La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
11207-05
Systemic therapy of psoriasis: methotrexate
Department of Dermatology, Faculty of Medicine, University Hospital, Bratislava, Slovakia. Abstract: Methotrexate is the first line therapy for the treatment of moderate to severe psoriasis and psoriatic arthritis all over the world. It has immunosupressive and anti-inflammatory effects. If we want to use it, we have to know its mechanism of action and also its possible toxicity and how to cope with it (Tab. 3, Fig. 1, Ref. 14). Full Text in free PDF www.bmj.sk. Key words: methotrexate, psoriasis, folic acid.
Methotrexate is the antagonist of folic acid. It belongs to the
first line treatment in Europe concerning the systemic treatmentof psoriasis. It has immunosuppresive, cytostatic and antiinflam-
matory effects. In dermatology, it started to be used in 1971. Almost forty years of experience are granting good knowledgeof its effects on psoriasis, but also of the side effects, incidenceof which varies depending on the treatment length, methotrexate
dose and supplementation of folic acid. Even thought it is on themarket for a long time, its effect on psoriasis is often unpredict-able. There are patients, who react on the treatment satisfacto-rily, but also patients who do not react at all. After a 12-week
treatment dosed 15 mg/week, 24 % of patients achieve PASI 75. In a direct comparative study on the biological agent adalimumab,with slowly increasing dose from 7.5 mg up to 22.5 mg/week,only 3 % of patients achieved this in 16th week of treatment. In
present, it is used for the treatment of moderate psoriasis, re-spective when local therapy is insufficiency.
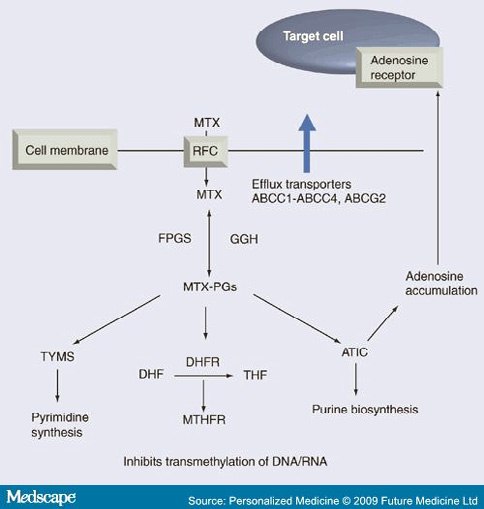
Methotrexate (Fig. 1), like the folic acid, binds to the same
transmembrane protein RFC (reduced folate carrier) and is trans-ported into the cell. In the cell membrane, also an active trans-
Fig. 1. Methotrexate mechanism of action (3).
port proteins exist, that evict the methotrexate out of the cell. Incytoplasm, the methotrexate is activated by the enzyme FPGS
the influence of enzyme gama-glutamylhydrolase, resulting in
(folylpolyglutamate syntetase) by polyglutamation. By the same
the creation of the former molecule of methotrexate. The active
enzyme, the folic acid is processed with the result of
form of methotrexate (polyglutamate) is responsible for its tar-
polygutamates of folic acid, which serve as the deposit for the
get effects in the cell. The most important effect of methotrexate
cell. Almost 50 % of the folic acid is stored in the body in the
is evoked by a blockade of dihydrofolate-reductase (DHFR). This
form of polyglutamates deposited in hepatic cells. One molecule
enzyme plays an important role in the metabolism of folic acid
of methotrexate can bind from 2 up to 7 glutamates. This pro-
by activating it to tetrahydrofolate (TFH). The blockade of this
cess is reversible. Methotrexate glutamates can be splintered by
enzyme leads to reduction in the creation of tetrahydrofolate.
Tetrahydrofolate is the important substrate for the de novo cre-
Department of Dermatology, Faculty of Medicine, University Hospital,
ation of purine and pyrimidine bases. This reduction is enhanced
by the inhibitory effect of methotrexate on another important
Address for correspondence: MUDr. Peter Kozub, Department of Der-
enzyme, tymidilate syntasis (TYMS), which is responsible for
matology, Faculty of Medicine, University Hospital, Bratislava, Slovakia.
the transformation of uridilate to tymidilate. The ending result
Indexed and abstracted in Science Citation Index Expanded and in Journal Citation Reports/Science Edition
Kozub P, Simaljakova M. Systemic therapy of psoriasis: methotrexate
of inhibitory influence of methotrexate on the enzymes mentioned
Tab. 1. Dosage of folic acid number of European dermatologists,
above is the blockade of DNA and RNA synthesis. Anti-inflam-
matory effect is induced by inhibition of other important enzyme,aminoimidazole-4-carboxamide ribonucleotide transformylase.
