La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Microsoft word - ferlise.tcnj.paper.doc
“The Demand for Prescription Drugs: An Analysis of U.S. States” Michael Ferlise The College of New Jersey April 19, 2002 Abstract This paper explains the variation observed in consumer spending on prescription drugs among US states. It concludes that expenditures on prescription drugs are primarily a function of public health issues and not the result of differences in access to medical care. Three variables: percentage of the population over sixty-five, the obesity rate and the percentage of the population that smokes account for much of the variation across states in per capita prescription drug use. This suggests that public health programs to reduce obesity levels and smoking rates may have a large effect on I. Introduction
The U.S. spends more than 90 billion dollars a year on prescription drugs alone,
or more than one percent of the entire Gross Domestic Product. Between 1997 and 1999
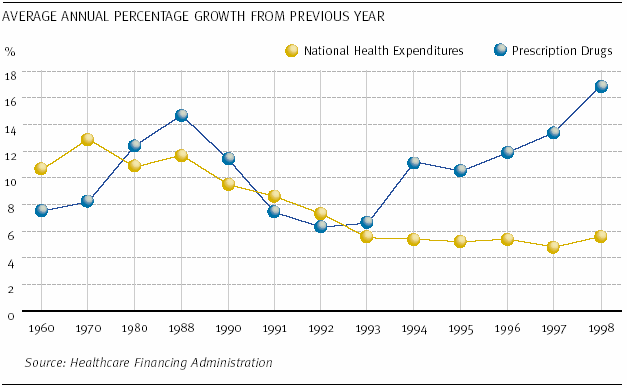
prescription drug expenditures grew nearly 200 times faster than overall national health
expenditures (chart 1). At the turn of the twentieth century, the average US citizen was
spending $327.71 a year on prescription drugs (see Table 1). But per capita prescription
drug use varies widely among the fifty US states. Some states have per capita
prescription drug spending of more than $400 while other states spent half that much.
Thus, it becomes crucial to account for the significant divergence in prescription drug use
between the various states. An accurate understanding of the causes resulting in the
aforementioned variation would permit prescription suppliers to employ a state-specific
rather than national prescription drug program. Likewise it might permit implementation
of public health strategies to reduce spending on prescription drugs. The new state-
specific drug program would ultimately lead to an increase in efficiency and a decrease in
costs to both the suppliers and buyers in the prescription drug market while
simultaneously providing better health care.
This paper explains the variation observed in consumer spending on prescription
drugs among US states. It concludes that expenditures on prescription drugs are
primarily a function of public health issues and not the result of differences in access to
medical care. Three variables: percentage of the population over sixty-five, the obesity
rate and the percentage of the population that smokes account for much of the variation
across states in per capita prescription drug. This suggests that public health programs to
reduce obesity levels and smoking rates may have a large effect on prescription drug use.
II. Background
Suraratdecha (1996) noted the need for a state specific prescription drug program
after reaching the conclusion that, “all states should not be regarded as a single
homogeneous group.” The article also points to the percentage of the population that is
over sixty-five in each state as a possible cause for the variation in prescription drug
usage. If this proves to be the case, the impact of these findings on the prescription drug
Armed with this knowledge, health care providers would be able to better
estimate the needs of their customers in each state. It is an unfortunate truth that as we
increase in age the likelihood of being affected by disease also increases. A
pharmaceutical provider would be able to determine which diseases appear more
frequently among the elderly and in response provide prescription medication more
efficiently, economically and rapidly. In addition to aging, obesity is a significant source
of health problems. Obesity is associated with a variety of risk factors for cardiovascular
disease such as hypertension, elevated cholesterol, and type two diabetes as well as
increased risk of cancer, stroke, osteo-arthritis and other diseases (Must et al. 1999).
Consequently, obesity may contribute to prescription drug use.
