La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Doi:10.1016/j.transproceed.2004.01.018
Pharmacology of Calcineurin Antagonists
M.H. Kapturczak, H.U. Meier-Kriesche, and B. Kaplan
ABSTRACTCyclosporine and tacrolimus share the same pharmacodynamic property of activated T-cell
suppression via inhibition of calcineurin. The introduction of these drugs to the immuno-
suppressive repertoire of transplant management has greatly improved the outcomes in
organ transplantation and constitutes arguably one of the major breakthroughs in modern
medicine. To this date, calcineurin inhibitors are the mainstay of prevention of allograft
rejection. The experience gained from the laboratory and clinical use of cyclosporine and
tacrolimus has greatly advanced our knowledge about the nature of many aspects of
immune response. However, the clinical practice still struggles with the shortcomings of
these drugs: the significant inter- and intraindividual variability of their pharmacokinetics,
the unpredictability of their pharmacodynamic effects, as well as complexity of interactions
with other agents in transplant recipients. This article briefly reviews the pharmacological
aspects of calcineurin antagonists as they relate to the mode of action and pharmacoki-
netics as well as drug interactions and monitoring.
CYCLOSPORINE AND TACROLIMUS—two of the anti–T-lymphocyteactivity,weredescribedinlead-
most potent immunosuppressives—are termed cal-
ing the way to its use in animal models of transplanta-
cineurin inhibitors due to their ability to inhibit this ubiq-
The impressive results of those studies were
uitous phosphatase. They both share similar physicochem-
followed shortly thereafter by first studies in human kidney
resulting in inhibition of synthesis of proinflammatory
after its discovery, in November of 1983, the US Food and
cytokines and interruption of the downstream sequence of
Drug Administration (FDA) approved cyclosporine for
events leading to allograft Both agents have
treatment and/or prevention of transplant rejection. Cur-
become the cornerstone of current immunosuppressive
rently, cyclosporine is used for prevention of graft rejection
in kidney, liver, heart, lung, and combined heart-lung
transplantation. In addition, it found its place in bone
marrow transplantation in prevention of graft-versus-host
The introduction of cyclosporine 20 years ago to the
disease as well as in treatment of autoimmune conditions
repertoire of immunosuppressive drugs constitutes one of
like psoriasis, atopic dermatitis, rheumatoid arthritis, and a
the major breakthroughs of modern medicine. It led to a
significant improvement in the outcomes of organ trans-
Cyclosporine is a lipophilic cyclic endecapep-
tide with one unique aminoacid in its structure. It was
In the early 1980s scientists at Fujisawa Pharmaceuticals
originally derived from a filamentous fungus Tolypocladium
began testing fermented Streptomyces broths for their
inflatum Gams in the laboratories of the Sandoz Company
specific inhibitory properties on mixed lymphocyte cultures.
in Basel, Switzerland. In 1971, in the antibiotic screening
process, which also included testing of various compounds
for their immunosuppressive properties, Drs J. Borel and
From the Department of Medicine, Division of Nephrology,
H. Sta¨helin observed that a fungal extract containing cyclo-
Hypertension and Transplantation, University of Florida Collegeof Medicine, Gainesville, Florida, USA.
sporine displayed not only a considerable immunosuppres-
Address reprint requests to Bruce Kaplan, MD, University of
sive activity but also absence of any significant cytotoxic
Florida College of Medicine, Division of Nephrology, Box
In 1976 the biological properties of cyclospor-
100224, 1600 SW Archer Road, Gainesville, FL 32610-0224.
ine, the first immunosuppressive agent with a specific
2004 by Elsevier Inc. All rights reserved.
360 Park Avenue South, New York, NY 10010-1710
Transplantation Proceedings, 36 (Suppl 2S), 25SϪ32S (2004)
The screening resulted in discovery of a soil fungus named
such a complex results in its binding to and inhibition of
Streptomyces tsukubaensis in 1984, which produced a potent
In the process of T-cell activation calcineurin,
immunosuppressant given a code FK506 and later named
which is a calmodulin-activated serine phosphatase, associ-
tacrolimus (acronym for Tsukuba macrolide immunosup-
ates with and dephosphorylates inactive nuclear factor of
pressive). In 1987, the results of in vitro testing and first
activated T cells (NFAT). This leads to NFAT translocation
to the nucleus and, in association with other transcription
tially, tacrolimus was evaluated in liver
factors like AP-1, initiation of downstream events involved
and the FDA approved it for the prevention of liver
transplant rejection in April 1994. Subsequently its use was
NFAT family, NFAT1, NFAT2, and NFAT4 participate in
expanded onto transplantation of other as well
transcriptional activation of interleukin-2 (IL-2), IL-4, and
as treatment of atopic dermatitis as a topical formulation.
The drug-immunophilin complex forms an inhib-
itory association with calcium-calmodulin–activated cal-
cineurin, preventing its binding and activation of
Cyclosporine and tacrolimus can also interfere with ac-
is a cyclic, highly hydrophobic endecapeptide that con-
tion of calcineurin on other substrates than NFAT. These
tains one unique aminoacid N-methyl-(4R)-4-butenyl-4-
methylthreonine in position 1 as well as two unusual
These actions can explain some of the side effects
aminoacids: sarcosine in position 3, and D-alanine in posi-
tion 8. Furthermore, seven of its aminoacids are N-methyl-
Unlike their inhibitory effects on transcription and ex-
ated, which may explain its resistance to inactivation in
pression of proinflammatory cytokines like IL-2, treatment
gastrointestinal Purified cyclosporine appears as
with cyclosporine or tacrolimus seems to be associated with
white prismatic needles, and is neutral and only slightly
an up-regulation of transforming growth factor beta (TGF-
soluble in water and saturated hydrocarbons. It is highly
). This cytokine has significant immunosuppressive prop-
soluble in lipids and other organic solvents.