Its blockade leads to accumulation of adenosine, an important
5 mg on the 4th day after the last dose of MTX
Methotrexate is used after fasting. Two forms exist oral
and parenteral. In dermatology, we use only methotrexate pills,
equate treatment in simultaneous joint disability. Cyclosporine
although the recent studies with methotrexate dosed subcutane-
also has an effect on joints, but it is achieved later than effects
ously in patients with rheumatic arthritis (4) showed a higher
on skin (approximately after 23 months), and does not have to
efficiency of subcutaneously applied methotrexate compared to
be sufficient. Methotrexate is the ideal drug in treatment of pa-
methotrexate dosed as pills and might indicate the future change.
tients with nummular chronic psoriasis and with severe joint dis-
After the oral dose, the maximal concentration in blood is
achieved in 12 hours. Depending on the dose, the biological
availability could be as high as 60 %. Elimination occurs mostly
by urine (more than 90 %), dosing in patients with renal diseaseshave to be reduced.
Methotrexate adverse effects could be divided into few
1. myelosuppression the most feared side effect of methotrex-
ate, which tends to occur in the beginnings of treatment. The
The weekly dose of methotrexate in patients with psoriasis
result is attenuation of bone marrow and pancytopenia. Because
varies from 7.5 mg to 22.5 mg. It starts with the lowest, so-called
of this, the starting dose of methotrexate is administered in re-
test dose of 5 or 7.5 mg for week, and after a week the blood
duced form and after a week the blood samples are checked.
samples are taken (biochemistry and blood count) for a possible
Pancytopenia is very rare. If it occurs, the treatment with meth-
occurrence of side effects. The most dangerous is myelosuppre-
otrexate has to be stopped immediately, and possibly the anti-
sion, which could be lethal to the patient. If the tests are within
dote is to be administered calciumfolinate.
normal levels, the dose of methotrexate could be raised. Labora-
2. hepatotoxicity is given by increasing the hepatic enzyme
tory parameters are checked frequently (blood count, hepatic
levels up to 23 times. It occurs pretty frequently and is com-
enzymes, renal parameters) and the patient is checked for pos-
monly dependent on the dose of methotrexate. The treatment
sible side effects on skin and mucous membranes, respective the
has not to be interrupted and usually a lowering of dose is suffi-
subjective tolerance of the dose from the gastrointestinal point
cient, or hepatoprotectives are to be added into treatment. The
of view is observed. The dose is adjusted according to the needs.
recommendations of world known dermatologists prevailed for
Two ways of dosing are used. American school prefers the drug
a long time due to an increased risk of hepatic fibrosis during
administration split into three doses of 12 hour intervals. This
long-time dosing of methotrexate, hepatic biopsies were taken
type is common in our country too. English school prioritizes
after achieving the cumulative dose of 1.5 g, but in present this
drug administration in a single day in the morning and evening,
recommendation is considered obsolete. Actually it is enough if
with a lower dosage even one-time only (Tab. 1).
the levels of hepatic enzymes are checked, abdominal ultrasoundperformed and the level of aminoterminal peptide procolagene
III (PIIINP) in serum observed. If the normal levels are achieved
repeatedly, the risk of significant hepatic fibrosis is negligible.
