La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Doi:10.1016/s0002-9149(03)00845-2
Effect of Amiodarone on the Descending Limb of the
Peter Smetana, MD, Esther Pueyo, BSc, Katerina Hnatkova, PhD,
Velislav Batchvarov, MD, A. John Camm, MD, and Marek Malik, PhD, MD
Comparing patients treated after myocardial infarc-
enrolled patients were survivors of acute myocardial
tion with amiodarone or with placebo, we found a
infarction (aged 18 to 75 years) who had left ventric-
significant rate-dependent prolongation of TpTe inter-
ular ejection fraction Յ40% as assessed by multiple-
val in patients who received amiodarone. Patients
gated nuclear angiography between days 5 and 21
who had arrhythmic death had significantly longer
after the index infarction. The median follow-up of the
TpTe intervals than others on placebo but not on
trial was 21 months. A total of 866 3-lead Holter
amiodarone. Assuming that TpTe reflects transmural
recordings (462 from patients receiving amiodarone
repolarization heterogeneity, our findings suggest
and 404 from patients receiving placebo) obtained 1
that heterogeneity and arrhythmic risk are increased
month after treatment randomization were available
by amiodarone. This contradicts the finding of de-
for this study. Clinical characteristics of the studypopulation are listed in
creased transmural repolarization heterogeneity by
RR, QT, and QTp intervals in all 24-hour record-
amiodarone and the appreciated antiarrhythmic effi-
ings were automatically measured on a beat-to-beat
cacy of this drug. ᮊ2003 by Excerpta Medica, Inc.
basis by a commercial Holter system (Pathfinder, Del
(Am J Cardiol 2003;92:742–746)
Mar Reynolds Medical, Irvine, California). TpTe in-
Therearesubstantialdifferencesintheelectricalprop- tervals were computed as the difference of QT and
erties between different layers of the ventricular
QTp intervals. The automatic measurement was per-
Based on in vitro experiments, the interval
formed under careful visual control, and artifacts were
between the peak and the end of the T wave (TpTe) was
eliminated manually. Only beats with accepted QT
proposed to quantify transmural heterogeneity in action
and RR intervals were considered. In each recording,
potential duration Also based on in vitro exper-
the analysis was performed using the lead with most
iments, the antiarrhythmic effect of amiodarone was
partly attributed to decreased transmural repolarization
Instead of using only the RR interval preceding
each beat, weighted averages of RR intervals (RR)
drug has this effect in the clinical setting. We therefore
within a window preceding each beat were consid-
examined the following assumptions. (1) If TpTe ex-
presses transmural repolarization heterogeneity and if
diac cycles in a window previous to the QT measure-
amiodarone decreases this heterogeneity, will the TpTe
ment were weighted for their impact on its rate
intervals in patients receiving placebo after infarction be
adaptation. For each cardiac beat, the corresponding
longer than in those receiving amiodarone? (2) If the
numeric representation of the RR interval history and
antiarrhythmic effect of amiodarone is at least in part
the corresponding RR interval value was derived. The
achieved by the decrease of transmural repolarization
optimum averaging window was identified individu-
heterogeneity, will patients who experience arrhythmic
ally in each patient by best-fitting QT/RR data to a set
death while receiving amiodarone have longer TpTe
of 10 a priori defined regression models designed to
intervals than those who do not? We therefore investi-
cover a physiologic variety of QT/RR In this
gated QT, Q to T peak (QTp), and TpTe intervals in
way, the influence of QT/RR hysteresis on the assess-
Holter recordings of patients who were enrolled into the
ment of the QT/RR relation was eliminated.
European Myocardial Infarction Amiodarone (i.e.,
Because transmural repolarization heterogeneity is
patients randomized to placebo and amiodarone after
known to be influenced by cycle uncorrected
QT, QTp, and TpTe intervals and TpTe/QT ratios
were averaged in each recording across 10-ms RR
The study used data collected during the European
interval bins ranging from 550 to 1,150 ms.