but also promotes deposition of matrix proteins and
development of tissue fibrosis. Calcineurin inhibitors have
been shown to be associated with increased intragraft
TGF- levels and development of allograft fi
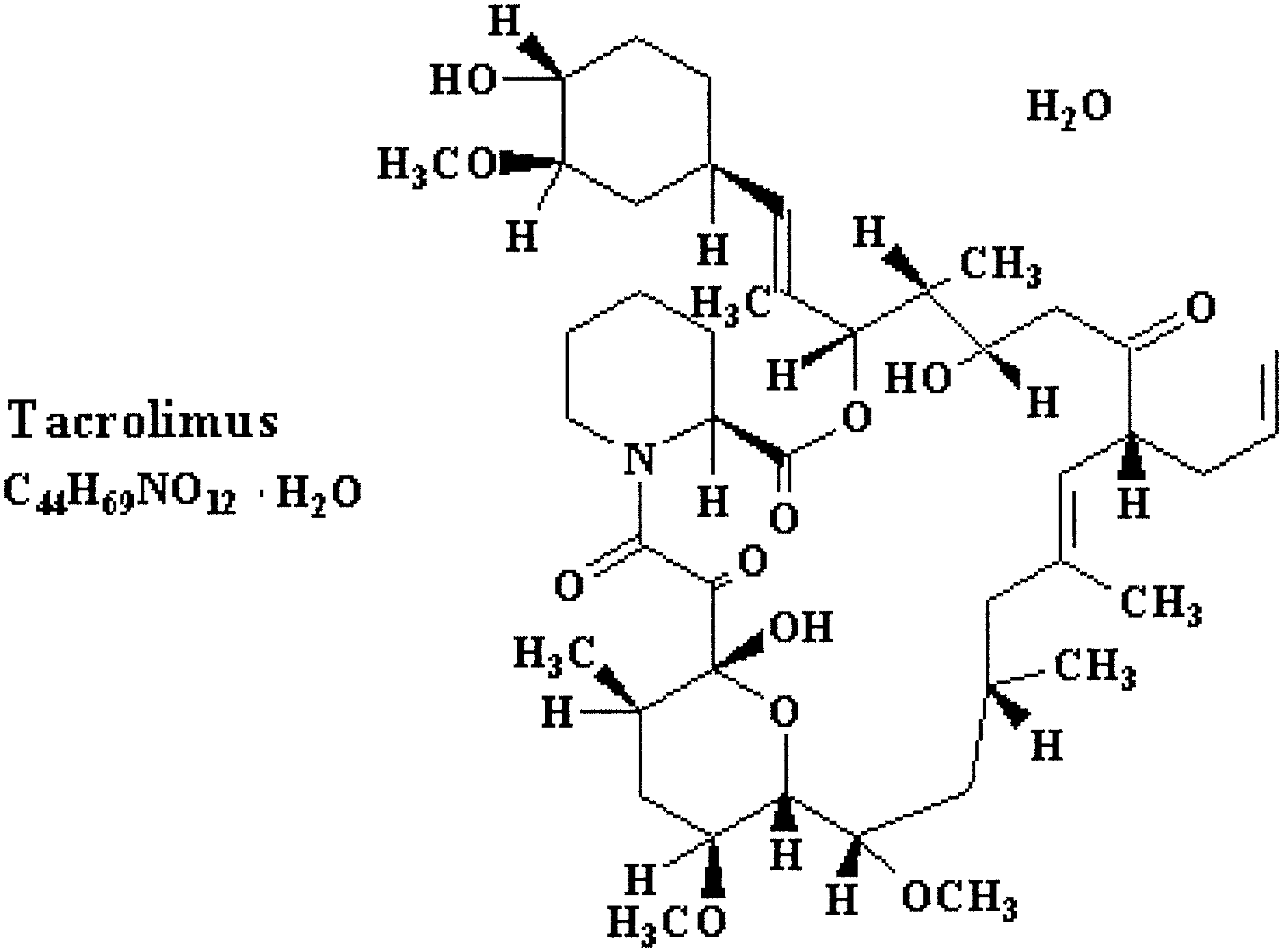
Tacrolimus (C44H69NO12 ⅐ H2O, molecular weight 804,
is a macrolide lactone antibiotic and appears as white
crystals or crystalline powder. It is insoluble in water,
slightly soluble in saturated hydrocarbons, and highly solu-
ble in lipids and other organic solvents.
MECHANISMS OF ACTIONCalcineurin-Dependent Mechanisms
Calcineurin inhibitors exert their cellular effects through
(CP) bind cyclosporine and FK-binding proteins (FKBPs)
bind tacrolimus. Cyclophilin A is the most abundant cyclo-
philin in T lymphocytes, and the predominant tacrolimus-
binding immunophilin is the FKBP12. The CPs and FKBPs
are structurally unrelated but both families have a cis-trans
prolyl-peptidyl isomerase activity. The binding of cyclospor-
ine or tacrolimus to its respective immunophilin enhances
the immunophilin’s affinity to calcineurin. Formation of
These effects seem to be more pronounced for tacrolimus
than and likely contribute to long-term com-
enzyme. Interindividual differences in the total CYP3A4
plications associated with these agents.
activity and the large number of exogenous and endogenous
substances capable of altering its function and expression
explain, in part, the tremendous differences of clearance
Both cyclosporine and tacrolimus have been noted to
rates of cyclosporine. Another factor found to significantly
suppress the immune response in calcineurin-independent
contribute to these differences is the variable expression of
Indeed, cyclosporine and tacrolimus interfere
intestinal P-glycoprotein. P-glycoprotein is a product of
not only in the calcineurin/NFAT pathways but have been
multidrug resistance-1 gene responsible for transport of a
shown to block both the Jun N terminal kinase and p38
wide range of xenobiotics, including calcineurin inhibitors,
signaling These pathways are necessary for
out of the intestinal epithelial cells, therefore reducing their
activation of AP-1 among other transcription The
interference with two distinct mechanisms of T-cell activa-
than 30 metabolites created by hydroxylation, demethyl-
tion contributes to the high specificity of immunosuppres-
ation, sulfation, and cyclization at position 1 without ever
disturbing the cyclic structure of All metab-
olites display only minimal, if any, immunosuppressive
The average half-life of cyclosporine is about 19
It is primarily excreted in bile (Ͼ90%) with less
than 1% contribution of the parent drug. Urine excretion
From the moment of its introduction into clinical practice,
accounts for 6% of the oral cyclosporine dose, of which only
cyclosporine use was plagued by highly variable and difficult
0.1% is Cyclosporine crosses the placenta
to predict bioavailability. It has been amply demonstrated
that the pharmacokinetic properties of cyclosporine can be
of gastrointestinal milieu (bile flow, concomitant ingestion
As with cyclosporine, the absorption of tacrolimus is highly
variable. This leads to various blood concentration pro-
fiIts bioavailability after oral administration ranges
ability in intestinal absorption of cyclosporine was especially
from 5% to 67% with a mean of 29% according to one study
pronounced in its first oil-based formulation (Sandimmun)
of transplant The absorption variability does
with the absolute bioavailability of this form varying be-
not visibly correlate with the type of transplanted organ or
tween 1% and 89% with a mean value of 30% (reviewed by
with age. The clearance, however, appears to be faster in
the pediatric recipient population, requiring administration
sion preparation of cyclosporine (Neoral) led to enhanced
of higher Some ethnic differences were also noted.
