La tétracycline, connue sous le nom commercial Sumycin, agit en bloquant la fixation de l’ARNt sur la sous-unité 30S ribosomale, interrompant l’élongation de la chaîne protéique bactérienne. Ce mécanisme confère une activité sur un spectre large, incluant bactéries Gram positives, Gram négatives, rickettsies et spirochètes. Sa biodisponibilité digestive varie selon la prise alimentaire et les interactions avec les ions divalents comme calcium et magnésium. Sa diffusion tissulaire est importante, notamment dans les voies respiratoires et génito-urinaires. L’élimination se fait par voie rénale et biliaire. Les effets indésirables incluent photosensibilisation, troubles digestifs et coloration dentaire en cas d’administration précoce. Les guides thérapeutiques mentionnent sumycin prix, en soulignant la nécessité de restreindre son utilisation afin de limiter les résistances acquises.
Untitled
Acta Orthop. Belg., 2005, 71, 29-35 Anastomosis between the median and ulnar nerve in the forearm An anatomic study and literature review
Konstantin J. KAZAKOS, Anastasios SMYRNIS, Konstantin C. XARCHAS, Alexandra DIMITRAKOPOULOU,
From the Orthopaedic Department, Democritus University of Thrace, Alexandroupolis, GreeceAnastomosis between the median and ulnar nerve in
and finally in the palm between the recurrent
the forearm has been shown to be of clinical signifi-
branch of the median and the deep branch of the
cance. We aimed to determine the presence of medi- an to ulnar nerve communications in the forearm of
Martin (13) was the first to report such an anasto-
the Greek population by anatomical studies. At the
mosis in 1763. He described a branch between the
same time we defined the types and patterns of the
median and ulnar nerves that “sometimes runs
anastomoses found and compared them to those
under the pronator teres muscle”. He also described
reported in similar studies that were retrieved after a wide review of the literature. One hundred and
a connection between median and ulnar nerves in
sixty three forearms from 100 cadavers (53 males,
the palm, the “arcus volaris nervorum”. Martin
47 females, 25-91 years old) were carefully dissected
made no comment on the content of these connect-
to observe median and ulnar nerve communication.
ing branches, whether they were motor or sensory. The anastomosis was found in 10 cadavers ; it was
He did not speculate on the final destination of
bilateral in 4 and unilateral in 6, on the right side in
their fibers. Gruber (6) was apparently the next to
four and on the left side in two. It occurred in 7 of the
mention these findings, in 1870. He dissected
53 male cadavers (14%) and in 3 of the 47 females
212 forearms and found a connection between
(6,5%). Overall, the anastomosis was found in 14 of
median and ulnar nerves in 38. The nerve branches
the 163 forearms (8,6%). No case of ulnar to median
generally coursed from the median nerve proximal-
nerve anastomosis in the forearm was found in
ly to the ulnar nerve distally. Gruber never
anatomical examination.
■ Konstantin J. Kazakos, MD, Assistant Professor. INTRODUCTION
■ Anastasios Smyrnis, MD, Orthopaedic Surgeon. ■ Konstantin C. Xarchas, MD, Lecturer.
■ Alexandra Dimitrakopoulou, MD, Orthopaedic Resident.
nerve are known as the most common form of
■ Dionysios-Alexandros Verettas, MD, Associate
“anomalous” innervation. These anastomoses in
Orthopaedic Department, Democritus University of Thrace,
the forearm and hand provide variations in the
innervation of the intrinsic hand muscles, as proved
Correspondence : Konstantin C. Xarchas, Democritus Univer-
by anatomical and nerve conduction studies (11, 12).
sity of Thrace, 6 I. Kaviri rd, 68100 Alexandroupolis, Greece.