Myocardial Infarction Amiodarone In short,
Statistical analysis was based on the intention to
treat at randomization. Arrhythmic death was used asthe outcome event. The classification of the mode of
From the Department of Cardiological Sciences, St. George’s HospitalMedical School, London, United Kingdom. This study was supported
death originally performed by the event committee of
in part by the Primara¨rzteverein des Wilhelminenspitals, Vienna, Aus-
the trial was used. A comparison was also performed
tria; and the Wellcome Trust and the British Heart Foundation, London,
between patients who did and did not have arrhythmic
United Kingdom. Dr. Malik’s address is: Department of Cardiological
death. Averaged values of QT, QTp, and TpTe in
Sciences, St. George’s Hospital Medical School, Cranmer Terrace,
individual RR bins were pooled together in amioda-
London SW17 0RE, United Kingdom. E-mail: m.malik@sghms.ac.uk. Manuscript received March 25, 2003; revised manuscript received
rone- and placebo-treated patients. Student’s t test for
unpaired samples was used for the comparison. A p
2003 by Excerpta Medica, Inc. All rights reserved.
The American Journal of Cardiology Vol. 92 September 15, 2003
TABLE 1 Baseline Characteristics of Patients*
*Values in parentheses represent the percentage of the total number in each arm. †
p Value refers to comparison between amiodarone group and placebo group.
TpTe interval in patients who receivedamiodarone after infarction who didnot have arrhythmic death. Although
value Ͻ0.05 was considered statistically significant.
patients who received placebo who had arrhythmic death
had significantly longer TpTe intervals than those who
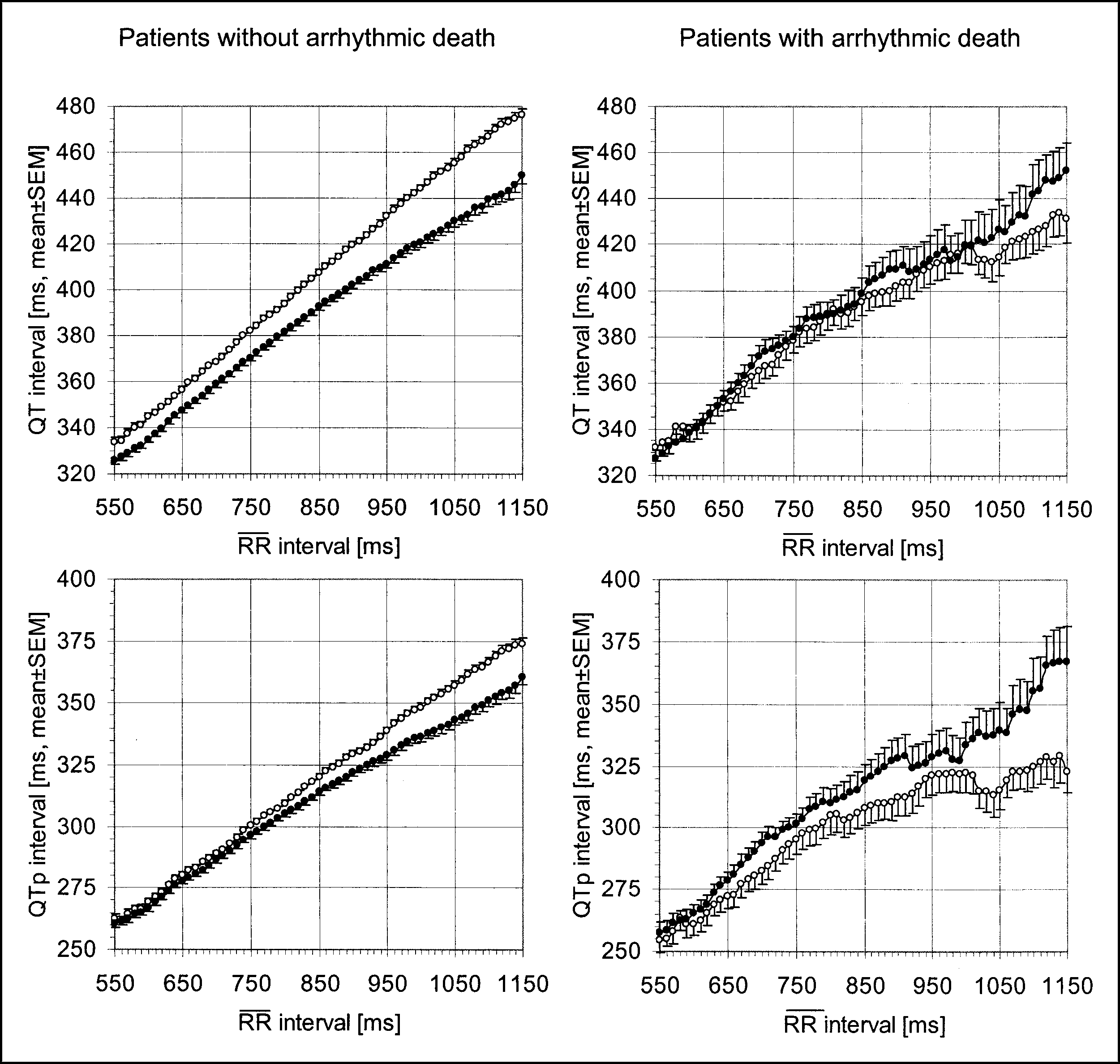
The rate relations of the QT and QTp intervals are
did not have arrhythmic death, there was no significant
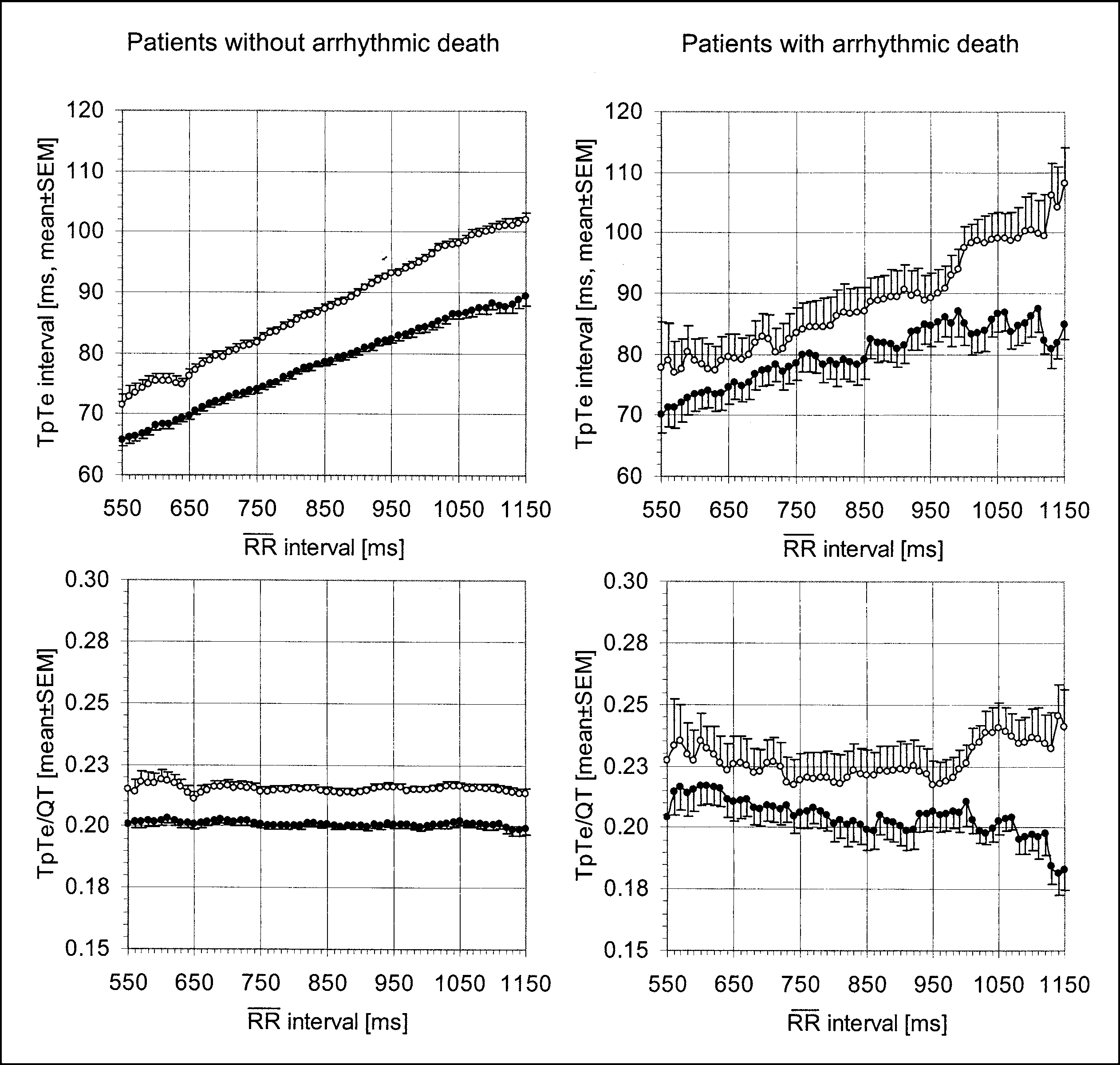
shown in and the rate relation of the TpTe
difference among patients who received amiodarone.