bioavailability and more independence from bile secretion.
African-American patients, for example, require higher
Neoral absorption is more rapid reaching 70% to 135%
tacrolimus doses than Caucasians to reach equivalent ther-
higher cyclosporine blood concentrations than Sandimmun
apeutic levels of the Although the absorption of
as measured by maximum blood concentration (Cmax) and
tacrolimus does not seem to be bile-dependent, meals with
area under the time/dose curve The correlation
a moderate content of fat have been shown to reduce the
between the drug dose and AUC was also noted to be
In blood, following intestinal absorption, tacrolimus re-
intrapatient variability in cyclosporine pharmacokinetics
distributes primarily to erythrocytes. The whole-blood con-
was lower for the microemulsion as compared to the oil
centrations are therefore 10 to 30 times higher than that of
Tacrolimus, unlike cyclosporine, does not seem
Due to its strongly lipophilic properties, the majority of
to associate with lipoproteins in plasma and binds to one of
cyclosporine following its intestinal absorption leaves the
the acute phase proteins—the ␣1-acid It
bloodstream. The apparent volume of distribution of cyclo-
readily passes into the fetal and to breast milk.
sporine varies between 4 and 8 Significantly
Tacrolimus undergoes near complete metabolism prior
higher blood concentrations of cyclosporine are noted in
to its elimination. Similar to cyclosporine, the main metab-
leukocyte-rich and fat-rich Within the blood-
olism of tacrolimus occurs via the CYP3A4 system. The
stream, cyclosporine is enriched primarily in erythrocytes
exact number of metabolites is not known, but reported to
(60% to 70%) and leukocytes (9%). The noncellular frac-
be as high as 15 or The main pathways include
tion of blood cyclosporine is carried mainly by lipoproteins
demethylation and hydroxylation with main metabolite
being 31-O-demethyl-tacrolimus, which also possesses im-
Cyclosporine is primarily metabolized by the CYP3A4
munosuppressive Renal excretion accounts for
slightly more than 2% of administered dose with less than
ity of CYP3A4-mediated cyclosporine metabolism occurs in
liver; however, other organs, kidneys and gut mucosa in
In an analogous fashion to cyclosporine, the pharmaco-
kinetic profile of tacrolimus is also affected by the intestinal
concerned, tacrolimus and sirolimus have synergistic in vivo
immunoinhibitory properties due the fact that both drugs
inhibit separate steps in T-lymphocyte The
combination of sirolimus with cyclosporine or tacrolimus
has, therefore, a potential for lower toxicity through utili-
Based on available literature, it is a common assumption
that cyclosporine and tacrolimus drug interactions are
Everolimus, which is the 40-O-hydroxyethyl derivative of
As mentioned above, the pharmacokinetic pro-
sirolimus, is also a substrate of both CYP3A4 and P-
files of both drugs are significantly affected by complemen-
glycoprotein and has, therefore, a potential for competitive
tary influence of both CYP3A4 and P-glycoprotein. It is
interactions with both calcineurin Since its
interesting that drugs that competitively inhibit CYP3A4
biological activity is, as in case of sirolimus, synergistic to
activity also usually act as P-glycoprotein inhibitors, there-
those of cyclosporine and tacrolimus, combining it with
fore increasing the bioavailability of calcineurin inhibitors
calcineurin inhibitors may lead to overall decrease in tox-
and their potential for toxicity. One commonly encountered
icity without affecting transplantation al-
though nephrotoxicity remains a significant problem even at
drugs, like phenobarbital, known to induce CYP3A4 levels
low doses of calcineurin inhibitors.
via activation of gene transcription also tend to up-regulate
levels of decreasing the overall bioavail-
ability of calcineurin inhibitors. This, in turn, can lead to
occurrence of rejection. In addition, the complicity of the
As discussed above, the use of calcineurin inhibitors is
interactions is enhanced by the fact that significant age-,
plagued by considerable intra- and interindividual differ-
gender-, and ethnicity-related differences in the profile of
ences in their pharmacokinetic properties. This makes the
various drug interactions with calcineurin inhibitors have
need of therapeutic drug monitoring a necessary standard
of care to ensure appropriate immunosuppression with
Interaction of Calcineurin Inhibitors With OtherImmunosuppressive Drugs
Corticosteroids, still a part of most immunosuppressive
To date, most transplant centers utilize whole-blood mea-
regimens, have been shown to be substrates, inhibitors, and
surements of cyclosporine trough levels as a means of
inducers of as well as potent inducers of
immunosuppressive monitoring. However, it has been dem-
onstrated that the correlation of “therapeutic” trough levels
and sample collection, corticosteroids have been shown to
with the actual drug or with clinical out-
either lower or increase cyclosporine requirements. The
is relatively poor. The determination of total
clinical importance of these interactions has been stressed
AUC is the most accurate measure of drug exposure, and its
but is not fully Similar concerns are very
values possibly correlate to some degree with the rate of
acute and chronic However, due to the cost
In combination with mycophenolate mofetil, tacrolimus
and inconvenience of multiple blood measurements re-
has been found to be associated with significantly higher
quired for AUC determination, this method is impractical
mycophenolic acid (MPA) trough levels and the total MPA
and several limited sampling strategies have been devel-
exposure (AUC) than when it was coadministered with
oped as surrogates for determination of full AUC utilizing
two or three point measurements with various correlation
cyclosporine decreasing rather than tacrolimus increasing
Currently, prospective studies are underway ex-
amining the utility of a single measurement of 2-hour (C
strated that cyclosporine interferes with enterohepatic re-
cyclosporine level, which has been shown recently to be
circulation of MPA, an effect not observed for tacroli-
associated with renal allograft The utilization
Cyclosporine influences the pharmacokinetics of siroli-
2 levels for monitoring seems to be logical, as the blood
concentrations of cyclosporine during the early postdose
mus by increasing its bioavailability via competitive inter-
period have been shown to correlate well with inhibition of
calcineurin and but is logistically difficult and
verse interaction is insignificant as the concentration of
plagued by a high intraindividual variability.