Such anastomoses have been reported in the upper
part of the forearm, rarely in the distal forearm
Acta Orthopædica Belgica, Vol. 71 - 1 - 2005
K. J. KAZAKOS, A. SMYRNIS, K. C. XARCHAS, A. DIMITRAKOPOULOU, D.-A. VERETTAS
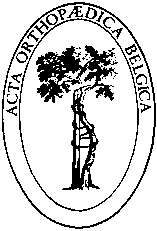
Fig. 1a and b. — Anastomosis (arrows) between the two nerves arising from the median nerve itself (Type II). UA : Ulnar artery, MN : Median nerve, A : Anastomosis, UN : Ulnar nerve.
described a branch coursing from the ulnar nerve
narrower range of incidence between 10% and
proximally to the median nerve distally. This anas-
tomosis is referred to as the Martin – Gruber anas-
These anastomoses may cause confusion in the
tomosis (MGA). It involves axons leaving either
diagnosis of conditions affecting the nerve supply
the main trunk of the median nerve or the anterior
to the intrinsic muscles of the hand. The crossing
interosseous nerve, crossing through the forearm to
axons may innervate intrinsic muscles supplied by
join the main trunk of the ulnar nerve and ultimate-
the ulnar nerve, the median nerve or both.
ly innervating the intrinsic hand muscles. This vari-ation has been reported to occur in as many as 15-
Table I. — Distribution of the anastomoses between the
31% of subjects (12, 29). Most often the anomalous
median and ulnar nerve in the forearm, related to sex and
axons innervate the first dorsal interosseous muscle
and less often the hypothenar and thenar mus-
cles (8). Its reported incidence differs between
physiologic and anatomic studies. In the former it
has been described as occurring in 5-40% ofcases
(12, 8, 4, 27) whereas anatomic studies report a
Acta Orthopædica Belgica, Vol. 71 - 1 - 2005
ANASTOMOSIS BETWEEN THE MEDIAN AND ULNAR NERVE IN THE FOREARM
Fig. 2a and b. — Anastomosis (arrows) between the two nerves arising from the anterior interosseous nerve (Type III). UA : Ulnar artery, MN : Median nerve, A : Anastomosis, UN : Ulnar nerve, AIN : Anterior interosseous nerve, FDS : Flexor digitorum superfi- cialis muscles.
Depending on the level of the nerve injury, an
MATERIAL AND METHODS
increased or decreased motor deficit of the intrinsichand muscles can be detected. The knowledge of
One hundred fresh frozen cadavers were dissected in
these anastomoses and the resulting anomalous
the morgue of Athens during a time period of three
innervation patterns is of major importance for
years. From these, 53 belonged to males and 47 tofemales. Sixty-three cadavers (30 male and 33 female)
assessment of traumatic or entrapment lesions of
were studied bilaterally and 37 (23 male and 14 female)
the median and ulnar nerve (11, 28).
unilaterally. In total, 163 forearms were dissected. The
The purpose of our research was to determine
age of cadavers ranged from 25 to 91 years.
the incidence and also the types of this anastomo-
An ‘S’ shaped incision was carried out, covering the
sis in the Greek population and compare our results
whole anterior surface of the forearm. The superficial
to those of similar previous studies. The findings
fascia was opened and the flexor carpi ulnaris muscle
and literature review are presented, to guide the
and tendon mobilised to give full exposure of the ulnar
hand surgeon when dealing with forearms with a
artery and ulnar nerve. The branches of the ulnar nerve
in the forearm were dissected and all possible anasto-
Acta Orthopædica Belgica, Vol. 71 - 1 - 2005
K. J. KAZAKOS, A. SMYRNIS, K. C. XARCHAS, A. DIMITRAKOPOULOU, D.-A. VERETTAS
moses between median and ulnar nerves were docu-
sex and presence or absence of the anastomosis in
mented. The level at which the connections joined the
the right forearm according to the Pearson test,
median and ulnar nerves was measured using the medi-
gave the following data : X2 = 0.11 and p = 0.73 ;
al epicondyle of the humerus as reference (point 0). The
b) the same cross – correlation for the left forearm
research was made with the use of magnifying glasses
gave the following values : X2 = 4.27 and p =
0.038 (table I). This confirms that absence of the
Statistical comparisons were performed in the depart-
anastomosis in the left forearm is more rare in
ment of statistics in the National School of Public Healthof Athens using the chi-squared test. P < 0.05 was
females than in males, or else that the anastomosis
regarded as statistically significant.