interval and TpTe/QT ratio in the investigated groups is
Assuming that TpTe reflects transmural repolariza-
shown in Because it is obvious from these
tion heterogeneity, these findings suggest that this
figures that the difference between the groups is rate
heterogeneity is increased by amiodarone. This con-
dependent, shows the statistical evaluation of the
tradicts the finding of decreased transmural repolar-
QT, QTp, and TpTe intervals and the TpTe/QT ratio at
ization heterogeneity by amiodarone in cardiac tissue
2 different RR interval bins (i.e., 550 to 560 ms and
Although direct in vivo evidence of this drug
effect is missing, 2 other studies that investigated the
QTp and QT intervals were longer in patients with-
electrophysiologic effects of amiodarone in isolated
out arrhythmic death who received amiodarone. The
Langendorff-perfused rabbit also described
difference was rate dependent as evidenced by being
no changes in dispersion of APD across the epicardi-
more marked at long RR intervals. However, patients
or between various right and left ventricular endo-
with arrhythmic death who received amiodarone had
cardial and epicardial Thus, a marked increase
shorter QTp intervals than did patients who received
in transmural repolarization heterogeneity by amioda-
placebo. Although this was less obvious at short RR
intervals, it became increasingly more marked at
It seems therefore questionable whether the TpTe
interval measured in clinical Holter recordings reflects
amiodarone vs no arrhythmic death on placebo: 550 to
transmural repolarization heterogeneity. Using a ca-
560 ms, p ϭ 0.216, and 1,140 to 1,150 ms, p ϭ 0.005,
respectively). For patients receiving placebo, there
that the inscription of the T wave of the electrocar-
was no significant difference between those with and
diogram stems mainly from differences in APD in
without arrhythmic death at any RR interval bin.
different layers of the ventricular wall. It was shown
Among patients receiving amiodarone, the TpTe
that the peak of the T wave marks full repolarization
interval did not significantly differ between those who
of the epicardium, whereas the end of the T wave
did and did not have arrhythmic death. However,
marks full repolarization of the M region. Therefore,
irrespective of the arrhythmic outcome, TpTe was
in vitro TpTe interval was shown to measure trans-
significantly longer in patients receiving amiodarone
mural dispersion of By recording epicardial
monophasic action potentials fromdifferent areas of the heart in open-chested dogs simultaneously with 2surface electrocardiographic leads,an earlier also suggested thatTpTe interval bear a certain relationto the dispersion of repolarization inthe entire heart.
in humans is missing, and the extentof transmural gradients of APD invivo remains to be Additionally, recent evidence sug-gests that transmural heterogeneitiesmight be even more variable thanConsidering the 3-di-mensional structure of the intactheart and the multitude of gradientspreviously (e,g.,apico-basal, right–left ventricular,anterior–posterior, and transmural),it seems unlikely, in a clinical set-ting, that the projection of the repo-larization dipole onto the body sur-face could be attributed to just thetransmural APD gradient. Still, al-though it was assumed already in the
FIGURE 1. Uncorrected mean QT and QTp intervals in patients on amiodarone (open circles) or on placebo (filled circles) plotted against 10-ms RR interval bins. Compari- son are made in patients with (left panel) and without (right panel) arrhythmic death.
sured in the intact organism is gener-ated by more than transmural ventric-ular gradients,” clinically measuredTpTe intervals are being increasinglyused as a surrogate of transmural repo-larization
creased TpTe values in various high-risk suggest that in-creased
circumstances, related to arrhythmicrisk. However, these observations donot prove that TpTe reflects transmu-ral repolarization heterogeneity, andthey also do not prove that increasedTpTe is a general risk marker in eachclinically defined population. Ourfinding of prolonged TpTe intervalsin patients receiving amiodarone—together with the widely appreciatedantiarrhythmic effiand lowof the drug—isclearly not compatible with the no-tion that clinical TpTe measurestransmural repolarization heteroge-neity and that an increase in such aheterogeneity is an arrhythmic riskfactor.