cyclosporine is approximately 100-fold higher at the inter-
action This interaction is also timing-dependent
with sirolimus concentrations increased to a greater degree
with concomitant cyclosporine administration than when
Unlike the case of cyclosporine, the trough levels of tacroli-
administered several hours Tacrolimus and siroli-
mus correlate reasonably well with and are the
mus have been shown to inhibit each other’s metabo-
most common measure of tacrolimus treatment monitoring.
In addition, as far as the biological activity is
Measurements at other time points, for instance C2 levels,
did not show better correlation with AUC than trough
15. Calne RY, Rolles K, White DJ, et al: Cyclosporin A initially
as the only immunosuppressant in 34 recipients of cadaveric
organs: 32 kidneys, 2 pancreases, and 2 livers. Lancet 2:1033, 1979
16. Powles RL, Barrett AJ, Clink H, et al: Cyclosporin A for the
treatment of graft-versus-host disease in man. Lancet 2:1327, 1978
17. Kino T, Hatanaka H, Miyata S, et al: FK-506, a novel
There is little doubt that over the last 20 years calcineurin
immunosuppressant isolated from a Streptomyces. II. Immunosup-
inhibitors have usurped an as yet uncontested hegemony as
pressive effect of FK-506 in vitro. J Antibiot (Tokyo) 40:1256, 1987
a part of prevention of transplant rejection. Since their
18. Kino T, Hatanaka H, Hashimoto M, et al: FK 506, a novel
introduction, the field of transplantation has left the roam
immunosuppressant isolated from a Streptomyces. I. Fermenta-
of hawkish experimentation and become a universally ac-
tion, isolation, and physico-chemical and biological characteristics.
cepted standard of care for many otherwise terminal disor-
19. Ochiai T, Nakajima K, Nagata M, et al: Effect of a new
ders. Moreover, the use of calcineurin inhibitors has greatly
immunosuppressive agent, FK 506, on heterotopic cardiac allo-
advanced our knowledge about the nature of many pro-
transplantation in the rat. Transplant Proc 19:1284, 1987
cesses involved in immune response. On the other hand, we
20. European FK506 Multicentre Liver Study Group: Random-
have also learned about the dark side of these drugs: the
ised trial comparing tacrolimus (FK506) and cyclosporin in preven-
tion of liver allograft rejection. Lancet 344:423, 1994
significant inter- and intraindividual variability of their
21. The U.S. Multicenter FK506 Liver Study Group: A compar-
pharmacokinetics, the unpredictability of their pharmaco-
ison of tacrolimus (FK 506) and cyclosporine for immunosuppres-
dynamic effects, as well as complexity of interactions with
sion in liver transplantation. N Engl J Med 331:1110, 1994
other agents in transplant recipients. Although the collec-
22. Ellis D: Clinical use of tacrolimus (FK-506) in infants and
tive two decade-long experience with calcineurin inhibitors
children with renal transplants. Pediatr Nephrol J 9:487, 1995
23. Laskow DA, Neylan JF, Shapiro RS, et al: The role of
curbs our appetite for a panacea, it also opens up new
tacrolimus in adult kidney transplantation: a review. Clin Trans-
venues for development of more tailored approaches to
immunosuppression in individual transplant recipients.
24. Bram RJ, Hung DT, Martin PK, et al: Identification of the
immunophilins capable of mediating inhibition of signal transduc-
tion by cyclosporin A and FK506: roles of calcineurin binding and
cellular location. Mol Cell Biol 13:4760, 1993
25. Cardenas ME, Hemenway C, Muir RS, et al: Immunophilins
1. Venkataramanan R, Jain A, Warty VW, et al: Pharmacoki-
interact with calcineurin in the absence of exogenous immunosup-
netics of FK 506 following oral administration: a comparison of FK
506 and cyclosporine. Transplant Proc 23:931, 1991
26. Loh C, Carew JA, Kim J, et al: T-cell receptor stimulation
2. Clipstone NA, Crabtree GR: Identification of calcineurin as a
elicits an early phase of activation and a later phase of deactivation
key signaling enzyme in T-lymphocyte activation. Nature 357:695,
of the transcription factor NFAT1. Mol Cell Biol 16:3945, 1996
3. Flanagan WM, Corthesy B, Bram RJ, et al: Nuclear associa-
27. Northrop JP, Ho SN, Chen L, et al: NF-AT components
tion of a T-cell transcription factor blocked by FK-506 and
define a family of transcription factors targeted in T-cell activation.