Methotrexate is indicated for the treatment of nummular
Levels of PIIINP should be checked every 34 months. If the
chronic psoriasis and psoriatic arthritis. It is not suitable for treat-
levels increase, the liver tissue samples should be taken by bi-
ing acute conditions (erythrodermia, generalized pustulous pso-
riasis, exudative psoriasis), in which systemic corticoid therapy
3. gastrointestinal adverse effects (diarrhea, nausea, abdomi-
is preferred. Methotrexate starts operating within a month and
nal pain) occurs mainly due to high dosage. They are relative
its effect fully develops after two months. From this reason it is
common and when they occur, the dose of methotrexate should
a great additive to systemic corticoid therapy. Serious acute state
is suppressed by corticoids, which are later dropped. The effi-
4. skin and mucous membrane adverse effects (ulcers in mouth
ciency of methotrexate is relatively lower, but it depends on
cavity, stomatitis, cheilitis, alopecia, exanthemas) are relatively
a patients weight, dose, the speed of increasing the dose and
common as well and dosage-dependent. If they occur, the dos-
dosage of folic acid. It has the most sovereign effect on joints
age should be adjusted. They are not the reason to terminate the
among the first-line treatment. Neotigason is absolutely inad-
390 3945. teratogenic effects contraception is required during the treat-
Tab. 2. Peroral methotrexate available in Slovakia since 1.10.2009 (14).
ment with methotrexate, it also should be provided for the nextthree months after the end of treatment. The frequency of menses
is checked and pregnancy test should be taken if suspicious.
6. mutagenic effects continuous phototherapy is not recom-
mended because of the possible increased risk of skin carcinoma.
Restrictions during methotrexate administration (5)
During the treatment, patients are prohibited to drink alco-
holic beverages. They cannot use some drugs simultaneously,
for example non-steroid antiflogistics, which are used frequently
by patients with synchronous psoriatic arthritis. Non steroid anti-
flogistics increase and extent serum levels of methotrexate and
could significantly increase the risk of severe hematologic and
gastrointestinal toxicity. Methotrexate is bounded to albuminsin serum and drugs, which interact with the same bonds (salicy-
lates, fenylbutazone, fenytoine, sulphonamides), could increase
Tab. 3. Folic acid available in Slovakia since 1.10.2009 (14).
its toxicity. Oral antibiotics (tetracycline, chloramphenicol) and
non-absorbable wide-spectrum antibiotics could lower the ab-
sorption of methotrexate by gastrointestinal tract. Penicillin could
also reduce the renal excretion of methotrexate. Higher attention
should be paid to patients using other potentially hepatotoxic
drugs (leflunomid, azathioprine, retinoids, sulphasalazine). Dur-ing the treatment the vaccination is not recommended.
practice such a dosing is unreal due to dosage of folic acid only
by 10 mg and small pills, which could not be split easily becausethe pills does not have the splitting gap. Other problem could
First blood samples (blood count, laboratory values) are taken
result from the weekly dose of folic acid. It is different, when
after a week of treatment. Frequency of following blood checks
patient takes 30 mg of folic acid during the methotrexate dosage
depends on the speed of dose increment, they should be per-
of 7.5 mg/week or 15 mg/week. In the first case we significantly
formed at least once a month in first three months of treatment.
reduce the risk of potential side effects, but at a cost of lowering
After balancing the dose and physiological levels in blood
its effect. In the second case the effect should be better, but its
samples, these intervals could be elongated. In the blood count
toxicity could rise. Due to that, the dosage of folic acid should
we follow the numbers of erythrocytes, leucocytes, neutrophiles,
be adjusted to individual needs of patient.