scribed increased TpTe intervals inpatients with long QT syndrome
FIGURE 2. Uncorrected mean TpTe interval and TpTe/QT ratio in patients on amioda- rone (open circles) or on placebo (filled circles) plotted against 10-ms RR interval bins. Comparison are made in patients with (left panel) and without (right panel) arrhyth- mic death. 744 THE AMERICAN JOURNAL OF CARDIOLOGYா TABLE 2 QT, QTp, and TpTe Intervals and TpTe/QT Ratio at Different RR Interval Bins in Patients With and Without Arrhythmic Death Receiving Amiodarone or Placebo
*p Value refers to comparison between amiodarone group and placebo group. †Mean Ϯ SD. ‡p Value refers to comparison between patients with and without arrhythmic death.
TpTe prolongation with arrhythmic risk. Consistent
tencies addressed in this study suggest that extrapola-
with this finding, we did not observe any difference in
tion of results of experimental studies of myocardial
TpTe between patients with and without arrhythmic
tissue models to human surface electrocardiograms is
death who received amiodarone. However, our finding
problematic. More appropriate surrogates of the in
of significantly longer TpTe intervals (at higher heart
vitro measured TpTe interval (e.g., the spatial mor-
rates) in patients with arrhythmic death who received
phology of the T wave) should be investigated.
placebo suggests that under some circumstances thismeasure is related to arrhythmic risk. In other words,as is with QT interval, there might be both a “bene-
1. Sicouri S, Antzelevitch C. A subpopulation of cells with unique electrophys-
ficial” and “bad” prolongation of the TpTe interval.
iological properties in the deep subepicardium of the canine ventricle. The M cell.
Our findings might also possibly suggest that insofar
Circ Res 1991;68:1729 –1741. 2. Yan GX, Antzelevitch C. Cellular basis for the normal T wave and the
as QTp and TpTe intervals are prolonged, amiodarone
electrocardiographic manifestations of the long-QT syndrome. Circulation 1998;
treatment is proportionally beneficial. However, when
TpTe/QT is increased, arrhythmic risk is enhanced. 3. Sicouri S, Moro S, Litovsky S, Elizari MV, Antzelevitch C. Chronic amioda- rone reduces transmural dispersion of repolarization in the canine heart. J Car-
Because the TpTe interval is influenced by inaccu-
diovasc Electrophysiol 1997;8:1269 –1279.
racies in both determination of the peak and the end of
4. Julian DG, Camm AJ, Frangin G, Janse MJ, Munoz A, Schwartz PJ, Simon P.
the T wave, its reliability might be questioned. How-
Randomised trial of effect of amiodarone on mortality in patients with left-ventricular dysfunction after recent myocardial infarction: EMIAT. European
ever, in this study, automatic measurements were
Myocardial Infarct Amiodarone Trial Investigators. Lancet 1997;349:667–674.
carefully visually validated to minimize this problem. 5. Pueyo E, Smetana P, Hnatkova K, Malik M. Optimum RR window length for
The analysis was performed on an intention-to-
estimation of the QT/RR regression model from continuous 24-hour Holterrecordings. Proc Annu Conference Comput Cardiol 2002;565–568.
treat basis at randomization. It is likely that some of
6. Batchvarov VN, Ghuran A, Smetana P, Hnatkova K, Harries M, Dilaveris P,
the patients receiving amiodarone discontinued the
Camm AJ, Malik M. QT-RR relationship in healthy subjects exhibits substantial
study medication during follow-up. However, because
intersubject variability and high intrasubject stability. Am J Physiol Heart CircPhysiol 2002;282:H2356 –2363.
we found few differences in patients receiving pla-
7. Iwata H, Kodama I, Suzuki R, Kamiya K, Toyama J. Effects of long-term oral
cebo, the exclusion of patients who discontinued the
administration of amiodarone on the ventricular repolarization of rabbit hearts.