4. Fruman DA, Klee CB, Bierer BE, et al: Calcineurin phospha-
28. Shaw KT, Ho AM, Raghavan A, et al: Immunosuppressive
tase activity in T lymphocytes is inhibited by FK 506 and cyclo-
drugs prevent a rapid dephosphorylation of transcription factor
sporin A. Proc Natl Acad Sci U S A 89:3686, 1992
NFAT1 in stimulated immune cells. Proc Natl Acad Sci U S A
5. O’Keefe SJ, Tamura J, Kincaid RL, et al: FK-506- and
CsA-sensitive activation of the interleukin-2 promoter by cal-
29. Timmerman LA, Clipstone NA, Ho SN, et al: Rapid shut-
tling of NF-AT in discrimination of Ca2ϩ signals and immunosup-
6. Kahan BD: Cyclosporine. N Engl J Med 321:1725, 1989
7. Starzl TE, Klintmalm GB, Weil R, et al: Cyclosporin A and
30. Rao A, Luo C, Hogan PG: Transcription factors of the
steroid therapy in sixty-six cadaver kidney recipients. Surg Gynecol
NFAT family: regulation and function. Annu Rev Immunol 15:707,
8. Terasaki PI, Cecka JM, Gjertson DW, et al: A ten-year
31. Henderson DJ, Naya I, Bundick RV, et al: Comparison of
prediction for kidney transplant survival. Clin Transpl 501, 1992
the effects of FK-506, cyclosporin A and rapamycin on IL-2
9. Heusler K, Pletscher A: The controversial early history of
cyclosporin. Swiss Med Wkly 131:299, 2001
32. Johansson A, Moller E: Evidence that the immunosuppres-
10. Borel JF, Feurer C, Gubler HU, et al: Biological effects of
sive effects of FK506 and cyclosporine are identical. Transplanta-
cyclosporin A: a new antilymphocytic agent. Agents Actions 6:468,
33. Frantz B, Nordby EC, Bren G, et al: Calcineurin acts in
11. Calne RY, White DJ, Rolles K, et al: Prolonged survival of
synergy with PMA to inactivate I kappa B/MAD3, and inhibitor of
pig orthotopic heart grafts treated with cyclosporin A. Lancet
34. Aperia A, Ibarra F, Svensson LB, et al: Calcineurin mediates
12. Green CJ, Allison AC: Extensive prolongation of rabbit
alpha-adrenergic stimulation of Naϩ,K(ϩ)-ATPase activity in re-
kidney allograft survival after short-term cyclosporin-A treatment.
