La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Layout
Mucosalpreservationiscriticaltosuccessintreatmentofnasalobstructionsecondaryto
turbinate hypertrophy. Since hypertrophy is most often secondary to submucosal and non-
osseous factors including hypervascularity and submucosal soft tissue excess, Bipolar
Radiofrequency Turbinate Ablation (RFTA) represents a highly effective, rapid, and well-tolerated technique
that can be done both in the office/ clinic under local anaesthetic as well as in the operating room (OR) in
conjunction with other nasal, sinus, or turbinate procedures.
Hypertrophy of the inferior turbinates is an important
cause of nasal obstruction. It is caused by multiple fac-
Ablation (RFTA) to be an extremely valuable instru-
tors including both soft tissue and bony factors,
ment in management of the obstructive turbinate,
including hypervascular engorgement, inflammation,
both as an isolated procedure, and in conjunction
and compensatory turbinate hypertrophy on the side
with septoplasty, sinus surgery, and as an adjunct to
less blocked by cartilaginous or bony deformities.
limited excisional turbinate procedures. Additionally,
Medical treatment for obstruction, while critical and
RFTA can be done easily in the office / clinic setting,
first-line in nature, often fails when anatomical
with re-usable instrumentation, thus providing a
turbinate obstruction exists. Thus, turbinate reduction
patient-friendly, cost effective alternative to OR
is critical to management of the obstructed nose.1
surgery in selected cases. We recommend RFTA as an
Traditional y, turbinate excision comprised the main-
essential tool in the rhinologic armamentarium.4,5,6
stay of treatment. However, our increasing understand-ing of the role of turbinates in nasal obstruction, along
Preoperative assessment
with the morbidity of excisional techniques, most
A thorough nasal and sinus examination delineates
notable in the prevalence of ‘empty nose syndrome’, led
the causes of nasal obstruction. Contributions of the
to more conservative approaches to the turbinates.
turbinates, septum, nasal valve, dorsum, and inflam-
‘How I Do It’ is
Unlike epithelium-ablating techniques, RFTA has been
matory and infectious causes should be weighed
co-ordinated by
shown to preserve mucociliary clearance.2,3
before proceeding. The soft tissue contribution to
Mr KW Ah-See, MD, FRCS, FRCS(ORL), Consultant Otolaryngologist -Head and Neck Surgeon, Aberdeen Royal Infirmary, Foresterhill, Aberdeen, AB25 2ZN, UK. Tel: +44 (0)122 455 3571, Email: kim.ah-see@nhs.net ‘How I Do It’ 1a: Preoperative view of hypertrophic left turbinate.1b: RF device inserted into hypertophic turbinate with fullNote how the hypertrophic turbinate obstructs the airway,penetration of the bipolar electrodes.David Greene, MD, FACS, FARS, Chief of Otolaryngology, Physicians Regional Health System; Adjunct Faculty, Cleveland Clinic Head and Neck Institute. Correspondence Physician’s Regional Medical Center, 6101 Pine Ridge Road, Naples, FL 34109, USA. Email: DavidGreeneMD@ comcast.net 1c: Turbinate at completion of ablation pass with the RF1d: Postoperative view. Completed turbinate ablation withTel: 239-348-4081. device. Note the contraction and blanching of the turbinate,substantial reduction of turbinate bulk, clear airway, andwhich indicates the endpoint of treatment.unobstructed view of the middle turbinate.