study medication would only make our findings even
Jpn Circ J 1996;60:662–672. 8. Zabel M, Hohnloser SH, Behrens S, Woosley RL, Franz MR. Differential
effects of D-sotalol, quinidine, and amiodarone on dispersion ventricular repo-
Despite the convincing in vitro concept and good
larization in the isolated rabbit heart. J Cardiovasc Electrophysiol 1997;8:1239 –
accessibility of the TpTe interval as a measure of
1245. 9. Autenrieth G, Surawicz B, Kuo CS. Sequence of repolarization on the ven-
transmural repolarization heterogeneity, the inconsis-
tricular surface in the dog. Am Heart J 1975;89:463–469. 10. Anyukhovsky EP, Sosunov EA, Rosen MR. Regional differences in electro-
congenital long QT syndrome: the increased transmural dispersion of repolariza-
physiological properties of epicardium, midmyocardium, and endocardium. In
tion. Pacing Clin Electrophysiol 1998;21:172–175.
vitro and in vivo correlations. Circulation 1996;94:1981–1988. 16. Viitasalo M, Oikarinen L, Swan H, Vaananen H, Glatter K, Laitinen PJ, 11. Weissenburger J, Nesterenko VV, Antzelevitch C. Transmural heterogeneity
Kontula K, Barron HV, Toivonen L, Scheinman MM. Ambulatory electrocar-
of ventricular repolarization under baseline and long QT conditions in the canine
diographic evidence of transmural dispersion of repolarization in patients with
heart in vivo: Torsades de pointes develops with halothane but not pentobarbital
long-QT syndrome type 1 and 2. Circulation 2002;106:2473–2478.
anesthesia. J Cardiovasc Electrophysiol 2000;11:290 –304. 17. Savelieva I, Yap YG, Yi G, Guo X, Camm AJ, Malik M. Comparative
reproducibility of QT, QT peak, and T peak-T end intervals and dispersion in
Akar FG, Yan GX, Antzelevitch C, Rosenbaum DS. Unique topographical
normal subjects, patients with myocardial infarction, and patients with hypertro-
distribution of M cells underlies reentrant mechanism of Torsade de pointes in the
phic cardiomyopathy. Pacing Clin Electrophysiol 1998;21:2376 –2381.
long-QT syndrome. Circulation 2002;105:1247–1253. 18. Lubinski A, Kornacewicz-Jach Z, Wnuk-Wojnar AM, Adamus J, Kempa M, 13. Franz MR, Bargheer K, Rafflenbeul W, Haverich A, Lichtlen PR. Monopha-
Krolak T, Lewicka-Nowak E, Radomski M, Swiatecka G. The terminal portion of
sic action potential mapping in human subjects with normal electrocardiograms:
the T wave: a new electrocardiographic marker of risk of ventricular arrhythmias.
direct evidence for the genesis of the T-wave. Circulation 1987;75:379 –386. Pacing Clin Electrophysiol 2000;23:1957–1959. 14. Rosenbaum DS, Kaplan DT, Kanai A, Jackson L, Garan H, Cohen RJ, Salama 19. Mason JW. Amiodarone. N Engl J Med 1987;316:455–466.
G. Repolarization inhomogeneities in ventricular myocardium change dynami-
20. van Opstal JM, Schoenmakers M, Verduyn SC, de Groot SH, Leunissen JD,
cally with abrupt cycle length shortening. Circulation 1991;84:1333–1345.
van Der Hulst FF, Molenschot MM, Wellens HJ, Vos MA. Chronic amiodarone
15. Lubinski A, Lewicka-Nowak E, Kempa M, Baczynska AM, Romanowska I,
evokes no Torsade de pointes arrhythmias despite QT lengthening in an animal
Swiatecka G. New insight into repolarization abnormalities in patients with
model of acquired long-QT syndrome. Circulation 2001;104:2722–2727. Syncope in Children and Adolescents and the Congenital Long QT Syndrome
Anant Khositseth, MD, Matthew W. Martinez, MD, David J. Driscoll, MD, and
From a population-based epidemiologic cohort of chil-
range (420 to 470 ms) as patients with “incomplete
dren and adolescents who sought medical attention for
penetrant” or “concealed” LQTS also is unknown. syncope (n ؍ 151), screening 12-lead electrocardio- Such information is critical for proper interpretation of grams were obtained from 118 patients (79 female) to
the screening ECG when evaluating a young person
determine the frequency of significant QT prolongation.