nal tubule cells. Proc Natl Acad Sci U S A 89:7394, 1992
35. Tumlin JA, Sands JM: Nephron segment-specific inhibition
13. Kostakis AJ, White DJ, Calne RY: Prolongation of the rat
of Naϩ/K(ϩ)-ATPase activity by cyclosporin A. Kidney Int 43:246,
heart allograft survival by Cyclosporin A. ICRS Med Sci 5:280,
36. Dawson TM, Steiner JP, Dawson VL, et al: Immunosuppres-
14. Calne RY, White DJ, Thiru S, et al: Cyclosporin A in
sant FK506 enhances phosphorylation of nitric oxide synthase and
patients receiving renal allografts from cadaver donors. Lancet
protects against glutamate neurotoxicity. Proc Natl Acad Sci U S A
37. Khanna AK, Hosenpud JD: Cyclosporine induces the ex-
59. Tan KK, Hue KL, Strickland SE, et al: Altered pharmaco-
pression of the cyclin inhibitor p21. Transplantation 67:1262, 1999
kinetics of cyclosporin in heart-lung transplant recipients with
38. Cuhaci B, Kumar MS, Bloom RD, et al: Transforming
cystic fibrosis. Ther Drug Monit 12:520, 1990
growth factor-beta levels in human allograft chronic fibrosis corre-
60. Noble S, Markham A: Cyclosporin. A review of the pharma-
late with rate of decline in renal function. Transplantation 68:785,
cokinetic properties, clinical efficacy and tolerability of a micro-
emulsion-based formulation (Neoral). Drugs 50:924, 1995
39. Khanna A, Cairns V, Hosenpud JD: Tacrolimus induces
61. Kovarik JM, Mueller EA, van Bree JB, et al: Reduced inter-
increased expression of transforming growth factor-beta 1 in
and intraindividual variability in cyclosporine pharmacokinetics
mammalian lymphoid as well as nonlymphoid cells. Transplanta-
from a microemulsion formulation. J Pharm Sci 83:444, 1994
62. Mueller EA, Kovarik JM, van Bree JB, et al: Improved dose
40. Khanna A, Plummer M, Bromberek C, et al: Expression of
linearity of cyclosporine pharmacokinetics from a microemulsion
TGF-beta and fibrogenic genes in transplant recipients with tacroli-
mus and cyclosporine nephrotoxicity. Kidney Int 62:2257, 2002
63. Kahan BD, Dunn J, Fitts C, et al: Reduced inter- and
41. Shihab FS, Tanner AM, Shao Y, et al: Expression of
intrasubject variability in cyclosporine pharmacokinetics in renal
TGF-beta 1 and matrix proteins is elevated in rats with chronic
transplant recipients treated with a microemulsion formulation in
conjunction with fasting, low-fat meals, or high-fat meals. Trans-
42. Shin GT, Khanna A, Ding R, et al: In vivo expression of
transforming growth factor-beta I in humans: stimulation by cyclo-
64. Fahr A: Cyclosporin clinical pharmacokinetics. Clin Phar-
43. Suthanthiran M, Morris RE, Strom TB: Immunosuppres-
65. Hoyer PF, Brodehl J, Ehrich JH, et al: Practical aspects in
sants: cellular and molecular mechanisms of action. Am J Kidney
the use of cyclosporin in paediatric nephrology. Pediatr Nephrol
44. Metcalfe S, Alexander D, Turner J: FK 506 and cyclosporin
66. Misteli C, Rey E, Pons G, et al: Pharmacokinetics of oral
each block antigen-induced T cell receptor signalling that is
cyclosporin A in diabetic children and adolescents. Eur J Clin
dependent on CD4 co-receptor and operates in the absence of
detectable cytoplasmic calcium fluxes. Transpl Int 7(Suppl 1):S549,
67. Kahan BD, Ried M, Newburger J: Pharmacokinetics of
cyclosporine in human renal transplantation. Transplant Proc
45. Metcalfe S, Alexander D, Turner J: FK506 and cyclosporin
A each inhibit antigen-specific signaling in the T cell line 171 in the
68. Lensmeyer GL, Wiebe DA, Carlson IH, et al: Concentra-
absence of a calcium signal. Cell Immunol 158:46, 1994
tions of cyclosporin A and its metabolites in human tissues
46. Matsuda S, Moriguchi T, Koyasu S, et al: T lymphocyte
activation signals for interleukin-2 production involve activation of
69. Ried M, Gibbons S, Kwork D: Cyclosporine levels in human
MKK6-p38 and MKK7-SAPK/JNK signaling pathways sensitive to
tissue of patients treated for one week to one year. Transplant Proc
cyclosporin A. J Biol Chem 273:12378, 1998
47. Matsuda S, Shibasaki F, Takehana K, et al: Two distinct
70. Gupta SK, Benet LZ: High-fat meals increase the clearance
action mechanisms of immunophilin-ligand complexes for the
blockade of T-cell activation. EMBO Rep 1:428, 2000
71. Kolansky G: Cyclosporine formulary considerations. Phar-
48. Matsuda S, Koyasu S: [A second target of cyclosporin A and
FK506]. Tanpakushitsu Kakusan Koso 45:1823, 2000
72. Lemaire M, Tillement JP: Role of lipoproteins and erythro-
49. Matsuda S, Koyasu S: Mechanisms of action of cyclosporine.
cytes in the in vitro binding and distribution of cyclosporin A in the
50. Karin M: The regulation of AP-1 activity by mitogen-
73. Urien S, Zini R, Lemaire M, et al: Assessment of cyclospor-
activated protein kinases. J Biol Chem 270:16483, 1995
ine A interactions with human plasma lipoproteins in vitro and in
51. Cooney GF, Habucky K, Hoppu K: Cyclosporin pharmaco-
vivo in the rat. J Pharmacol Exp Ther 253:305, 1990
kinetics in paediatric transplant recipients. Clin Pharmacokinet
74. Shimada T, Yamazaki H, Mimura M, et al: Interindividual
variations in human liver cytochrome P-450 enzymes involved in
52. Dunn S, Cooney G, Sommerauer J, et al: Pharmacokinetics
the oxidation of drugs, carcinogens and toxic chemicals: studies
of an oral solution of the microemulsion formulation of cyclospor-
with liver microsomes of 30 Japanese and 30 Caucasians. J Phar-
ine in maintenance pediatric liver transplant recipients. Transplan-
75. Haehner BD, Gorski JC, Vandenbranden M, et al: Bimodal
53. Lindholm A, Welsh M, Rutzky L, et al: The adverse impact
distribution of renal cytochrome P450 3A activity in humans. Mol
of high cyclosporine. Clearance rates on the incidences of acute
rejection and graft loss. Transplantation 55:985, 1993
76. Webber IR, Peters WH, Back DJ: Cyclosporin metabolism
54. Schroeder TJ, Hariharan S, First MR: Variations in bioavail-
by human gastrointestinal mucosal microsomes. Br J Clin Pharma-
ability of cyclosporine and relationship to clinical outcome in renal
transplant subpopulations. Transplant Proc 27:837, 1995
77. Saeki T, Ueda K, Tanigawara Y, et al: Human P-glycopro-
55. Friman S, Backman L: A new microemulsion formulation of
tein transports cyclosporin A and FK506. J Biol Chem 268:6077,
cyclosporin: pharmacokinetic and clinical features. Clin Pharmaco-
78. Schinkel AH, Borst P: Multidrug resistance mediated by
56. Lindholm A, Sawe J: Pharmacokinetics and therapeutic drug
P-glycoproteins. Semin Cancer Biol 2:213, 1991
monitoring of immunosuppressants. Ther Drug Monit 17:570, 1995
79. Christians U, Sewing KF: Cyclosporin metabolism in trans-
57. Mehta MU, Venkataramanan R, Burckart GJ, et al: Effect
plant patients. Pharmacol Ther 57:291, 1993
of bile on cyclosporin absorption in liver transplant patients. Br J
80. Radeke HH, Christians U, Sewing KF, et al: The synergistic
immunosuppressive potential of cyclosporin metabolite combina-
58. Cooney GF, Fiel SB, Shaw LM, et al: Cyclosporine bioavail-
tions. Int J Immunopharmacol 14:595, 1992
ability in heart-lung transplant candidates with cystic fibrosis.
81. Yee GC: Recent advances in cyclosporine pharmacokinetics.
82. Maurer G, Lemaire M: Biotransformation and distribution
103. Christians U, Jacobsen W, Benet LZ, et al: Mechanisms of
in blood of cyclosporine and its metabolites. Transplant Proc 18:25,
clinically relevant drug interactions associated with tacrolimus. Clin
83. Venkataramanan R, Starzl TE, Yang S: Biliary excretion of
104. Mathis AS, DiRenzo T, Friedman GS, et al: Sex and
cyclosporine in liver transplant patients. Transplant Proc 17:286,
ethnicity may chiefly influence the interaction of fluconazole with
calcineurin inhibitors. Transplantation 71:1069, 2001
84. Flechner SM, Katz AR, Rogers AJ, et al: The presence of
105. Tuteja S, Alloway RR, Meier-Kriesche HU, et al: The
cyclosporine in body tissues and fluids during pregnancy. Am J
effect of gender on ketoconazole induced changes in tacrolimus
pharmacokinetics. Transplantation 69:S163, 2000
85. Nyberg G, Haljamae U, Frisenette-Fich C, et al: Breast-
106. Rendic S, Di Carlo FJ: Human cytochrome P450 enzymes:
feeding during treatment with cyclosporine. Transplantation 65:
a status report summarizing their reactions, substrates, inducers,
and inhibitors. Drug Metab Rev 29:413, 1997
86. Jain AB, Venkataramanan R, Cadoff E, et al: Effect of
107. Wacher VJ, Wu CY, Benet LZ: Overlapping substrate
hepatic dysfunction and T tube clamping on FK 506 pharmacoki-
specificities and tissue distribution of cytochrome P450 3A and
netics and trough concentrations. Transplant Proc 22:57, 1990
P-glycoprotein: implications for drug delivery and activity in cancer
87. Jain AB, Fung JJ, Tzakis AG, et al: Comparative study of
cyclosporine and FK 506 dosage requirements in adult and pedi-
108. Demeule M, Jodoin J, Beaulieu E, et al: Dexamethasone
atric orthotopic liver transplant patients. Transplant Proc 23:2763,
modulation of multidrug transporters in normal tissues. FEBS Lett
88. Furukawa H, Imventarza O, Venkataramanan R, et al: The
109. Salphati L, Benet LZ: Modulation of P-glycoprotein ex-
effect of bile duct ligation and bile diversion on FK506 pharmaco-
pression by cytochrome P450 3A inducers in male and female rat
kinetics in dogs. Transplantation 53:722, 1992
89. Neylan JF: Racial differences in renal transplantation after
110. Campana C, Regazzi MB, Buggia I, et al: Clinically signif-
immunosuppression with tacrolimus versus cyclosporine. FK506
icant drug interactions with cyclosporin. An update. Clin Pharma-
Kidney Transplant Study Group. Transplantation 65:515, 1998
90. Neylan JF: Effect of race and immunosuppression in renal
111. Hubner GI, Eismann R, Sziegoleit W: Drug interaction
transplantation: three-year survival results from a US multicenter,
between mycophenolate mofetil and tacrolimus detectable within
randomized trial. FK506 Kidney Transplant Study Group. Trans-
therapeutic mycophenolic acid monitoring in renal transplant
91. Beysens AJ, Wijnen RM, Beuman GH, et al: FK 506:
112. Zucker K, Rosen A, Tsaroucha A, et al: Unexpected
monitoring in plasma or in whole blood? Transplant Proc 23:2745,
augmentation of mycophenolic acid pharmacokinetics in renal
transplant patients receiving tacrolimus and mycophenolate
92. Jusko WJ, D’Ambrosio R: Monitoring FK 506 concentra-
mofetil in combination therapy, and analogous in vitro findings.