Mortimer (1997) considers the effects of managed care in comparison to self-paid
insurance plans. She concluded that managed care sectors have a tendency to be more
price elastic than self-paid sectors. In short, a small change in prescription prices for the
managed care sector results in the substitution of generic drugs for name brand drugs. In
other sectors consumers tended to be less sensitive to price changes and remained loyal to
This could be one possible cause for the variation in prescription drug use noted
above. If it turns out that managed health care sectors are more prevalent in certain areas
of the country, say the South or Midwest, we would be able to postulate, for the time
being, that this is a factor in the variation of drug use in these areas. If a large majority of
the population uses managed health care in the South or Midwest they would be more
inclined to use prescription drugs because of their low cost. This increased use could
possibly result in yet another outcome, that being over diagnosis.
The possibility of over diagnosis is considered by Bonuck, Memmott and Aron
(2001). This article maintains that a reduction in the price of prescriptions leads
individuals, in particular the elderly, to over diagnose themselves. It instills a better safe
than sorry attitude in the elderly in regard to drug usage. In addition, prescription drugs
might serve as a substitute for physician care. States with higher numbers of people per
physician would then have higher prescription drug use.
Lundin (2000) concludes, “that physicians’ habits and tastes acquired by patients
are important.” The knowledge of both the physician and the patient of what drugs are
available play a large role in drug usage. For example if you live in the South a doctor
may give you several prescriptions to combat the common flu, whereas a patient
suffering from the same illness in the North might receive only one prescription from his
physician that is capable of producing the same result.
Kolassa (1995) argues that if a physician was to alter his or her prescribing habits
due to drug prices they might use older drugs because of their low cost, which may result
in the same scenario as above. It would take more low cost alternatives to equal the
results of the higher priced cutting edge drugs. In response, as income increases people
are able to afford more qualified physicians. This results in a lower rate of prescription
drug use due to the physician’s knowledge of superior drugs. Per capita income is also
effective in accounting for the use of discretionary prescription drugs such as Propecia or
acne preventative drugs. As income rises people are able to allocate a larger portion of
income to discretionary drugs or luxury drugs
III. Limitations
Initially one would think of a large number of possible causes for the variation.
Unfortunately, due to the inability to attain, or accurately account for, certain potential
causes the study was limited as to what was included in the analysis. Some possible
causes that did not make the final analysis included the public or societal acceptance of
certain prescription drugs. While the analysis was unable to numerically address this
issue we must be mindful that it may be an influencing factor on the conclusions drawn
herein. In the end, these types of issues would have to be considered using a sensitivity
analysis. Another possible variable that did not make the final analysis was the
substitutability of over the counter medications for prescription medications. An educated
consumer may be aware of possible sicknesses he or she is inflicted with and, rather than
seek a physician’s help, take over the counter medications to combat the illness e.g.
ibuprofen is available in over the counter two hundred mg tablets – the prescription dose
is six hundred mg so some patients would just take three of the two hundred mg tablets
and avoid a visit to the doctors. Again, this data was unavailable and impractical to
generate but may have had some significance in explaining the variation. One final
variable that may have some effect, but also was not included, was the extent of the
physician’s knowledge of the prescription drugs available in the market place. Similar to
what Kolassa (1995) discussed, if a physician is unaware of new prescription drugs he or
she will prescribe older medications that may require larger doses or multiple
IV. Data and Analysis
Based on the discussion above, we regressed per capita prescription drug usage on
per capita income, persons per physician, obesity rate, percentage of the population over
65, percentage of the population without insurance, percentage of the population that
smokes and the percentage of the population that is enrolled in HMOs. Data was
collected from Thomas (2001), The Statistical Abstract of the U.S., and the Center for
Disease Control’s Behavioral Risk Factor Surveillance System. It was expected that as all
of the independent variables increased (except for persons per physician and persons
without health insurance) an increase in per capita prescription drug use would be
observed. It was believed that as the number of persons per physician and persons
without health insurance increased the rate of prescription drug use would decrease.
The initial regression revealed that a two-step regression would be required in
order to compensate for the correlation between several of the independent variables
(Persons Per Physician and Income, Obesity Rate and Income and HMO membership
with income and People Per Physician). The results from the initial regression can be
viewed in table two. These correlations can easily be attributed to the following reasons:
It was expected that as income goes up the number of persons per physician will go down
as indicated by the inverse correlation. This is the result of physicians locating
themselves around high-income densely populated urban regions. Obesity rates and
income were found to be negatively correlated because as per capita income increases
people can afford to purchase healthier foods and also have the ability to allot more time
to exercise due to their increase in leisure time (Sobal and Stunkard, 1989). Since
income and education are also closely related, it can also be assumed that higher income
people are making healthier decisions as income increases, thereby reducing the rate of
obesity in the state. The correlation between income and HMOs is likely the result of
faster increases in medical care costs in high-income states.