in the left forearm is 1.2 times more frequent infemales than in males. DISCUSSION
nerve were found in 10 out of 100 samples of
Anastomoses between median and ulnar nerves
cadavers, which were studied. It occurred in 7 of
in the forearm are of phylogenetic significance (2).
the 53 male cadavers (3 bilateral and 4 only in the
In many mammals and frequently in primates there
right forearm) and in 3 of the 47 female cadavers
are similar connections between the median and
(1 bilateral and 2 only in the left forearm).
ulnar nerve at or below the elbow. Anastomoses
Therefore, the anastomosis between the two nerves
could be remnants of the common ventral nerve
was found in 14 of the 163 forearms, which were
trunk innervating flexor muscles in the upper
dissected (table I). The incidence in the male fore-
extremity, which is noted in the early stages of evo-
arms was 14% and 6.5% in the female forearms.
lution. Anastomoses occur frequently in humans
These anastomoses were classified into three types
and are therefore considered a variation rather than
depending on the level of origin of the anastomosis
from the median nerve. Type I originates from the
It has been estimated that in the forearms of 15%
branch of the median nerve to the superficial fore-
to 31% of individuals, motor axons descend from
arm flexor muscles, Type II from the median nerve
the median nerve, crossing to the ulnar nerve, and
itself (fig 1) and Type III from the anterior
ultimately innervating intrinsic hand muscles
interosseous nerve (fig 2). Type I occurred in one
which are normally supplied by the ulnar nerve (12,
case (n = 1-7%), type II occurred in one case (n =
29). This anastomosis gives rise to changes in motor
1-7%) and type III occurred in 12 cases (n = 12-
conduction studies, identifying its presence. When
87%) and the branch passed medially to join the
this anastomosis exists in a patient with carpal tun-
ulnar nerve in either its upper or middle one-third.
nel syndrome, it may result in unusual findings in
The average length of the anastomosis was
6.4 cm. Its origin was on average 6.8 cm distal to
There is no consensus in the literature about the
the medial epicondyle, and its connection to the
classification of anastomosis between the two
ulnar nerve was on average 11.0 cm distal to the
nerves. Numerous classifications have been
medial epicondyle. The anastomosis joined the
proposed by Nakashima (14), Hirasawa (9),
ulnar nerve as a single branch in twelve cases and
Thomson (25), Shu et al (21), Srinivasan and Rhodes
split into two branches in two cases. The superior
(22) and Rodriguez-Niedenfuhr et al (17) ; their clas-
branch had a recurrent course and the inferior one
sifications were based on anatomical dissections.
ran downwards. Anastomoses between ulnar nerve
Uchida and Sugioka (26), Oh et al (15) and Kimura
proximally to the median nerve distally were not
et al (11) proposed classifications based on electro-
found out, nor were anastomoses between these
physiological examinations and Shu (21) proposed
another classification based on histological exami-
With regard to the analysis of frequency the fol-
nations. A summary of these classification schemes
lowing were found : a) Cross – correlation between
Acta Orthopædica Belgica, Vol. 71 - 1 - 2005
ANASTOMOSIS BETWEEN THE MEDIAN AND ULNAR NERVE IN THE FOREARM
Table II. — Classifications of anastomosis between the median and ulnar nerves.(Abbreviation : MN : median nerve, UN : ulnar
nerve, AIN : anterior interosseous nerve, TM : thenar muscles, HM : hypothenar muscles, FDP : flexor digitorum profundus mus-
Anastomosis Hirasawa Srinivasan Nakashima Rodriguez Uchida (20) Kimura (1)
muscular branchesFDP muscleoriginated fromthe connection
The incidence of anastomosis between the two
with carpal tunnel syndrome (CTS) and from 15%
nerves in earlier reports was 15.2% according to
to 39% in either normal or unselected subjects.