the middle volume of erythrocyte and from the laboratory val-
In the case that patient is treated by methotrexate only, se-
ues hepatic and renal parameters. In the case of rising levels of
rum levels of folic acid could decrease and secondarily the middle
the middle volume of erythrocytes, we can check the levels of
volume of erythrocytes could rise. Heavy pancytopenia could
folic acid and B12. At least once a year patient should undergo
occur from a grave deficit of folates. Despite that not every der-
abdominal ultrasound. Also, aminopeptide procolagene III is not
matologist uses the folic acid. During the spring symposium
the part of routine check, but after repeatedly higher levels of
EADV 2009 in Bucurest the practice of European dermatolo-
hepatic enzymes and positive hepatic ultrasound it should be
gists was presented (6): Only 32 % of dermatologists commonly
use the folic acid daily during treatment with methotrexate, next32 % only during specific circumstances (i.e. a rise in the middle
volume of erythrocytes) and the rest 36 % does not use the folicacid at all. Various weekly dosages of folic acid were presented;
Methotrexate is an antagonist of folic acid. Methotrexate and
the results are to be seen in the Table 1. In the results it is shown
folic acid competes against each other to bind on the same re-
that even European dermatologists are consistent about the dose
ceptor. Folic acid has been added into the treatment to lower the
of folic acid (in most European countries the dosage of 5 mg is
possible undesirable side-effects. By adding the folic acid we
available in single pills, instead of Slovakia), the weekly dose is
also lower the immunosuppressive and anti-inflammatory effect
not uniform and probably the randomized blinded trials will be
of methotrexate. Commonly the axiom states that 5 mg of folic
needed to get the results of optimal dosage scheme. Dermatolo-
acid is administered per day, missing out on days when methotr-
gists have agreed that the supplementation of folic acid during
exate is dosed. If we assume that methotrexate is dosed once or
the treatment with methotrexate should be realized during the
twice per week, other days the folic acid should be taken. In our
whole time of treatment. If the higher levels of middle volume
Kozub P, Simaljakova M. Systemic therapy of psoriasis: methotrexate
of erythrocytes over 106 fl persist, treatment with methotrexate
It is also important to remember, that even though the supple-
mentation of folic acid lowers the efficiency of methotrexate, it
The majority of patients with psoriasis has lower levels of
primarily lowers the immunosuppressive effect. Anti-inflamma-
folic acid and a higher middle volume of erythrocytes. The com-
tory effect of methotrexate is not bonded to folate metabolism,
parative trial CHAMPION, in which the effects of adalimumab
but probably to inhibition of aminoimidazole karboxamide ribo-
and methotrexate were evaluated, supports the fact that only folic
nucleotide transformylamylase, which results in accumulation
acid by itself in monotherapy could bring some benefit for the
of adenosine, which is one of the main elements of the anti-in-
patient. The dose of methotrexate was increased from 7.5 mg up
to 22.5 mg in 16th week when needed. Together with methotrex-
Adjuvant therapy with folic acid during the methotrexate
ate, the folic acid was administered in a dose of 5 mg/day. Pa-
treatment definitely has its meaning. It significantly reduces the
tients dosed with placebo also received the folic acid treatment
hepatotoxicity and mildly the gastrointestinal and skin respec-
in a dose of 5 mg/day. The last group of patients reached PASI
tive mucosal adverse effects and only minimally influence the
75 in 16th week as high as 18.9 %. It is too high number for the
methotrexate efficiency. It is necessary to adequately adjust the
placebo group, but these patients also received the folic acid treat-
dosages of both drugs to actual needs of patient.
ment, high probability is that the folic acid itself has some posi-tive effect in treatment. Theoretically it could mean that every
patient (regardless the treatment) could get folic acid as
a supplement to systemic, local or biological treatment or pho-
Methotrexate has an irreplaceable role in biological treat-
totherapy. Other trials are needed to confirm the beneficial ef-
ment of psoriasis and psoriatic arthritis. It is used mainly during
fect of folic acid on psoriasis. Folic acid was added to methotr-
the treatment with TNFá blockers, especially treatment with
exate treatment to lower the possible side effects. French au-
infliximab. With its cytostatic effect, methotrexate blocks B-lym-
thors Prey and Paul (7) analyzed 6 double blinded placebo con-
phocytes and decreases the production of antibodies against
trolled trials focused on the effects of folic acid ror foline acid
infliximab. Antibodies against infliximab have neutralizing char-
on the safety and efficiency of methotrexate treatment in patients
acter and are able to lower the efficiency of methotrexate, but
with rheumatoid arthritis and with psoriasis with or without pso-
also can induce infusion reactions. Even if the concentration of
riatic arthritis. They founded that gastrointestinal (diarrhea, nau-
antibodies against infliximab is not examined as a standard, its
sea, abdominal pain) and skin (respective mucosal) adverse ef-
increased values could result in decreasing of its effect. During
fects (ulcers in mouth cavity, stomatitis, alopetia, exanthemas)
the treatment with infliximab, two ways of failure can occur: (1)
were only mildly lowered, but hepatotoxicity, defined as eleva-
infliximab does not tighten up its effect meaning that patient
tion of alaninaminotraspherase up to double the normal levels,
will get better after the infusion dosage, but this improvement
was significantly reduced thanks to the supplementation with
lasts only 46 weeks, after which the gradual deterioration oc-
folic and foline acid by 35.8 %. Hematological adverse effects
curs, but after the next infusion, the patient will get temporarily
(neutropenia, lymphopenia, and anemia) could not be evaluated
better again, (2) infliximab effect is not adequate patient does
because of its rare occurrence, but the significant reduction was
not get better despite the infusion treatment, vice-versa to worse
not reached depending on dosage or not of folic/foline acid in
manifestation. The solving of the first case is based on shortage
the patients that expressed these hematological side effects. The
in intervals of infusion dosage to 46 weeks, solving the second
results showed that the supplementation of folic/foline acid sig-
case is the methotrexate. Adding of methotrexate lowers the con-
nificantly decreased the hepatotoxicity of methotrexate and
centration of neutralizing antibodies against infliximab, also its
mildly decreased its gastrointestinal, resp. skin/mucosal adverse
immunosuppressive and anti-inflammatory effect takes place.