The final analysis of the data, as Suraratdecha (1996) anticipated, revealed the
fact that the percentage of the population over sixty-five was most closely correlated to
the rate of prescription drug use in each state. Table 2 shows that a one percent increase
in the population over 65 increases annual per capita spending on prescription drugs by
more than $17. This could be attributable to several factors, one of the most obvious
being, the relationship between getting old and becoming ill. As a person ages, he or she
becomes increasingly susceptible to illness. This is attributable to the fact that after a
person passes the age of roughly twenty-five, the body begins to gradually die as cell
growth begins to slow down. Without the body’s ability to effectively fight off disease
and the effects of aging, a person becomes increasingly reliant on drugs to compensate
for the body’s shortcomings. While the miracle of modern pharmaceuticals has
undisputedly increased life expectancy, the natural consequence is the body’s
components now have to perform for a longer period of time then at any time in our
evolutionary history. The body’s various parts are not suited to the increased longevity
and, as a result, there is a demand for new types of medications for problems caused by
The second independent variable that proved to be helpful in explaining the per
capita expenditures on prescription drugs was the rate of obesity. Table 2 shows that a
one percent increase in obesity increases annual per capita spending on prescription drugs
by more than $7.60. This could be attributable to several factors. As a person becomes
heavier the organs in his or her body become more taxed as carrying out their daily
functions become increasingly difficult. For instance, the energy expelled by a normal
heart in an average sized individual may increase dramatically as the body weight of that
same individual nears obesity and the heart is required to circulate the blood thru an
increasing number of blood vessels. It is this increased workload on the organs that
makes them more prone to failure or reduced efficiency. The individual then becomes
more dependent on prescription drugs to assist the organs in carrying out there daily
functions. Another explanation as to the increase in prescription drugs usage among
obese individuals is their increased likelihood to contract diabetes. Along with the
increases in prescription drug use as a direct result of diabetes, this disease, unfortunately,
increases the bodies chance of contracting other ailments such as heart disease, kidney
failure and vision irregularities. The secondary effects of the disease require additional
expensive medicines to treat complications and can substantially increase expenditures on
prescription drugs for a state having a large number of diabetics. Certain public policies
were recently instituted such as tax deductions for spending on approved weight loss
programs. These types of public policies may persuade members of the obese population
to increase their attempts at losing weight. Currently obese individuals can deduct taxes
on weight loss programs as far back as 1998.
The final independent variable that was helpful in explaining per capita
prescription drug use was the percentage of the population that smokes. A one percent
increase in smokers leads to more than a $4 increase in per capita prescription drug
spending. It is a well-known fact that smoking is detrimental to your health. Studies
have shown that smoking increases the body’s risk of contracting diseases such as Cancer
and Heart Disease. As with obesity, the secondary effects of smoking drastically increase
the amount of per capita prescription drug spending, due in part to the high cost of
medications to treat the secondary diseases resulting from smoking.
Neither people per physician, per capita income, the percentage of uninsured, or
percent enrolled in an HMO had any significant impact on per capita prescription drug
use. The number of people per physician was included under the assumption that as the
rate of people per physician decreases physicians would be better able to monitor their
patients and as a result diagnose them more frequently. This increase in the diagnosis
rate would ultimately lead to an increase in prescription outlays by each individual. It
was expected that based on this increase a negative correlation would appear between the
amounts of people per physician and drug expenditures in each state. This was not the
Per capita income was included because higher income might increase access to
medical care and permit purchases of more expensive medications. Access to medical
care does not seem to be an important determinant of prescription drug expenditures. For
similar reasons, increases in the percentage of the population without health insurance
were expected to decrease the rate of prescription drug use. People without health
insurance must pay full price for their prescriptions and as a result will tend to purchase
The final variable that was used in hopes of explaining the variation in drug use
was the percentage of the population that was enrolled in HMOs. Given that HMO’s tend
to have good prescription drug plans, it was assumed that as the percentage of the
population covered by HMOs increases the rate of prescription drug use would increase.