Gruber (6), 15.5% according to Thomson (25),
Uchida and Sugioka (26) determined the incidence
10.5% according to Hirasawa (9), 15.5% according
of anastomosis in patients without and with cubital
to Mannerfelt (12), 23% according to Taams (24),
tunnel syndrome and found an incidence of 16% in
21.3% according to Nakashima (14), 13.1% accord-
the normal controls and 17% in the cubital tunnel
ing to Rodriguez-Niedenfuhr et al (17).
syndrome group. In other electrodiagnostic studies
Mannerfelt (12) was the first to use electrodiag-
the highest incidence of the anastomosis was found
nostic techniques to detect anastomosis between
for the first dorsal interosseous muscle (FDI).
the two nerves and reported a 15% incidence in a
Wilbourn and Lambert (29) reported that anomalous
study of 41 patients. Crutchfield and Gutmann (4)
axons innervate the FDI muscle much more com-
found an incidence of 28% in the general popula-
monly (95%) than the hypothenar (41%) and thenar
tion and 62% in 29 relatives of 5 subjects with
muscles (14%). In 22 limbs showing the anastomo-
anastomosis. Several other authors, using electro-
sis in our study, the anastomotic median axons
diagnostic techniques, have reported incidences of
innervated the FDI area 21 times, hypothenar mus-
anastomosis ranging from 8% to 26% in patients
cles in 9 cases and thenar muscles in 3 cases.
Acta Orthopædica Belgica, Vol. 71 - 1 - 2005
K. J. KAZAKOS, A. SMYRNIS, K. C. XARCHAS, A. DIMITRAKOPOULOU, D.-A. VERETTAS
Kimura et al (11) studied 656 arms of 328 subjects
It has been suggested that unilateral anastomosis
using electrophysiological methods and found ana-
between the two nerves occurs more often on the
stomosis in 57 (17%) subjects and 96 arms (15%).
right side than on the left (24). In our study anasto-
The incidence of anastomosis in our study was 8.6%.
moses were also found mainly on the right side in
We used the classification of patterns and
anatomical examination (four against two).
types (18) to compare our results to those of previ-
Crutchfield and Gutmann (4) and Piza-Katzer (16)
ous reports. Pattern I comprises cases with one
found median-ulnar nerve communication in the
anastomotic branch, and Pattern II those with two
family members of persons who showed this
anastomotic branches. Types a, b, and c are subdi-
anomalous connection, and suggested that there is
visions depending on the level of origin of the
familiar inheritance, probably autosomal dominant.
anastomosis from the median nerve. Type a origi-
In the present study, we did not study familiar
nates from the branch of the median nerve to the
superficial forearm flexor muscles. Type b origi-
Occurrence frequency for ulnar to median nerve
nates from the median nerve itself and Type c from
communication was reported as 5% by Rosen (19)
the anterior interosseous nerve. Our results confirm
and 16.7% by Golovchinsky (5). In the present
that the anastomosis appears as one branch with
study, we did not find any ulnar to median com-
various origins from the median nerve or its
branches, as already described by Thomson (25),
No statistically significant difference was found
Srinivasan and Rhodes (22) and Taams (24) (table III).
between men and women regarding the frequency
Intramuscular anastomosis has also been describ-
of these anastomoses. This was an expected result,
ed (14, 17), but we found no such anastomosis
in view of earlier analyses, which indicated auto-
despite the use of magnification during dissection.
somal dominant inheritance of these innervation
The course of the anastomosis has been more
frequently described as transverse or oblique than
There is now electrophysiological evidence that
arched (6, 9). We found that the transverse or
median – ulnar nerve anastomoses convey motor
oblique course depended on whether the anasto-
fibers from the median to the ulnar nerve in the
motic end at the ulnar nerve was in the superior or
forearm for innervation of the intrinsic muscles in
the hand (7, 10). These electrophysiological findings
At its termination, the anastomosis has been
indicate that there is motor communication from
recorded either as a single branch or as a single
the median to the ulnar nerve in the forearm.
branch which divided into two branches, one with
Median nerve stimulation at the elbow evoked not
an oblique course and the other with a recurrent
only muscle action potentials (MAP) from the
course (9). Like Gruber (6), we found a single con-
thenar muscles, but also from the hypothenar and
nection more frequently than a double one.
the first dorsal interosseous muscles.