ENTNews | JUL/AUG 2008 | VOL 17 NO 3
turbinate hypertrophy, versus that of thebone, can be assessed by decongestionwith oxymetazoline.
of obstruction, such as nasal steroids, aller-gy treatment, and treatment of sinusitis,should be performed. Failure of medicaltherapy is the indication for surgical treat-ment. In the ENT clinic, most often ourpatients have already undergone maximal
Figure 2: Radiofrequency Turbinate Ablation (RFTA) procedure: before and after.
medical therapy, and are ready for surgicalintervention.
later, a second injection is given to ‘re-
inflate’ the turbinate, expanding the sub-
burning or injuring surrounding structures.
vision, allowing the surgeon to observe the
1. Isolated turbinate hypertrophy princi-
hypertrophic turbinate tissues blanch and
additional tachycardia in the patient since
cautery, the tissue is not allowed to char. As
3. High-risk status of the patient for the OR
probe (Ellman International, Oceanside, NY,
4. Patient preference for a minimally-inva-
USA) is then introduced submucosally into
the turbinate at the head of the turbinate
turbinate probe consisted of two parallel
needles with 24.5mm exposed electrodes.
sparing turbinate reduction technique, in
conjunction with turbinate out-fracture, or
turbinate obstructing the valve area. In our
series, RFTA has thus facilitated greatly
Surgical technique
probe is slid out of the turbinate (Surgitron
In the office / clinic setting, the patient is
4.0 Dual Frequency radiofrequency genera-
reduced complications to minimal levels.
tor, Ellman International, Oceanside, NY,
USA). This setting utilises 19 watts, which
Postoperative period
For patients treated with RFTA as an isolated
amount of 1% lidocaine with 1:100,000 epi-
procedure, there is no recovery period. Our
nephrine, to anaesthetise the turbinate, but
patients occasionally require acetaminophen
not give the patient excessive side-effects
‘paracetamol’ for analgesia, but often need
of epinephrine uptake. Five to ten minutes
nothing, and can resume normal activities
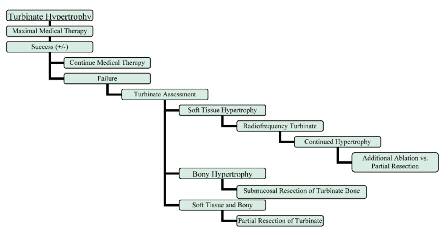
Figure 2: Algorithm for choice of turbinate reduction techniques.
ENTNews | JUL/AUG 2008 | VOL 17 NO 3
as long as they avoid straining. Nasal emollients and saline are rec-ommended as needed. The patients were seen one month later. In5% of our series, a small crust was noted and removed. At this time,patients with soft-tissue hypertrophy of the turbinates should feelsubstantially improved. Those in whom complete relief has notbeen achieved can be scheduled for other nasal surgery in the ORsuch as septoplasty. For patients who have undergone RFTA in con-junction with other nasal and sinus procedures, standard FESS / sep-toplasty / rhinoplasty care is given, but is much lessened by thereduced morbidity of RFTA versus resection. Our experience The author has performed 438 RFTA procedures using this technique, with follow-up from one month to five years, in patients ranging from 18-85. The procedure was well tolerated by all of the patients. A sub- stantial proportion of patients were managed for nasal obstruction causing CPAP failures in OSAS. Two hundred and twenty of the cases were performed in the office / clinic, with only four episodes of bleed- ing requiring conservative treatment. Notably, all four of these patients had been on anticoagulant therapy, and were treated in the office / clinic to avoid the risk of anaesthesia. No cases of atrophic rhinitis, crusting, synechiae, dryness, persistent crusting, olfactory disturbance, synechiae, necrosis, or any other complication were noted in RFTA- treated turbinate tissue in either the isolated or combination RFTA groups. Substantial decrease in the bulk of the turbinate was observed in all cases. The only patients who ultimately required OR surgery (sep- toplasty, FESS, or rhinoplasty), were those who were identified preop- eratively as having bony and cartilaginous deformity, and had elected RFTA as a minimally invasive procedure, or as a way to avoid OR risks. More than half of patients whom the author recommended for OR surgery were satisfied with the improvement from RFTA, despite indi- cations for more invasive surgery. Conclusion Radiofrequency Turbinate Ablation (RFTA) is a safe and highly effec- tive technique for symptomatic nasal obstruction refractory to medical therapy, and attributable to hypertrophy of turbinate soft tissue. Bipolar RFTA preserves the turbinate mucosa, thus minimis- ing the risk of complications and physiological disturbances from turbinate reduction. When used in conjunction with excisional techniques to reduce obstructive turbinate bone, it facilitates mucosal preservation for the remainder of the turbinate, thus improving patient tolerance and outcomes. Thus, RFTA should be considered an effective and cost effective option in the treatment of nasal obstruction. n References
1. Rice DH, Kern EB, Marple BF, Mabry RL, Friedman WH. The turbinates in nasal and
sinus surgery: a consensus statement. Ear Nose Throat J. 2003;82(2):82-4.