tions in plasma and whole blood. Transplant Proc 23:2732, 1991
93. Kay JE, Sampare-Kwateng E, Geraghty F, et al: Uptake of
113. Filler G, Zimmering M, Mai I: Pharmacokinetics of myco-
FK 506 by lymphocytes and erythrocytes. Transplant Proc 23:2760,
phenolate mofetil are influenced by concomitant immunosuppres-
94. Warty V, Venkataramanan R, Zendehrouh P, et al: Distri-
114. Vidal E, Cantarell C, Capdevila L, et al: Mycophenolate
bution of FK 506 in plasma lipoproteins in transplant patients.
mofetil pharmacokinetics in transplant patients receiving cyclo-
sporine or tacrolimus in combination therapy. Pharmacol Toxicol
95. Wijnen RM, Ericzon BG, Tiebosch AT, et al: Toxicity of FK
506 in the cynomolgus monkey: noncorrelation with FK 506 serum
115. van Gelder T, Klupp J, Barten MJ, et al: Comparison of the
effects of tacrolimus and cyclosporine on the pharmacokinetics of
96. Venkataramanan R, Swaminathan A, Prasad T, et al: Clin-
mycophenolic acid. Ther Drug Monit 23:119, 2001
ical pharmacokinetics of tacrolimus. Clin Pharmacokinet 29:404,
116. Kaplan B, Meier-Kriesche HU, Napoli KL, et al: The
effects of relative timing of sirolimus and cyclosporine microemul-
97. Alak AM, Moy S: Biological activity of tacrolimus (FK506)
sion formulation coadministration on the pharmacokinetics of each
and its metabolites from whole blood of kidney transplant patients.
117. Lampen A, Christians U, Guengerich FP, et al: Metabolism
98. Moreno M, Latorre A, Manzanares C, et al: Clinical man-
of the immunosuppressant tacrolimus in the small intestine: cyto-
agement of tacrolimus drug interactions in renal transplant pa-
chrome P450, drug interactions, and interindividual variability.
99. Labroo RB, Thummel KE, Kunze KL, et al: Catalytic role of
118. Lampen A, Zhang Y, Hackbarth I, et al: Metabolism and
cytochrome P4503A4 in multiple pathways of alfentanil metabo-
transport of the macrolide immunosuppressant sirolimus in the
small intestine. J Pharmacol Exp Ther 285:1104, 1998
100. Siegsmund MJ, Cardarelli C, Aksentijevich I, et al: Keto-
119. Qi S, Xu D, Peng J, et al: Effect of tacrolimus (FK506) and
conazole effectively reverses multidrug resistance in highly resistant
sirolimus (rapamycin) mono- and combination therapy in prolon-
gation of renal allograft survival in the monkey. Transplantation
101. Schuetz EG, Beck WT, Schuetz JD: Modulators and sub-
strates of P-glycoprotein and cytochrome P4503A coordinately
120. Vu MD, Qi S, Xu D, et al: Tacrolimus (FK506) and
up-regulate these proteins in human colon carcinoma cells. Mol
sirolimus (rapamycin) in combination are not antagonistic but
produce extended graft survival in cardiac transplantation in the
102. Bleck JS, Thiesemann C, Kliem V, et al: Diltiazem in-
creases blood concentrations of cyclized cyclosporine metabolites
121. Crowe A, Lemaire M: In vitro and in situ absorption of
resulting in different cyclosporine metabolite patterns in stable
SDZ-RAD using a human intestinal cell line (Caco-2) and a single
male and female renal allograft recipients. Br J Clin Pharmacol
pass perfusion model in rats: comparison with rapamycin. Pharm
122. Jacobsen W, Serkova N, Hausen B, et al: Comparison of
130. Kahan BD, Welsh M, Schoenberg L, et al: Variable oral
the in vitro metabolism of the macrolide immunosuppressants
absorption of cyclosporine. A biopharmaceutical risk factor for
sirolimus and RAD. Transplant Proc 33:514, 2001
chronic renal allograft rejection. Transplantation 62:599, 1996
123. Nashan B: Early clinical experience with a novel rapamycin
131. Marsh CL: Abbreviated pharmacokinetic profiles in area-
under-the-curve monitoring of cyclosporine therapy in de novo
124. Shaw LM, Holt DW, Keown P, et al: Current opinions on
renal transplant patients treated with Sandimmune or Neoral.