effects. The influence on the myelotoxicity was not significant.
Similarly as in the methotrexate monotherapy, we start with an
The dosage of folic acid used in the mentioned studies was ei-
induction dose of 7.5 mg/week. If after one week, the bone mar-
ther 1 or 5 mg daily and the foline acid 15 mg/week. Concur-
row attenuation is not observed, the dosage is increased ad-
rently the effect of these acids on the methotrexate efficiency
equately. The possible preventive effect of methotrexate on
was observed. The results showed that in patients with rheuma-
the infusion reactions for a long time during the treatment with
toid arthritis both acids had mildly negative effect on methotrex-
infliximab is considered. Many studies have proved its benefit,
ate, but in patients with psoriasis this effect was not so clear.
even if the infusion reactions did not occur in the group of pa-
Authors also dealt with the dosage of acids. Only in one trial the
tients treated by methotrexate. Time factor is very important.
two doses of folic acid (27.5 mg/week vs 5 mg/week) were com-
The full effect of methotrexate can be expected as soon as in
pared, but it was not achieved that the higher dose is more effi-
two months. Crandall and Mackner found out that the risk of
infusion reactions was significantly lower after 4 months of
Some results suggested that patients with higher weight need
simultaneous therapy with methotrexate and infliximab (9).
either the higher dose of methotrexate or lower doses of folic
After adding the methotrexate to infliximab or other TNFá
acid. Other trials are needed to confirm these observations. It is
blocker, we pay more attention to the levels of hepatic enzymes,
on the dermatologist himself to adjust the dose of methotrexate
because the combination of two increases the risk of hepato-
and folic acid depending on the patients needs.
390 394Farmacogenetics of methotrexate
Farmacogenetics of methotrexate deals with the response on
1. Flytstrom I et al. Methotrexate vs. ciclosporin in psoriasis: effective-
treatment and genetically based variability. It follows simple
ness, quality of life and safety. A randomized controlled trial. Br J Der-matol 2008; 158: 116121.
nucleotide polymorphisms (SNP) of genes of those enzymes,
transport proteins, effector proteins or receptors, which are the
2. Saurat JH et al. Efficacy and safety results from the randomized
part of the drug effect. It also follows their relationship to effi-
controlled comparative study of adalimumab vs. methotrexate vs. place-bo in patients with psoriasis (CHAMPION). Br J Dermatol 2008; 158:
ciency and toxicity of the drug. In case of methotrexate (used to
treatment of psoriasis), the following proteins and their poly-
3. Hughes LB et al. Recent advances in rheumatoid arthritis therapy
FPGS polymorphism without influencing the efficiency
and management: recent advances in predictors of efficacy and toxicity. www.medscape.com
GGH polymorphism without influencing the efficiency or
4. Braun J et al. Comparison of the clinical efficacy and safety of sub-
cutaneous versus oral administration of methotrexate in patients withactive rheumatoid arthritis: results of a six-months, multicenter, rando-
MTHFR polymorphism C677T, A1298C without influ-
mized, double-blind, controlled, phase IV trial. Arthritis Rheum 2008;
encing the efficiency or toxicity (10), compared to patients with
rheumatoid arthritis, where both polymorphisms are associated
5. Methotrexat-Lachema, súhrn charakteristických vlastností lieku
with an increased risk of adverse effects,
ATIC polymorphism C347G without influencing the ef-
ficiency or toxicity (10), more frequent end of treatment (12),
6. Boffa M. Methotrexate for psoriasis an update. Spring symposiumEADV Bucharest 2009.
ABCC1 (transmembrane protein evicting the methotrexate
out of the cell) polymorphism in the area of this gene is associ-
7. Prey S, Paul C. Effect of folic or folinic acid supplementation on
ated with good response on methotrexate (11),
methotrexate-associated safety an efficacy in inflammatory disease:
ABCG2 (other transmembrane protein evicting the methotr-
a systematic review. Br J Dermatol 2009; 160: 622628.