Table III. — Patterns and types of anastomosis shown by different authors
Pattern I Pattern II
Acta Orthopædica Belgica, Vol. 71 - 1 - 2005
ANASTOMOSIS BETWEEN THE MEDIAN AND ULNAR NERVE IN THE FOREARM
It is therefore clear that the anastomoses
12. Mannerfelt L. Studies on the hand in ulnar nerve paraly-
between median and ulnar nerves are clinically
sis. A clinical-experimental investigation in normal and
relevant. These connections are often suggested as
anomalous innervation. Acta Orthop Scand 1966 : Suppl87 part 2 : 19-29.
causes for unusual motor losses of the muscles in
13. Martin R. Tal om nervus allmanna Egenskaperi
the hand after peripheral nerve lesions (3, 20).
Mannisikans Kropp. Las Salvius 1763.
Symptoms of carpal tunnel syndrome with co-exis-
14. Nakashima T. An anatomic study on the Martin-Gruber
tence of this anastomosis may be incomplete
anastomosis. Surg Radiol Anat 1993 ; 15 : 193-195.
because of proper functionality of thenar mus-
15. Oh SJ, Claussen GC, Ahmad BK. Double anastomosis
of median-ulnar and ulnar-median nerves : report of an
cles (10). By recognising the existence of different
electrophysiologically proven case. Muscle Nerve 1995 ;
types of anastomosis, mistakes in the diagnosis of
peripheral nerve lesions or compression neuro-
16. Piza-Katzer H. [Familial occurence of Martin-Gruber
pathies in the forearm can be avoided (1, 28).
anastomosis]. Handchirurgie 1976 ; 8 : 215-218. 17. Rodriguez-Niedenfuhr M, Vazquez T, Parkin I, REFERENCES Logan B, Sanudo JR. Martin-Gruber anastomosis revisit- ed. Clin Anat 2002 ; 15 : 129-134. 18. Rodriguez-Niedenfuhr M, Vazquez T, Ferreira B, 1. Bergman FO, Blom SE, Stenstrom SJ. Radical excision Parkin I, Nearn L, Sanudo JR. Intramuscular Martin-
of a fibro-fatty proliferation of the median nerve, with no
Gruber anastomosis. Clin Anat 2002 ; 15 : 135-138.
neurological loss symptoms. Plast Reconstr Surg 1970 ;
19. Rosen AD. Innervation of the hand : an electromyographic
study. Electromyogr Clin Neurophysiol 1973 ; 13 : 175-
2. Bunnell S. Surgery of the Hand. 3rd ed. JB Lippincott, 20. Rowntree T. Anomalous innervation of the hand muscles. 3. Cliffton E. Unusual innervation of the intrinsic muscles of J Bone Joint Surg 1949 ; 31-B : 505 - 510.
the hand by median and ulnar nerve. Surgery 1948 ; 23 :
21. Shu H, Chantelot C, Oberlin C, Alnot JY, Shao H.
[Anatomic study and review of the literature on the Martin
4. Crutchfield CA, Gutmann L. Hereditary aspects of
Gruber anastomosis]. Morphologie 1999 ; 83 : 71-74.
median-ulnar nerve communications. J Neurol Neurosurg22. Srinivasan R, Rhodes J. The median-ulnar anastomosis Psychiatry 1980 ; 43 : 53-55.
(Martin-Gruber) in normal and congenitally abnormal
5. Golovchinsky V. Frequency of ulnar-to-median nerve
fetuses. Arch Neurol 1981 ; 38 : 418-419.