This would be the result of the availability of low cost prescriptions to HMO members.
As before, this proved not to be the case.
V. Conclusions
The data indicate that expenditures on prescription drugs are primarily a function
of public health issues and not the result of differences in the quality of medical care or
access to physicians. While not every independent variable proved useful in explaining
the variation observed in the dependent variable, we are able to conclude that as the
population ages their reliance on prescription drugs increase. This also holds true for the
rate of obesity, in that as the mean body mass of the population increases the rate of
prescriptions utilized by individuals also increases. The percentage of the population that
smokes was also helpful in explaining the rate of prescription drug use. The recent
introduction of certain public policies (tax deduction for weight loss programs and anti
smoking campaigns) may result in a larger percentage of healthy individuals among the
population thereby decreasing per capita spending on prescription drugs among US
states. Other initiatives to improve public health may also have the effect of reducing
References
Gaquin, Deirdre A. 2000 County and City Extra: Annual Metro, City and County Data Book. 9th edition. 2000 Berman Press. Automated Graphics Systems, Inc., White Plains,
Health Care Financing Administration. http://www.hcfa.gov/stats Kolassa, E.M. “Physicians’ Perceptions of Prescription Drug Price: Their Accuracy and
Effect on the Prescribing Decision.” Journal of Research in Pharmaceutical
Economics. 6(1), 1995, pages 23-37. Lundin , Douglas. “Moral Hazards in Physcian Prescription Behavior.” Journal of Health and
Mortimer, Rika. “Demand for Prescription Drugs: The Effects of Managed Care
Pharmacy Benefits.” University of California, Berkeley. Department of
Must, A., Spadano, J., Coakley, E.H., Field, A., Lolditz, G. & Dietz, W.H. “The Disease
Burden Associated with Overweight and Obesity.” Journal of the American Medical Association, 282, 1999, pages 1523-1529.
National Center for Chronic Disease Prevention & Health Promotion. http://apps.nccd.cdc.gov/brfss/Trends/trendchart_c.asp Thomas, Richard K. Health and Healthcare in the United States. 2001 Nations Health
Corporation. Automated Graphics Systems, Inc., White Plains, MD.
Shapiro, Robert J. Statistical Abstract of the United States: The National Data Book. 120th edition. 2000. US Census Bureau, Washington DC, 2000. Sobal, J. and Stunkard, A.J. “Socioeconomic Status and Obesity: A Review of the Literature.”
Suraratdecha, Chutima. “A Model of State-level Prescription Drug Expenditures in the
USA.” Applied Economic Letters. 1996, pages 289-292.
Appendix Simple Statistics Variable N Mean Std Dev Minimum Maximum OLS and Two Step Regression Analysis Dependent Variable: Per Capita Prescription Drug Use (in dollars) Coefficients: Per Cap Drug Use Per Cap Drug use (Two Step)
t-statistics given in parentheses. * = significant at the 0.1 level, ** = significant at the 0.05 level, *** = significant at the 0.01 level.
Deuxièmes Journées Nationales de Cytométrie en Flux (JNCF 2009) Monastir 15, 16 et 17 janvier 2009 Deuxièmes Journées Nationales de Cytométrie en Flux Faculté de Pharmacie de Monastir: 15-17 janvier 2009 Jeudi 15 janvier 2009 (Atelier Pratique) 08h00 – 09h00 : INSCRIPTION 09h00 – 12h30 : COURS 09h00 - 10h30 : Cours 1 (Claude LAMBERT): Principes
Comments received from I&APs on the proposed Desert Star South Development (by 8 September 2010) ______________________________________________________________________________ From: Ranwedzi Mashudu [mailto:RanwedziM@dwa.gov.za] Sent: 08 September 2010 02:51 PM To: Lima Maartens Subject: RE: Re comment period for DSS Scoping Report Hi Lima Unfortunately there are still
 Appendix
Appendix