with syncope. Thus, the objectives of this study were
The distribution of heart rate corrected QT intervals
to identify the frequency of significant and diagnostic
(QTc) was compared with age- and sex-matched con-
QT prolongation (QTc Ͼ470 ms) as well as the fre-
trols. Only one patient had QTc >470 ms. ᮊ2003 by quency of a nondiagnostic ECG in a community-based Excerpta Medica, Inc.
population of fainters who sought medical attention
(Am J Cardiol 2003;92:746–749)
compared with age- and sex-matched controls. It is generally recommended that an electrocardio-
Using data from the Rochester Epidemiology
gram (ECG) be part of the current evaluation of
Project, 151 children and adolescents Ͻ21 years old,
of whom 98 were female and 131 white, who lived in
prevalence of long QT syndrome (LQTS) in syncope
Rochester, Minnesota, were identified as having
is unknown. Before the molecular breakthroughs in
sought medical attention for an initial syncopal epi-
LQTS, a QT interval corrected for heart rate (QTc),
sode between 1987 and The medical records of
according to Bazett’s formula, Ն440 ms was consid-
each patient were reviewed, and those without docu-
ered prolonged, and a QTc Ͻ420 ms was considered
mentation of a screening ECG were contacted for
normal. However, more recent genotype–phenotype
participation in this Institutional Review Board-ap-
correlations have indicated that 25% to 40% of carri-
proved study. A 12-lead ECG was obtained from 118
ers of LQT1 and LQT2 mutations show QTc values
(78%) patients (79 female) from this cohort. The QTc
(420 to 470 ms) that overlap with those of noncarri-
was computed both automatically using the Marquette
In contrast, the prevalence of “fainters” having
MAC8 (GE Marquette Medical Systems, Inc., Mil-
a nondiagnostic ECG with a QTc falling in this same
waukee, Wisconsin) and manually. Manual determi-nation of the QT interval was performed using guide-
From the Department of Pediatric and Adolescent Medicine/Division
of Pediatric Cardiology; the Department of Medicine/Division of
investigator (MWM) performed all manual QTc de-
Cardiovascular Diseases; and the Department of Molecular Pharma-
terminations using lead II and the standard Bazett’s
cology and Experimental Therapeutics, Mayo Clinic/Mayo Founda-
tion, Rochester, Minnesota. Dr. Ackerman is supported by the Doris
Duke Charitable Foundation, New York, New York, and the National
agnostically significant QT prolongation was defined
Institutes of Health, Bethesda, Maryland (grant No. HD42569). Dr.
Ackerman’s address is: Long QT Syndrome Clinic and Sudden Death
ECGs from 118 age- and sex-matched controls
Genomics Laboratory, Guggenheim 501, Mayo Clinic/Mayo
were obtained from Mayo Clinic’s electrocardiogra-
Foundation, Rochester, Minnesota 55905. E-mail: ackerman.
phy database. The age of controls was matched to the
michael@mayo.edu. Manuscript received March 20, 2003; revisedmanuscript received and accepted May 27, 2003.
patient age at time of ECG rather than age at syncope,
2003 by Excerpta Medica, Inc. All rights reserved.
The American Journal of Cardiology Vol. 92 September 15, 2003
MPharm 4 PHAR0037 Law & Ethics Case Studies The aim of this study is to develop your-problem solving skills when faced with legal and ethical problems in pharmacy practice. Objectives Following your revision and completion of this background work you will be expected to:- • Understand the legal requirements of the Medicines Act 1968 concerning the appropriate supply of prescription only
American Journal of Obstetrics and Gynecology (2004) 190, S30e8James Trussell, PhD,a,* Charlotte Ellertson, PhD,b Felicia Stewart, MD,cElizabeth G. Raymond, MD, MPH,d Tara Shochet, MPHeWoodrow Wilson School of Public and International Affairs, Office of Population Research, Princeton University,Princeton, NJa; Ibis Reproductive Health, Cambridge, Massb; University of California San Francisco,
 monophasic action potentials fromdifferent areas of the heart in open-chested dogs simultaneously with 2surface electrocardiographic leads,an earlier also suggested thatTpTe interval bear a certain relationto the dispersion of repolarization inthe entire heart.
monophasic action potentials fromdifferent areas of the heart in open-chested dogs simultaneously with 2surface electrocardiographic leads,an earlier also suggested thatTpTe interval bear a certain relationto the dispersion of repolarization inthe entire heart.