2. Sapci T, Sahin B, Karavus A, Akbulut UG. Comparison of the effects of radiofre-
quency tissue ablation, CO2 laser ablation and partial turbinectomy applications on nasal mucociliary functions. Laryngoscope. 2003;113(3):514-9.
3. Carrie S, Wright RG, Jones AS, Stevens JC, Parker AJ, Yardley AP. Long-term results
of trimming of the inferior turbinates. Clin Otolaryngol Allied Sci. 1996;21(2):139-41.
4. Coste A, Yona L, Blumen M, Louis B, Zerah F, Rugina M, Peynegre R, Harf A,
Escudier E. Radiofrequency is a safe and effective treatment of turbinate hypertro- phy. Laryngoscope. 2001;111(5):894-9.
5. Utley DS, Goode RL, Hakim I. Radiofrequency energy tissue ablation for the treat-
ment of nasal obstruction secondary to turbinate hypertrophy. Laryngoscope. 1999;109(5):683-6.
6. Elwany S, Gaimaee R, Fattah HA. Radiofrquency bipolar submucosal diathermy of
the inferior turbinates. Am J Rhinol. 1999;13(2):145-9. Competing interest: Dr Greene’s research on Radiofrequency Ablation of the Turbinates has been financially supported by Ellman International, Inc.
ENTNews | JUL/AUG 2008 | VOL 17 NO 3
National Symposium on Innovation in TB Diagnostics, Drug Targets and Biomarkers C.M.E. On Innovation in Molecular and Immunodiagnostics for PTB & EPTB in India (*Supported by KHS, AstraZeneca, ICMR, DBT, CSIR, DST & MCI) January 27 –28, 2014 JB Tropical Disease Research Centre, Mahatma Gandhi Institute of Medical Sciences, Sevagram - Poster Session: There
Consolidated TEXT produced by the CONSLEG system of the Office for Official Publications of the European Communities Office for Official Publications of the European Communities1986L0362 — EN — 06.05.2004 — 035.001 — 1 This document is meant purely as a documentation tool and the institutions do not assume any liability for its contents COUNCIL DIRECTIVE of 24 July 1986







 Mucosalpreservationiscriticaltosuccessintreatmentofnasalobstructionsecondaryto
turbinate hypertrophy. Since hypertrophy is most often secondary to submucosal and non-
osseous factors including hypervascularity and submucosal soft tissue excess, Bipolar
Radiofrequency Turbinate Ablation (RFTA) represents a highly effective, rapid, and well-tolerated technique
that can be done both in the office/ clinic under local anaesthetic as well as in the operating room (OR) in
conjunction with other nasal, sinus, or turbinate procedures.
Mucosalpreservationiscriticaltosuccessintreatmentofnasalobstructionsecondaryto
turbinate hypertrophy. Since hypertrophy is most often secondary to submucosal and non-
osseous factors including hypervascularity and submucosal soft tissue excess, Bipolar
Radiofrequency Turbinate Ablation (RFTA) represents a highly effective, rapid, and well-tolerated technique
that can be done both in the office/ clinic under local anaesthetic as well as in the operating room (OR) in
conjunction with other nasal, sinus, or turbinate procedures.

 turbinate hypertrophy, versus that of thebone, can be assessed by decongestionwith oxymetazoline.
turbinate hypertrophy, versus that of thebone, can be assessed by decongestionwith oxymetazoline.