therapeutic drug monitoring of immunosuppressive drugs. Clin
Neoral study group. Ther Drug Monit 21:27, 1999
132. Pescovitz MD, Barbeito R: Two-hour post-dose cyclospor-
125. Barone G, Chang CT, Choc MGJ, et al: The pharmacoki-
ine level is a better predictor than trough level of acute rejection of
netics of a microemulsion formulation of cyclosporine in primary
renal allograft recipients. The Neoral Study Group. Transplanta-
renal allografts. Clin Transplant 16:378, 2002
133. Batiuk TD, Kung L, Halloran PP: Evidence that calcineurin
126. Lindholm A, Kahan BD: Influence of cyclosporine phar-
is rate-limiting for primary human lymphocyte activation. J Clin
macokinetics, trough concentrations, and AUC monitoring on
outcome after kidney transplantation. Clin Pharmacol Ther 54:205,
134. Halloran PF, Helms LM, Kung L, et al: The temporal
profile of calcineurin inhibition by cyclosporine in vivo. Transplan-
127. Bowers LD, Canafax DM, Singh J, et al: Studies of cyclo-
sporine blood levels: analysis, clinical utility, pharmacokinetics, me-
135. Sindhi R, LaVia MF, Paulling E, et al: Stimulated response
tabolites, and chronopharmacology. Transplant Proc 18:137, 1986
of peripheral lymphocytes may distinguish cyclosporine effect in
128. Nankivell BJ, Hibbins M, Chapman JR: Diagnostic utility
renal transplant recipients receiving a cyclosporine ϩ rapamycin
of whole blood cyclosporine measurements in renal transplantation
using triple therapy. Transplantation 58:989, 1994
136. Jusko WJ, Piekoszewski W, Klintmalm GB, et al: Pharma-
129. Stiller C, Keown P: Failure of 125I-tracer selective mono-
cokinetics of tacrolimus in liver transplant patients. Clin Pharmacol
clonal antibody levels on a whole blood matrix to predict rejection
or nephrotoxic episodes in renal transplant patients under anti-
137. Bottiger Y, Undre NA, Sawe J, et al: Effect of bile flow on
lymphocyte globulin and prednisone therapy. Transplant Proc
the absorption of tacrolimus in liver allograft transplantation.
– Nuevas indicaciones auto- rizadas en el año 2001. del Sistema Nacional de Salud Vol. 26–No 1- 2002 Dirección Internet: http://www.msc.es/farmacia/infmedic Manejo de los fármacos en el tratamiento de la depresión A B S T R A C T La farmacología se ha convertido en un componente Pharmacology has become a fundamental component offundamental del tratamiento de los trastorn
PERIODONTAL SPECIALISTS OF INDIANA, PC James T Wolfe, DDS, MSD Burton V Largura, DDS, MSD High quality dental care and patient comfort are our goals . PRESCRIPTION GUIDE Halcion (Take 1 hour before appointment) This medication is used to help you relax. Many patients will sleep through their dental procedure. A common side effect is amnesia, you will probably not remember d
 Pharmacology of Calcineurin Antagonists
Pharmacology of Calcineurin Antagonists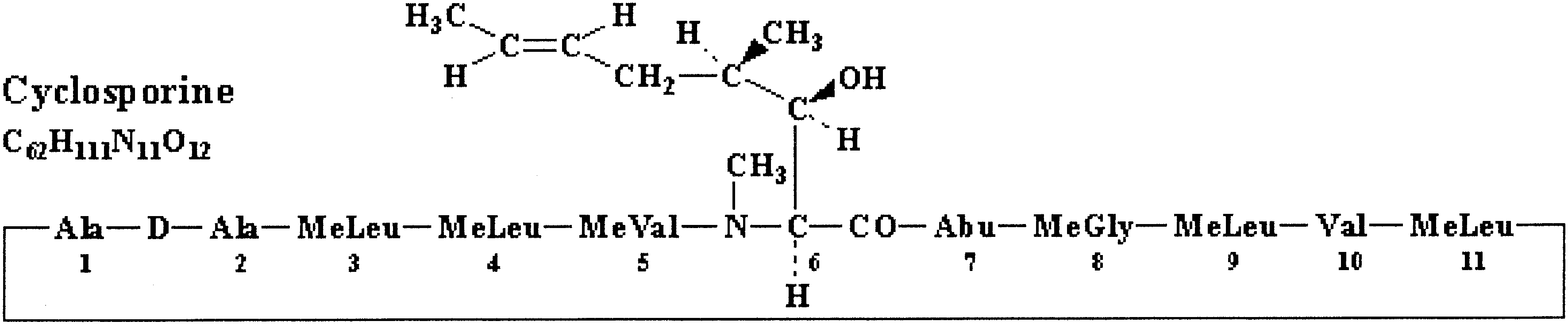
 The screening resulted in discovery of a soil fungus named
such a complex results in its binding to and inhibition of
Streptomyces tsukubaensis in 1984, which produced a potent
In the process of T-cell activation calcineurin,
immunosuppressant given a code FK506 and later named
which is a calmodulin-activated serine phosphatase, associ-
tacrolimus (acronym for Tsukuba macrolide immunosup-
ates with and dephosphorylates inactive nuclear factor of
pressive). In 1987, the results of in vitro testing and first
activated T cells (NFAT). This leads to NFAT translocation
to the nucleus and, in association with other transcription
tially, tacrolimus was evaluated in liver
factors like AP-1, initiation of downstream events involved
and the FDA approved it for the prevention of liver
transplant rejection in April 1994. Subsequently its use was
NFAT family, NFAT1, NFAT2, and NFAT4 participate in
expanded onto transplantation of other as well
transcriptional activation of interleukin-2 (IL-2), IL-4, and
as treatment of atopic dermatitis as a topical formulation.
The screening resulted in discovery of a soil fungus named
such a complex results in its binding to and inhibition of
Streptomyces tsukubaensis in 1984, which produced a potent
In the process of T-cell activation calcineurin,
immunosuppressant given a code FK506 and later named
which is a calmodulin-activated serine phosphatase, associ-
tacrolimus (acronym for Tsukuba macrolide immunosup-
ates with and dephosphorylates inactive nuclear factor of
pressive). In 1987, the results of in vitro testing and first
activated T cells (NFAT). This leads to NFAT translocation
to the nucleus and, in association with other transcription
tially, tacrolimus was evaluated in liver
factors like AP-1, initiation of downstream events involved
and the FDA approved it for the prevention of liver
transplant rejection in April 1994. Subsequently its use was
NFAT family, NFAT1, NFAT2, and NFAT4 participate in
expanded onto transplantation of other as well
transcriptional activation of interleukin-2 (IL-2), IL-4, and
as treatment of atopic dermatitis as a topical formulation.