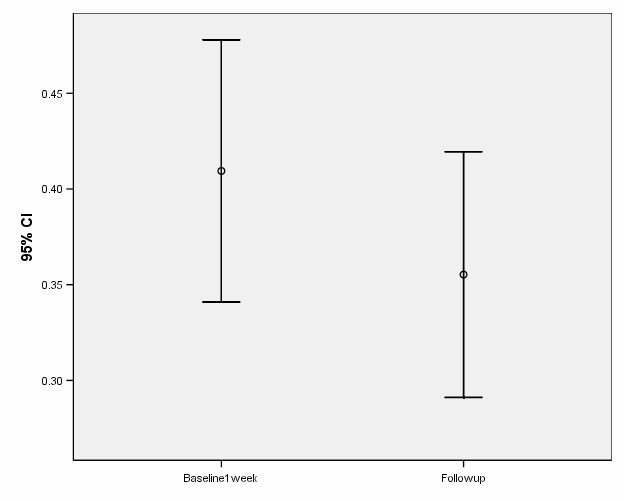 BMC Ophthalmology 2007, 7:3
BMC Ophthalmology 2007, 7:3