exate out of the cell) polymorphism in the area of this gene is
8. Dervieux T et al. Polyglutamation of methotrexate with common
associated with good response on methotrexate and early inci-
polymorphisms in reduced folate carrier, aminoimidazole carboxamide
ribonucleotide transformylase and thymidilate synthase are associatedwith methotrexate effects in rheumatoid arthritis. Arthritis Rheum 2004;
RFC (reduced folate carrier) polymorphism 80A in-
9. Crandall WV, Mackner LM. Infusion reactions to infliximab in chil-dren and adolescents: frequency, outcome and a predictive model. Ali-
Other methods then pharmacogenetic are used to evaluate
ment Pharmacol Ther 2003; 17: 7584.
an increased or decreased efficiency of methotrexate, respectiveto distinguish the responders from non-responders during the
10. Warren RB et al. Outcomes of methotrexate therapy for psoriasis
treatment of psoriasis vulgaris. Czech authors (13)
and relationship to genetic polymorphisms. Br J Dermatol 2009; 160:
possibility to evaluate the concentration of methotrexate poly-glutamates in erythrocytes and correlate this concentration with
11. Warren RB et al. Genetic variation in efflux transporters influences
efficiency and toxicity of methotrexate. Their pilot study did not
outcome to methotrexate therapy in patients with psoriasis. J Inv Der-matol 2008; 128: 19251929.
confirm a direct correlation of levels of methotrexate polyglu-tamates with the changes of PASI (Psoriasis Area and Severity
12. Campalani E et al. Polymorphisms in folate, pyrimidine and purine
metabolism are associated with efficacy and toxicity of methotrexate inpsoriasis. J Inv Dermatol 2007; 127: 18601867.
13. Hroch M et al. A pilot study of pharmacokinetically guided dosingof oral methotrexate in the initial phase of psoriasis treatment. JEADV2007; 22: 1924.
Methotrexate belongs to the first line of therapy in a systemic
treatment of psoriasis. It does not belong to the most efficient
14. MZ SR. Zoznam liekov a lieèiv plne uhrádzaných alebo èiastoène
antipsoriatic drugs, but its advantage is very good effect on po-
uhrádzaných na základe verejného zdravotného poistenia: http://
tential psoriatic arthritis. Other advantage is the price. Compared
to acitreine or ciclosporine it is much cheaper. With a good man-
agement it is relatively safe, even though the occurrence of pos-
sible adverse effects is higher and dose-dependent. Despite thatthe patients with coincident joint pain and biologically treatedpatients profit from the treatment with methotrexate. In both casesthe methotrexate has an irreplaceable position.
Recommendations for diagnosis and treatment of Lyme borreliosis: guidelines and consensus papers from specialist societies and expert groups in Europe and North America Sue O'Connell, Health Protection Agency Lyme Borreliosis Unit, HPA Microbiology Laboratory, Southampton University Hospitals NHS Trust, Southampton SO16 6YD Introduction European and American Lyme Borreliosis Diagnos
SPECIALTY MEDICATIONS available through Accredo Health Group, Inc., Medco’s specialty pharmacy Call toll-free (800) 803-2523, 8:00 a.m. to 8:00 p.m., eastern time, Monday through Friday, to confirm that your medication is covered. Effective as of January 1, 2011 Abraxane® (paclitaxel protein-bound particles) Berinert® (C1 esterase inhibitor [human])* Carimune® NF (immune globulin
 Systemic therapy of psoriasis: methotrexate
Department of Dermatology, Faculty of Medicine, University Hospital, Bratislava, Slovakia.
Systemic therapy of psoriasis: methotrexate
Department of Dermatology, Faculty of Medicine, University Hospital, Bratislava, Slovakia.