anastomosis revisited. Electromyogr Clin Neurophysiol23. Streib EW. Ulnar-to-median nerve anastomosis in the
forearm : electromyographic studies. Neurology 1979 ;
6. Gruber W. Uber die Verbindung Des Nervus medianus
mit dem Nervus ulnaris am Unterarme des Menschen und
24. Taams KO. Martin-Gruber connections in South Africa.
der Saugethiere. Arch Anat Physiol Wissen Med 1870 ;
An anatomical study. J Hand Surg 1997 ; 22-B : 328-330. 25. Thomson A. Third annual report of the Committee of 7. Gutmann L. Median - ulnar nerve communications and
Collective Investigations of the Anatomical Society of
carpal tunnel syndrome. J Neurol Neurosurg Psychiatry
Great Britain and Ireland for the years 1891-1892. J Anat8. Gutmann L. AAEM minimonograph #2 : important 26. Uchida Y, Sugioka Y. Electrodiagnosis of Martin-Gruber
anomalous innervations of the extremities. Muscle Nerve
connection and its clinical importance in peripheral nerve
surgery. J Hand Surg 1992 ; 17-A : 54-59. 9. Hirasawa K. Untersuchungen uber das periphere Nerven- 27. Van Dijk JG, Bouma PA. Recognition of the Martin-
system, Plexus brachialis und die Nerven der oberen
Gruber anastomosis. Muscle Nerve 1997 ; 20 : 887-889.
Extremität. Arb Anat Inst Kaiserlichen Univ Kyoto 1931 ;
28. Van Tieghem J, Vandendriessche G, Vanhecke J.
Martin-Gruber anastomosis : the explanation for late diag-
10. Iyer V, Fenichel GM. Normal median nerve proximal
nosis of severe ulnar nerve lesions at the elbow. Electro-
latency in carpal tunnel syndrome : a clue to coexisting
myogr Clin Neurophysiol 1987 ; 27 : 13-18.
Martin-Gruber anastomosis. J Neurol Neurosurg Psychia-29. Wilbourn AJ, Lambert EH. The forearm median to ulnar
nerve communication : electrodiagnostic aspects. Neurolo-11. Kimura J, Murphy MJ, Varda DJ. Electrophysiological
study of anomalous innervation of intrinsic hand muscles. Arch Neurol 1976 ; 33 : 842-844.
Acta Orthopædica Belgica, Vol. 71 - 1 - 2005
SCHEDA INFORMATIVA INTERVENTO DI VITRECTOMIA PER RETINOPATIA DIABETICA Approvata dalla Società Oftalmologica Italiana - Anno 2003 Gentile Signora, Signore, Lei soffre di una patologia responsabile di un calo alla vista e di altre possibili e gravi complicanze. Questa scheda contiene le informazioni sul trattamento che Le è proposto, sui risultati e sui rischi. Tutte le espression
 Acta Orthop. Belg., 2005, 71, 29-35
Acta Orthop. Belg., 2005, 71, 29-35
 K. J. KAZAKOS, A. SMYRNIS, K. C. XARCHAS, A. DIMITRAKOPOULOU, D.-A. VERETTAS
Fig. 1a and b. — Anastomosis (arrows) between the two nerves arising from the median nerve itself (Type II). UA : Ulnar artery,
K. J. KAZAKOS, A. SMYRNIS, K. C. XARCHAS, A. DIMITRAKOPOULOU, D.-A. VERETTAS
Fig. 1a and b. — Anastomosis (arrows) between the two nerves arising from the median nerve itself (Type II). UA : Ulnar artery,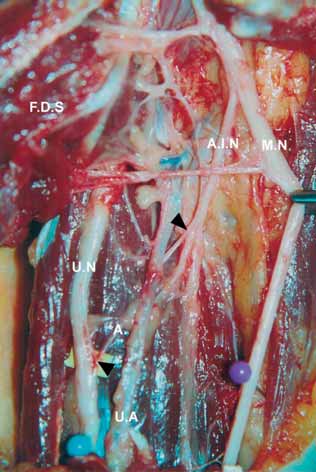
 ANASTOMOSIS BETWEEN THE MEDIAN AND ULNAR NERVE IN THE FOREARM
Fig. 2a and b. — Anastomosis (arrows) between the two nerves arising from the anterior interosseous nerve (Type III). UA : Ulnar
ANASTOMOSIS BETWEEN THE MEDIAN AND ULNAR NERVE IN THE FOREARM
Fig. 2a and b. — Anastomosis (arrows) between the two nerves arising from the anterior interosseous nerve (Type III). UA : Ulnar